I now have all four Dejour types illustrated, the TT-TG diagram, and the Schottle's point MPFL images. I have comprehensive textbook content from Campbell's, Rockwood & Green's, Miller's, and Rosen's, plus the latest 2024-2026 evidence. Let me now compose the full, detailed, well-illustrated answer.
Patellar Instability and Patellar Dislocations: A Complete Clinical Guide
SECTION 1 — ANATOMY AND STABILIZERS OF THE PATELLOFEMORAL JOINT
The patella sits within the femoral trochlear groove and is stabilized by a combination of bony and soft tissue restraints. Understanding these is essential to understanding why instability occurs.
Bony Stabilizers
- The lateral trochlear facet is normally taller and more prominent than the medial, creating a "wall" that resists lateral patellar displacement
- The patella engages the trochlea at approximately 20-30° of knee flexion - below this arc, soft tissues provide primary restraint
- Any trochlear shallowness (dysplasia) eliminates this bony containment
Soft Tissue Stabilizers
| Structure | Role |
|---|
| MPFL (Medial Patellofemoral Ligament) | Primary medial restraint - provides ~50-60% of resistance to lateral translation. Runs from superomedial patella to medial femoral epicondyle (Schottle's point). Ruptured in >90% of acute dislocations |
| VMO (Vastus Medialis Obliquus) | Active dynamic medial stabilizer; weakness allows lateral subluxation |
| Lateral retinaculum | Normally thicker than medial; excessive tightness contributes to patellar tilt and lateral tracking |
| Patellotibial and patellomeniscal ligaments | Secondary distal restraints |
Key Biomechanical Measurements
| Measurement | Normal Values | Significance |
|---|
