Bone as an organ. Development structure growth classification of bones
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed to compose a thorough, well-illustrated answer. Let me deliver it.
Bone as an Organ: Development, Structure, Growth, and Classification
1. Bone as an Organ - Overview
Bone is a calcified, living connective tissue forming the majority of the skeleton. It consists of a mineralized intercellular matrix containing collagen fibers, and several distinct cell types embedded within. As an organ, bone performs five major functions:
- Structural support for the body
- Protection of vital organs (brain, heart, lungs)
- Reservoir for calcium and phosphorus (metabolic function)
- Lever system on which muscles act to produce movement
- Container for blood-producing cells (hematopoiesis)
Bone is vascular and innervated. An adjacent artery typically gives off one nutrient artery per bone, supplying the marrow, spongy bone, and inner compact bone. The entire external surface (except articular surfaces) is covered by the periosteum, a fibrous membrane capable of forming new bone. Stripping the periosteum causes bone death. The periosteum is richly supplied with sensory nerve fibers and is exquisitely sensitive to injury - this explains much of the pain from fractures and periostitis.
- Gray's Anatomy for Students, p. 30
2. Classification of Bones
By Shape (Macroscopic)
| Type | Description | Example |
|---|---|---|
| Long | Tubular; length > width | Humerus, femur, tibia |
| Short | Cuboidal; approximately equal dimensions | Carpals, tarsals |