| Q angle | <15° (male), <20° (female) | Represents lateralizing force vector; increased with femoral anteversion/genu valgum |
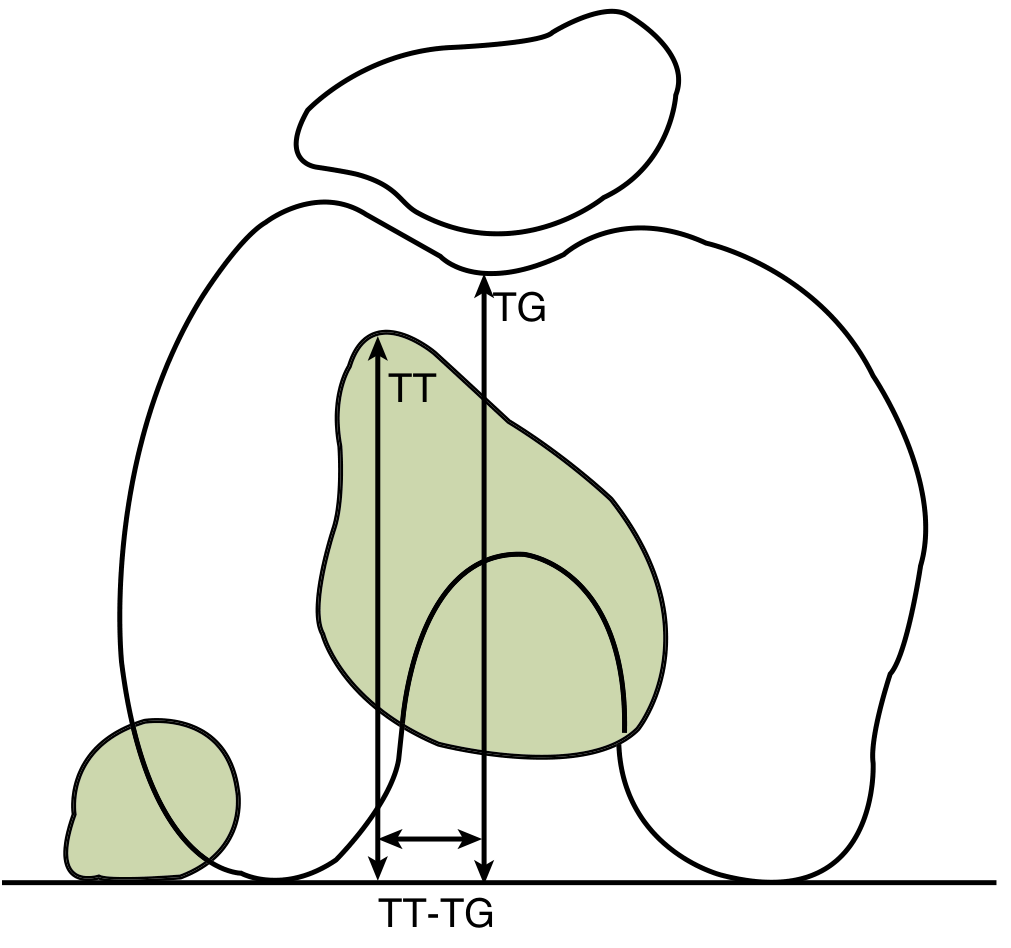
| TT-TG distance | 9-13 mm | Lateral tubercle displacement increases lateral pull; >20 mm = high instability risk |
| Insall-Salvati ratio | 0.8-1.2 | >1.2 = patella alta; reduces trochlear engagement |
| Caton-Deschamps index | 0.6-1.2 | >1.2 = patella alta |
| Trochlear sulcus angle | <140° (axial view) | >145-150° = trochlear dysplasia |
SECTION 2 — CLASSIFICATION OF PATELLAR INSTABILITY
A. By Functional Pattern (Lyon/Dejour Classification)
Three major clinical groups, introduced by H. Dejour:
| Group | Definition |
|---|
| Objective Patellar Instability (OPI) | At least one documented dislocation + identifiable anatomical risk factor. Lateral dislocation during knee extension (non-contact) is the most common presentation. Within OPI: acute (first-time), recurrent (>3 events), habitual (occurs at a consistent knee flexion angle every time), permanent (patella stays dislocated throughout full ROM) |
| Potential Patellar Instability (PPI) | Anatomical risk factors present + knee discomfort, but no documented complete dislocation - only subluxation or apprehension |
| Painful Patellar Syndrome (PPS) | Anterior knee pain without risk factors or dislocation - often misdiagnosed as instability |
B. By Direction of Dislocation
| Type | Description | Mechanism | Frequency |
|---|
| Lateral dislocation | Patella displaced laterally - the patella completely exits the trochlea laterally | Knee flexion + valgus stress + external tibial rotation on planted foot; or direct medial blow | ~95% - by far the most common |