| Flat | Two compact plates separated by spongy bone | Skull, ribs, sternum |
| Irregular | Complex shapes not fitting other categories | Vertebrae, facial bones |
| Sesamoid | Round/oval, develop within tendons | Patella, sesamoids of thumb/great toe |
Sesamoid and accessory bones are normal variants, commonly in the wrist, hands, ankles, and feet. They must not be confused with fractures on imaging.
- Gray's Anatomy for Students, p. 30
3. Structure of Bone
Macroscopic Structure
Bones have two gross structural types:
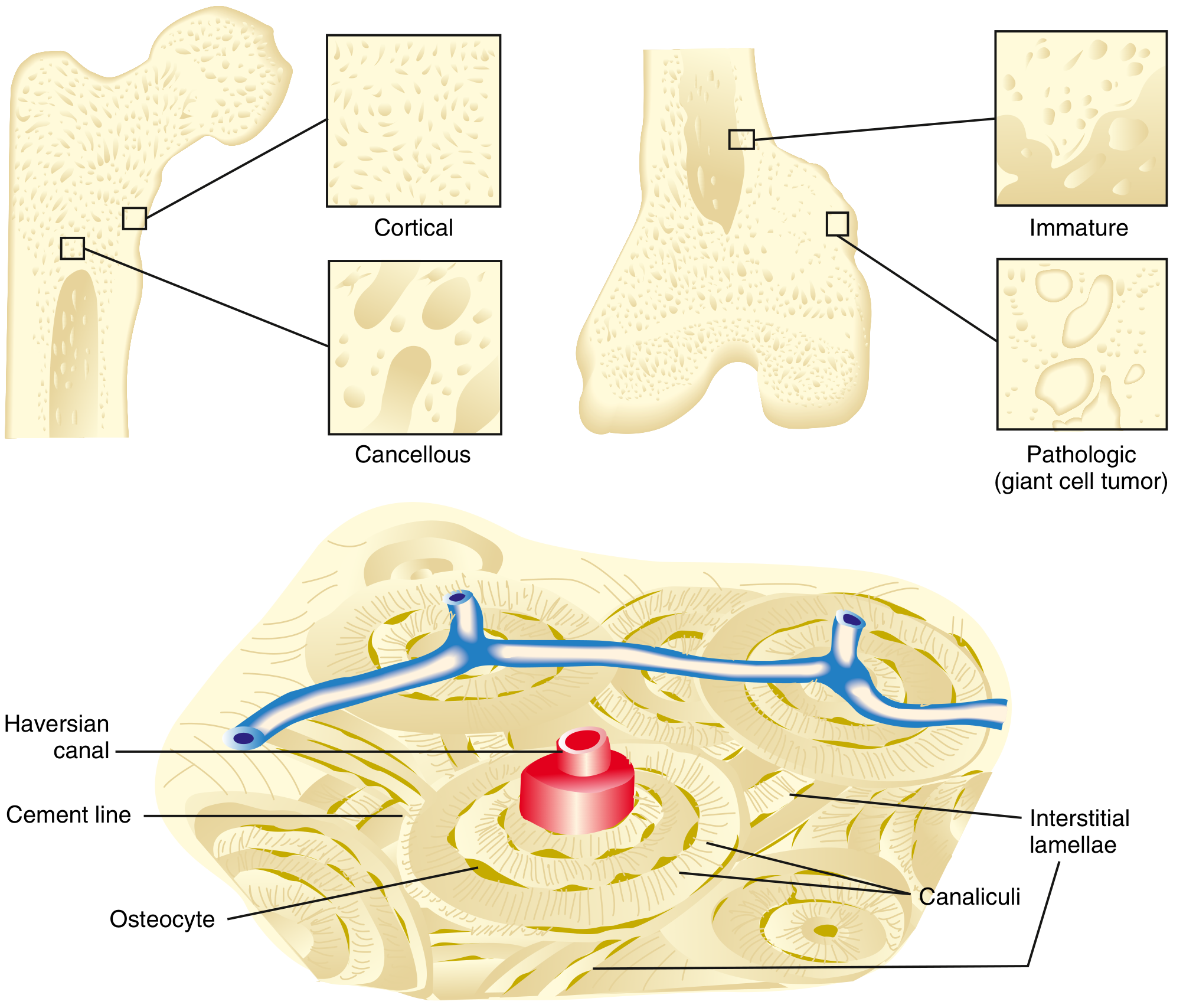
Compact (Cortical) Bone
- Makes up ~80% of the skeleton
- Forms the outer shell of all bones
- Characterized by slow turnover rate and high Young's modulus (stiffness)
- Consists of tightly packed osteons (Haversian systems):
- Each osteon = a central Haversian canal (containing arterioles, venules, capillaries, nerves) surrounded by concentric rings of bone (lamellae)
- Cement lines define the outer border of an osteon
- Interstitial lamellae fill spaces between osteons
- Haversian canals connect longitudinally; Volkmann's canals run transversely, connecting Haversian canals to each other and to the periosteum
- Nutrition delivered through canaliculi - tiny channels containing osteocyte cell processes
Cancellous (Spongy/Trabecular) Bone
- Makes up ~20% of the skeleton
- Found in epiphyses and inner surfaces of flat bones
- Loose network of struts and plates (trabeculae) aligned along lines of stress
- 30-90% of pores filled with bone marrow
- Higher turnover rate, smaller Young's modulus, more elasticity than cortical bone
Microscopic Classification
| Type | Characteristics | When Seen |
|---|---|---|
| Lamellar | Organized, stress-oriented lamellae; secondary bone formed by remodeling of woven bone; stronger; less flexible | Normal mature bone |
| Woven | Random collagen orientation; not stress-oriented; more osteocytes per unit area; higher turnover; weaker and more flexible | Embryonic skeleton, fracture callus, pathologic states (Paget, tumors) |
- Miller's Review of Orthopaedics 9e, p. 20-21
4. Cellular Biology of Bone
Three principal cell types maintain bone:
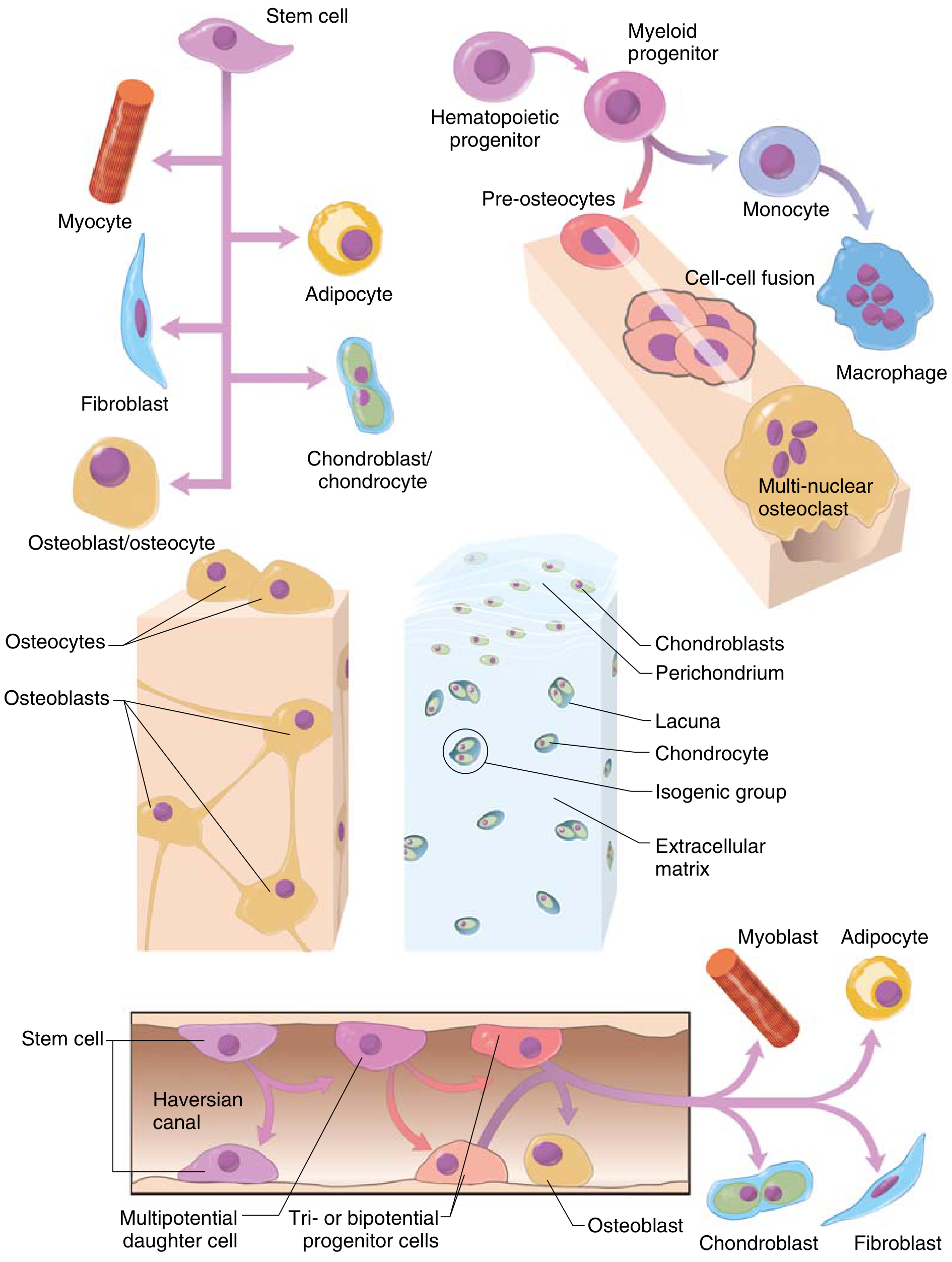
Osteoblasts
- Derived from mesenchymal stem cells (MSCs) lining Haversian canals, endosteum, and periosteum
- Key transcription factors: RUNX2 and BMP (bone morphogenetic protein) direct MSC differentiation toward the osteoblast lineage
- Appear as cuboidal cells aligned along osteoid surfaces
- Rich in endoplasmic reticulum, Golgi, and mitochondria (for matrix synthesis)
- Products: type I collagen (90% of organic matrix), alkaline phosphatase, osteocalcin, bone sialoprotein, RANKL, and osteoprotegerin (OPG)
- Under conditions of low strain + increased O₂ tension → differentiate to osteoblasts
- Under intermediate strain + low O₂ → differentiate to cartilage (chondrocytes)
- Under high strain → differentiate to fibrous tissue
Osteocytes
- Entrapped former osteoblasts residing in lacunae
- Maintain the ionic milieu of bone
- Less metabolically active; communicate via canalicular cell processes
- Disruption of active lining cell layer activates entrapped osteocytes
Osteoclasts