| Medial dislocation | Patella displaced medially | Almost exclusively iatrogenic (over-aggressive lateral release surgery or over-correction of realignment); traumatic medial dislocation is exceedingly rare | Rare |
| Superior dislocation | High-riding patella locked on the anterior femoral condyle in extension | Hyperextension (often in osteoarthritic knees with large osteophytes that trap the patella) | Very rare (<50 cases reported) |
| Intra-articular / horizontal dislocation | Patella rotates 90° inside the joint | High-energy direct trauma | Extremely rare |
| Habitual dislocation | Predictable dislocation occurring at a specific flexion angle during normal gait | Congenital/developmental; tight lateral structures or abnormal muscle insertions | Uncommon |
| Permanent / obligate dislocation | Patella remains permanently displaced, irreducible throughout entire ROM | Severe congenital dysplasia; neuromuscular conditions | Rare |
C. Dejour Classification of Trochlear Dysplasia
Trochlear dysplasia is the single strongest predictor of patellar instability. It is classified based on lateral radiograph signs and axial cross-sectional morphology:
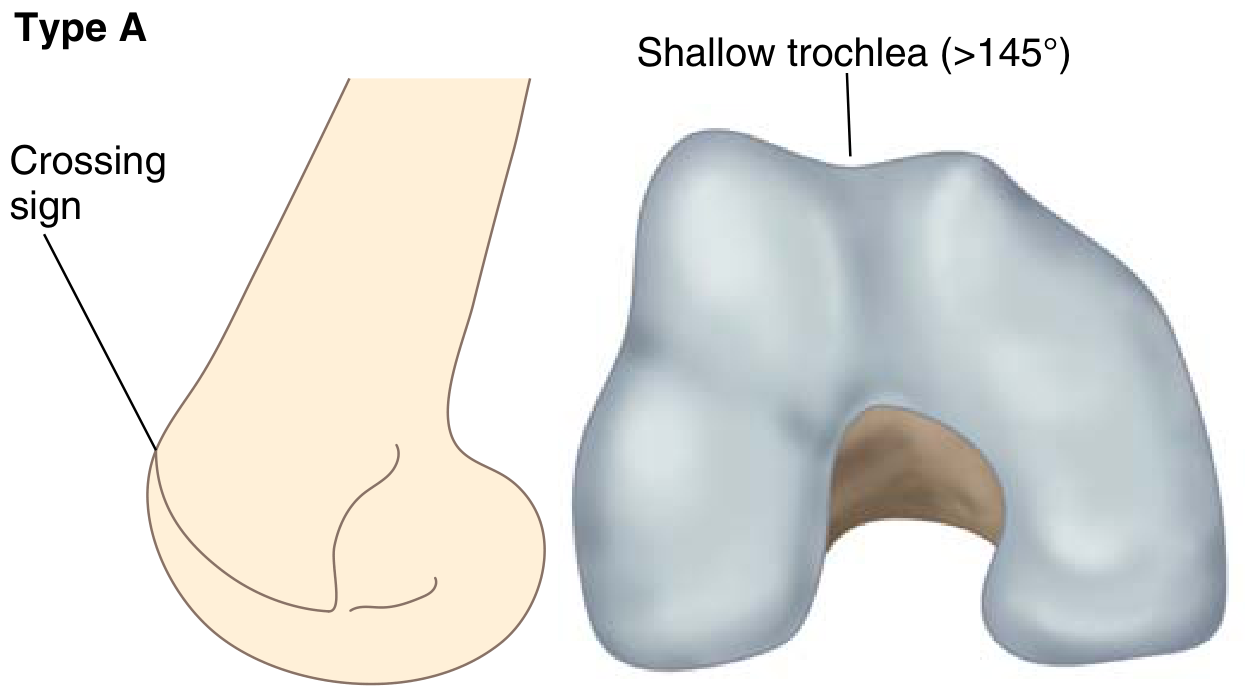
Dejour Type A - Shallow Trochlea
Type A: The trochlear groove line crosses the anterior femoral condyle outline (crossing sign) on the lateral view. Axially the trochlea is shallower than normal but still concave. Sulcus angle >145°.
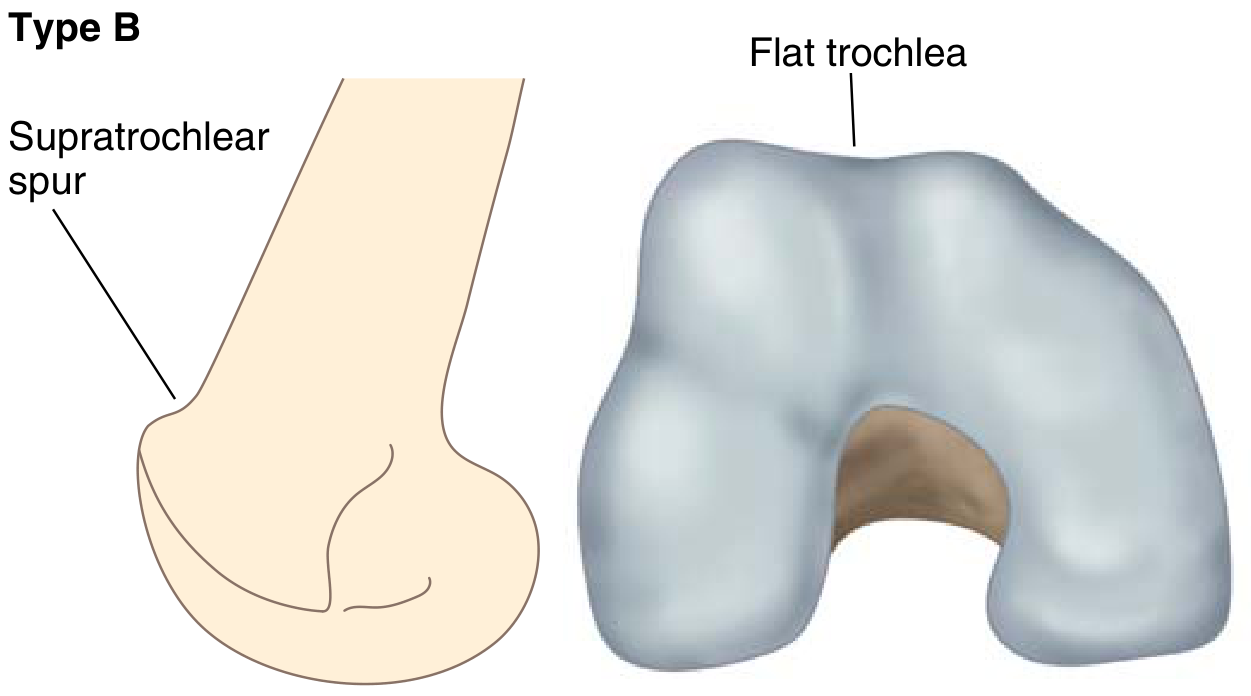
Dejour Type B - Flat Trochlea with Supratrochlear Spur
Type B: Crossing sign PLUS a supratrochlear spur (bony bump protruding proximally). Axially the trochlea is flat or frankly convex - no groove to contain the patella.
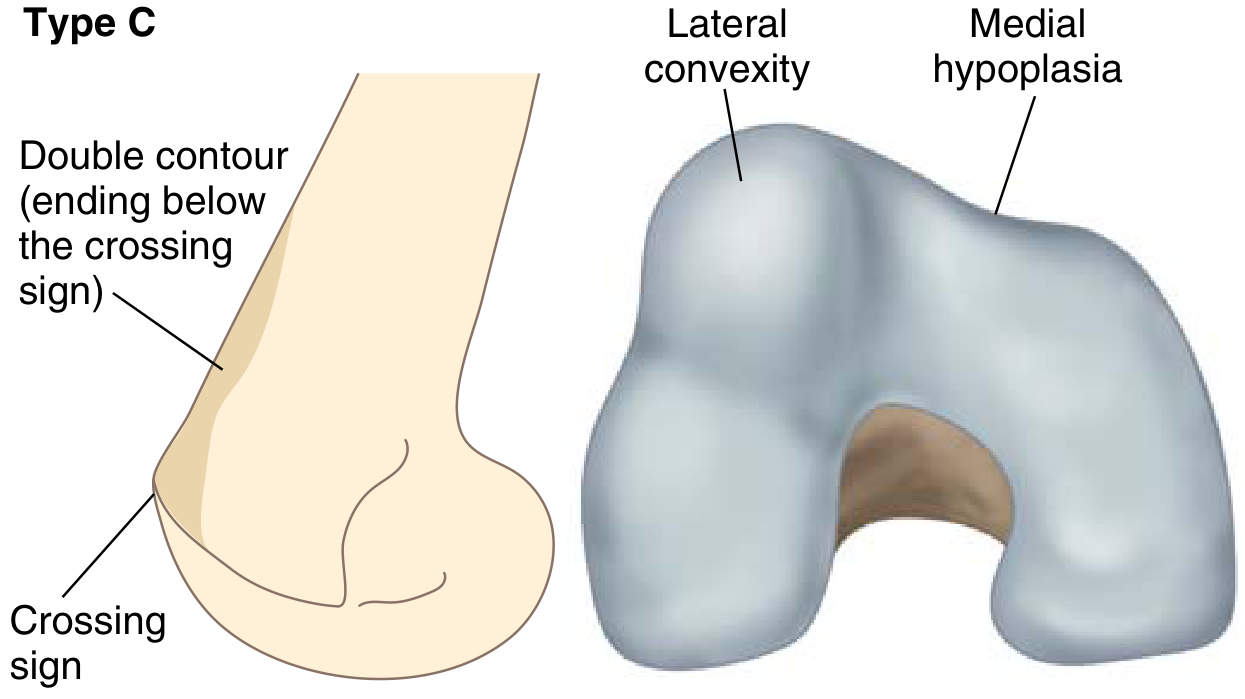
Dejour Type C - Lateral Convexity with Medial Hypoplasia
Type C: Crossing sign PLUS double contour (a second line below the crossing sign representing the hypoplastic medial condyle). Axially: lateral facet is convex while medial facet is hypoplastic.