- Derived from hematopoietic precursors (monocyte-macrophage lineage) - fuse to form multinucleated giant cells
- Regulated by the RANK/RANKL/OPG axis:
- Osteoblasts produce RANKL → binds RANK on osteoclast precursors → stimulates osteoclast differentiation
- Osteoblasts also produce OPG → decoy receptor that neutralizes RANKL → limits osteoclast activity
- Possess a ruffled (brush) border that increases membrane surface area for resorption
- Bind to bone via integrin (αvβ3/vitronectin receptor)
- Resorb bone at Howship lacunae by:
- Producing H⁺ via carbonic anhydrase → lowers pH → dissolves hydroxyapatite
- Releasing cathepsin K → proteolytic digestion of organic matrix
- Produce tartrate-resistant acid phosphatase (TRAP) - a histochemical marker
- Regulated by: calcitonin (inhibits), IL-1 (stimulates), IL-10 (inhibits)
Bone Matrix
Organic component (40% of dry weight):
- Collagen 90% - primarily type I collagen (mnemonic: "bone" contains "one"); provides tensile strength
- Proteoglycans - provide compressive strength; prevent premature mineralization
- Non-collagenous proteins: osteocalcin (most abundant; marker of bone turnover), bone sialoprotein, osteopontin, fibronectin
Inorganic component (60% of dry weight):
-
Primarily hydroxyapatite [Ca₁₀(PO₄)₆(OH)₂]
-
Mineral deposition occurs in the "hole zones" and "pores" of collagen fibrils
-
Miller's Review of Orthopaedics 9e, p. 22-24
5. Development of Bone (Ossification)
There are three mechanisms of bone formation:
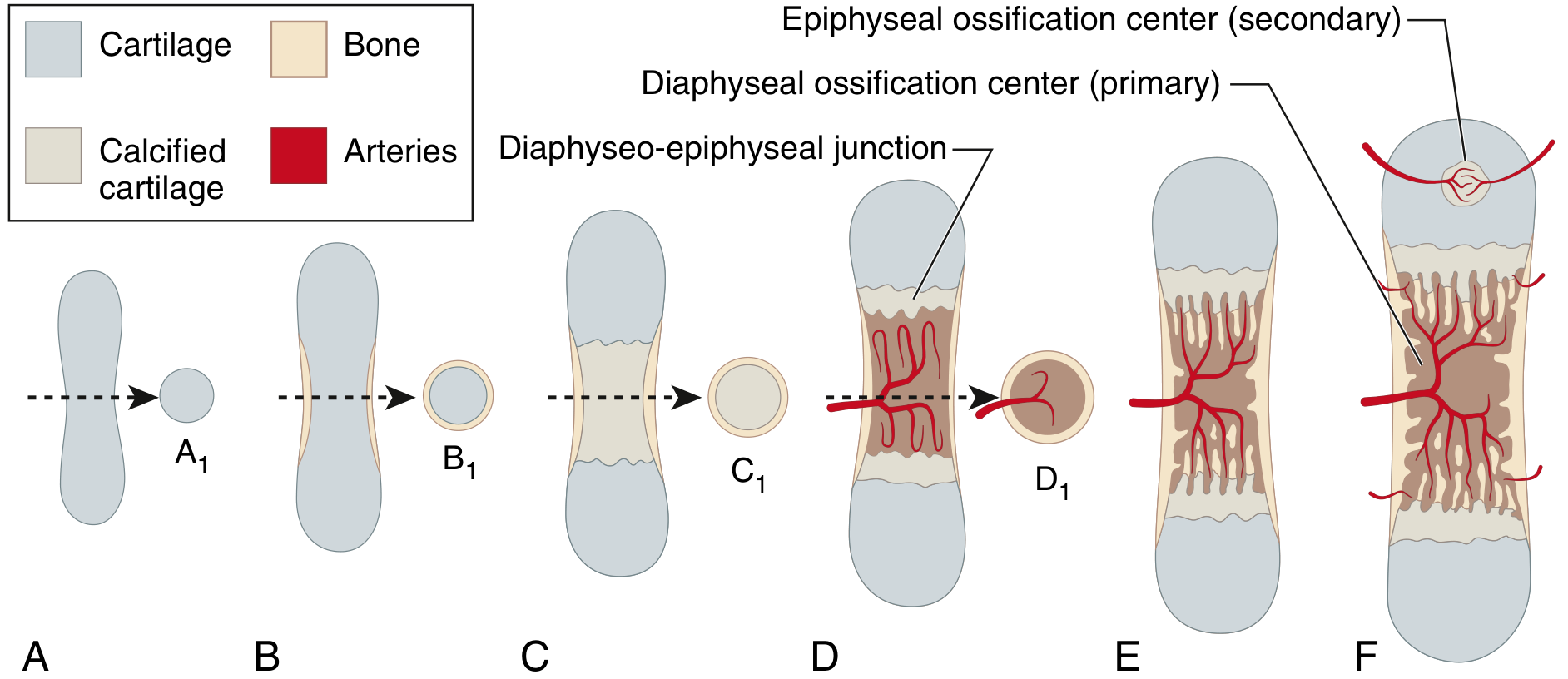
A. Endochondral Ossification
Bone replaces a pre-existing cartilage model. This is the mechanism for most bones of the body.
Normal examples: Embryonic formation of long bones; longitudinal growth at the physis; fracture callus; bone formed with demineralized bone matrix
Embryonic Formation of Long Bones (sequence):
- At ~6 weeks' gestation, mesenchymal cells in the limb bud differentiate into chondroblasts, forming a hyaline cartilage model (the skeletal anlage)
- A bone collar forms around the mid-shaft as periosteal osteoblasts lay down woven bone (intramembranous component)
- At ~8 weeks, vascular buds invade the central cartilage, bringing osteoprogenitor cells that differentiate into osteoblasts → primary ossification center forms in the diaphysis
- The central cartilage is resorbed by osteoclasts and replaced by bone/marrow
- Secondary ossification centers develop postnatally at the bone ends (epiphyses), driven by separate vascular invasion
- The cartilage sandwiched between the primary and secondary centers becomes the physis (growth plate)
B. Intramembranous Ossification
Aggregates of undifferentiated mesenchymal cells differentiate directly into osteoblasts - no cartilage intermediate.
Normal examples: Embryonic flat bone formation (skull, clavicle, mandible); bone formation during distraction osteogenesis; blastema bone
Disease: Cleidocranial dysostosis (defect in RUNX2) impairs intramembranous ossification
C. Appositional Ossification
Osteoblasts lay down new bone on existing bone surfaces.
Normal examples: Periosteal bone enlargement (increases bone width); the bone formation phase of remodeling
Diseases: Paget disease, infantile hyperostosis (Caffey disease), melorheostosis
- Miller's Review of Orthopaedics 9e, p. 26-27
6. Growth of Bone
The Physis (Growth Plate) - Longitudinal Growth
Two types of growth plates exist in immature long bones:
- Horizontal physis - responsible for longitudinal growth
- Spherical physis - located at the epiphyseal periphery; less organized
The physis is organized into four distinct zones from epiphysis toward metaphysis:
| Zone | Key Events | Clinical Significance |
|---|---|---|
| Reserve (Resting) zone | Cells store lipids, glycogen, proteoglycan aggregates; low O₂ tension | Lysosomal storage diseases (Gaucher disease) affect this zone |
| Proliferative zone | Longitudinal stacking of chondrocytes ("column of coins"); active cellular proliferation and matrix production; increased O₂ | Growth hormone acts here; achondroplasia = FGFR3 mutation impairing this zone |
| Hypertrophic zone (3 sub-zones): | ||
| - Maturation | Chondrocytes increase 5× in size; accumulate Ca²⁺ in mitochondria | PTH-related peptide (PTHrP) inhibits maturation; Indian hedgehog protein regulates PTHrP |
| - Degeneration | Chondrocytes die; release Ca²⁺ from matrix vesicles | Mucopolysaccharide diseases cause degeneration here |
| - Provisional calcification | Type X collagen enables mineralization; low O₂ and decreased proteoglycans aid calcification | Rickets causes widening of this zone (no provisional calcification); SCFE occurs here |
Osteoblasts then migrate from sinusoidal metaphyseal vessels and use the calcified cartilage as scaffolding to deposit bone.