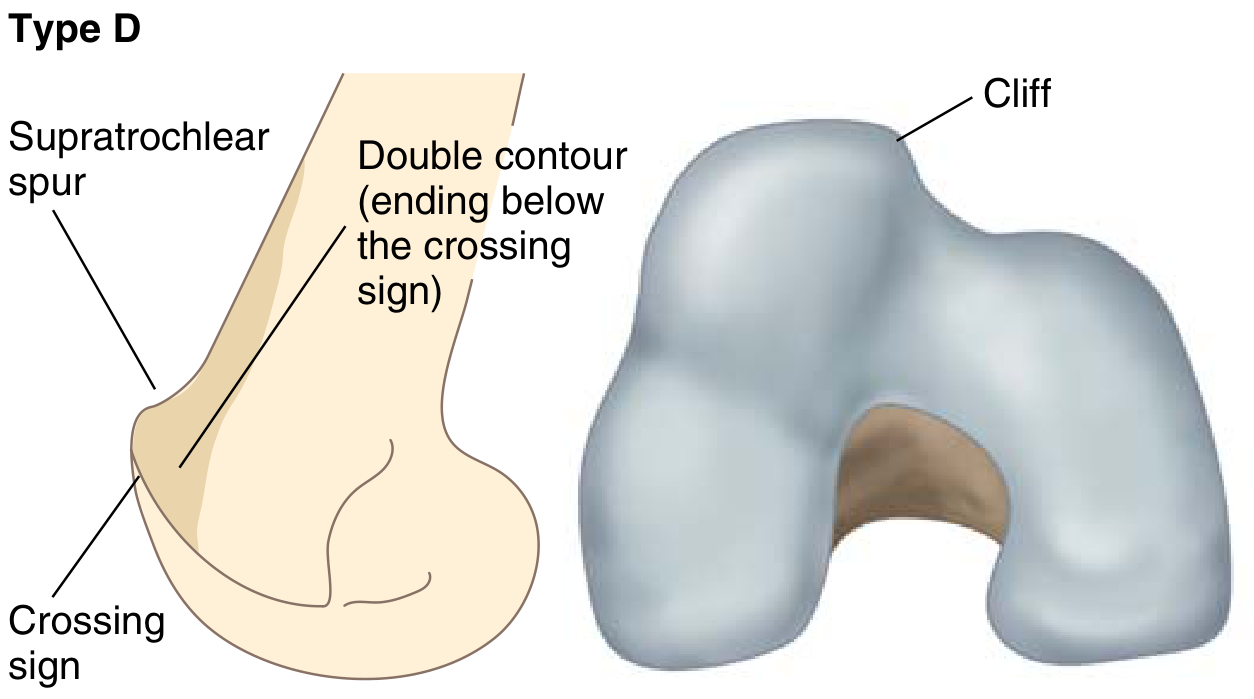
Dejour Type D - Most Severe "Cliff Pattern"
Type D: All three lateral signs present (crossing sign + supratrochlear spur + double contour). Axially there is an abrupt asymmetry ("cliff") between the two facets - the most unstable bony morphology. Type D requires trochleoplasty.
| Dejour Type | Lateral X-ray Signs | Axial Morphology | Surgical Implication |
|---|
| A | Crossing sign only | Shallow trochlea | MPFL recon ± TTO |
| B | Crossing sign + spur | Flat/convex trochlea | MPFL recon + trochleoplasty |
| C | Crossing sign + double contour | Convex lateral + medial hypoplasia | MPFL recon ± TTO |
| D | Crossing sign + spur + double contour | Cliff/asymmetric | MPFL recon + trochleoplasty + TTO |
Updated Dejour V3.0 (2024 - quantitative MRI-based):
- Type 0 (no dysplasia): Sulcus angle <157°; LTI >14°
- Type 1 (low-grade): Sulcus angle >157°; LTI <14°; central bump <5 mm
- Type 2 (moderate): Sulcus angle/LTI unmeasurable; central bump <5 mm
- Type 3 (high-grade): Bump >5 mm; most severe - requires trochleoplasty
SECTION 3 — RISK FACTORS AND PREDISPOSING ANATOMY
| Risk Factor | Detail |
|---|
| Trochlear dysplasia | Most powerful single risk factor; eliminates bony containment |
| Patella alta | Delayed engagement into the trochlea; the patella is "free" for longer during flexion |
| Increased TT-TG distance | Lateral pull vector; >20 mm is strongly associated with instability |
| MPFL deficiency | Traumatic rupture or congenital laxity; >90% ruptured in acute dislocation |
| VMO weakness / hypoplasia | Loss of dynamic medial stabilization |
| Ligamentous laxity | Hypermobility syndromes (Ehlers-Danlos, Down syndrome, Marfan's) |
| Female sex | Higher physiological laxity; broader pelvis increases Q angle |
| Age 10-17 years | Peak incidence 29/100,000 in this age group |
| Femoral anteversion | Increases effective valgus; rotates the trochlea into a less favorable orientation |
| Genu valgum | Increases Q angle and lateral pull |
| Positive family history | Genetic predisposition to dysplasia and laxity |
| "Miserable malalignment syndrome" | Femoral anteversion + genu valgum + pronated feet - compounds instability, especially in adolescents |
- Campbell's Operative Orthopaedics 15th Ed, p. 1861
- Miller's Review of Orthopaedics 9th Ed, p. 365
SECTION 4 — SIGNS AND SYMPTOMS
History
- Mechanism: Pivoting/twisting on a planted foot (most common - non-contact); external tibial rotation with knee flexed; or direct blow to the medial patella
- Age 9-14: A pop + swelling after twisting is more likely patellar instability than ACL tear
- Prior episodes: Recurrence rate is 15-75% after first dislocation
- Spontaneous reduction: Patella often self-reduces as the knee extends; patient describes seeing or feeling the kneecap "pop out and back in"
Symptoms
| Symptom | Description |
|---|
| Acute, severe anterior knee pain | Immediate, localised to the patella |