Hormonal regulation of the physis:
- Growth hormone - acts in the proliferative zone
- PTHrP - inhibits chondrocyte maturation (keeps cells in proliferative phase)
- Indian hedgehog (Ihh) - produced by hypertrophic chondrocytes; regulates PTHrP
- Thyroid hormone - stimulates hypertrophic differentiation
- Estrogen/testosterone - stimulate physeal closure at the end of puberty
Appositional Growth (Width)
Periosteal osteoblasts lay down new bone on the outer surface, increasing bone diameter. Simultaneously, endosteal osteoclasts resorb the inner surface to enlarge the medullary cavity.
Bone Remodeling
Bone is continuously remodeled throughout life, replacing old bone with new bone in discrete packets via the basic multicellular unit (BMU):
-
Activation → Resorption (osteoclasts) → Reversal → Formation (osteoblasts) → Quiescence
-
Regulated by: PTH (stimulates resorption indirectly via osteoclasts), calcitonin (inhibits osteoclasts), vitamin D (stimulates Ca²⁺ absorption and bone mineralization), mechanical stress
-
Miller's Review of Orthopaedics 9e, p. 27-28; Junqueira's Basic Histology 17e, p. 402
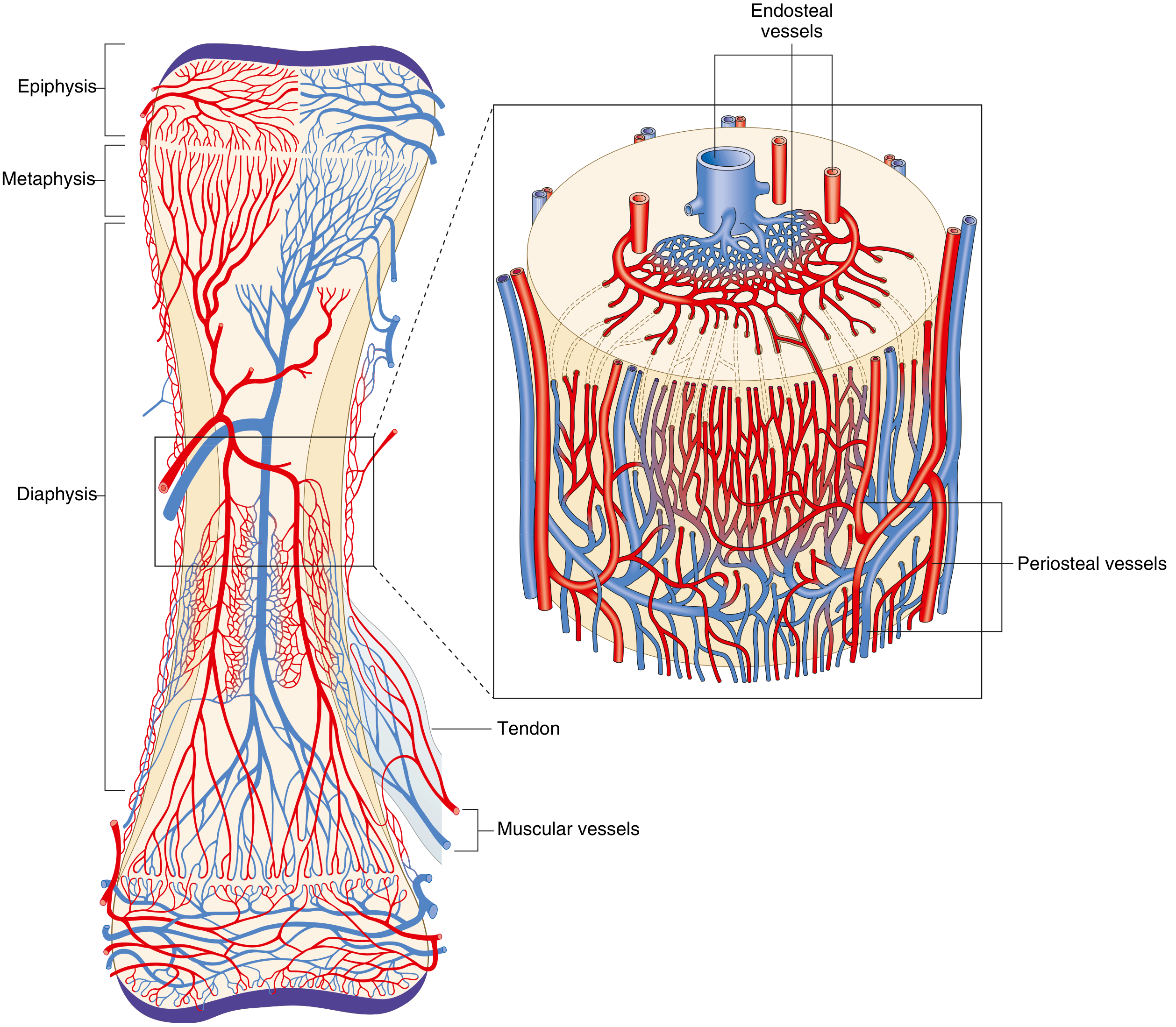
7. Blood Supply of Bone
Long bones receive blood from three systems:
| System | Characteristics |
|---|---|
| Nutrient artery system | High pressure; supplies 60% of cortical bone; enters through nutrient foramen → branches into ascending and descending arteries → arterioles supply inner 2/3 of cortex via Haversian system |
| Metaphyseal-epiphyseal system | Arises from periarticular vascular plexus (e.g., geniculate arteries) |
| Periosteal system | Low pressure; supplies outer 1/3 of cortex; capillaries from periosteal vessels |
Direction of flow: In mature bone, arterial flow is centrifugal (inside → outside) due to high-pressure nutrient system dominance. Venous flow is centripetal (outside → inside). When the nutrient artery is disrupted (fracture) or in immature bone, periosteal pressure dominates and flow reverses to centripetal.
8. Metabolic Role of Bone
Bone is the body's primary calcium reservoir:
- Storage: When dietary calcium is adequate, calcium is deposited into bone matrix as hydroxyapatite
- Mobilization: When dietary calcium is deficient, PTH stimulates osteoclasts to resorb bone and release Ca²⁺
- Regulation: PTH indirectly stimulates osteoclasts (via RANKL on osteoblasts) → raises serum Ca²⁺. Calcitonin inhibits osteoclast activity → lowers serum Ca²⁺. Vitamin D (1,25-(OH)₂D₃) enhances intestinal Ca²⁺ absorption and is needed for normal matrix mineralization.
Deficiency states:
-
Vitamin D/Ca²⁺ deficiency in children → Rickets (widened hypertrophic zone, bowing of long bones)
-
Same deficiency in adults → Osteomalacia (unmineralized osteoid accumulates)
-
Vitamin A deficiency → suppresses endochondral bone growth
-
Vitamin C deficiency → impairs collagen synthesis → scurvy
-
Histology: A Text and Atlas (Pawlina), p. 622-623; Junqueira's Basic Histology 17e, p. 400-401
Summary Table
| Topic | Key Points |
|---|---|
| Functions | Support, protection, mineral reservoir, movement, hematopoiesis |
| Classification by shape | Long, short, flat, irregular, sesamoid |
| Microscopic types | Woven (immature/pathologic) vs. lamellar (mature/normal) |
| Macroscopic types | Cortical (compact, 80%) vs. cancellous (trabecular, 20%) |
| Structural unit | Osteon (Haversian system) in cortical bone; trabeculae in cancellous bone |
| Cells | Osteoblast (forms), osteocyte (maintains), osteoclast (resorbs) |
| Ossification | Endochondral (long bones), intramembranous (flat bones), appositional (width) |
| Physeal zones | Reserve → Proliferative (GH acts here) → Hypertrophic (PTHrP/Ihh) → Provisional calcification |
| Growth regulators | GH, PTHrP, Ihh, thyroid hormone, sex steroids, mechanical stress |
| Matrix | 40% organic (type I collagen 90% + proteoglycans + NCPs) + 60% inorganic (hydroxyapatite) |
Sources: Miller's Review of Orthopaedics 9e | Gray's Anatomy for Students | Junqueira's Basic Histology 17e | Histology: A Text and Atlas (Pawlina)
This is a shared conversation. Sign in to Orris to start your own chat.