| Swelling / effusion | Develops within hours post-injury; hemarthrosis common especially with osteochondral fracture |
| Inability to weight bear | Difficulty walking and bending the knee |
| Giving way | Episodic buckling - hallmark of recurrent instability |
| Catching / locking | Suggests loose osteochondral bodies |
| Pop or crack | Heard/felt at time of dislocation; should not be confused with ACL rupture |
| Visible deformity | Patella displaced laterally if not yet spontaneously reduced |
| Stiffness | Post-injury; worse in the morning |
| Subluxation sensation | Patella "threatening to shift" without complete dislocation (in chronic instability) |
| Numbness / paraesthesia | Occasional; from pressure on saphenous nerve or peroneal nerve with significant displacement |
Physical Examination
Inspection:
- Knee held in partial flexion (guarding)
- Visible lateral displacement if still dislocated
- Diffuse swelling and ecchymosis (especially medially - from medial retinaculum/MPFL tear)
- Quadriceps wasting in chronic cases
Palpation:
- Medial retinacular tenderness - the cardinal sign; along medial patellar border and at MPFL attachment on medial femoral condyle
- Hemarthrosis / joint effusion - ballottement, fluctuance
- Palpable defect in the medial retinaculum (acute)
- Diffuse patellar tenderness
Special Clinical Tests:
| Test | Technique | Positive Finding | Significance |
|---|
| Patellar apprehension test (Fairbank's sign) | Patient supine, knee at 20-30°; examiner pushes patella laterally | Fear, quadriceps contraction, patient grabs examiner's hand | Most specific test for lateral instability; sensitivity ~39%, specificity ~92% |
| Patellar glide test | Divide patella into 4 quadrants mediolaterally; assess excursion | >3 quadrants lateral = hypermobility; <1 quadrant medial = lateral retinacular tightness | Quantifies passive restraints |
| J-sign | Observe patella tracking during active extension from 90° to 0° | Patella jumps laterally ("J" shape) as it exits the trochlea near full extension | Suggests patella alta or trochlear dysplasia |
| Patellar tilt test | Examiner lifts lateral patellar edge with knee extended | <0° tilt (lateral edge cannot be elevated to neutral) = lateral retinacular tightness | Guides lateral release decision |
| Medial apprehension test | Medially directed pressure on patella | Apprehension = iatrogenic medial instability (post lateral release) | |
| Clarke's test | Compress patella into trochlea, patient contracts quadriceps | Pain under patella | Non-specific; patellofemoral chondromalacia |
| VMO assessment | Palpate VMO during straight leg raise | Atrophy or absent contraction | Chronic instability |
SECTION 5 — INVESTIGATIONS AND EVALUATION
Step-by-Step Investigation Framework
ACUTE PRESENTATION
↓
1. Clinical examination → Confirm dislocation or spontaneous reduction
↓
2. Plain radiographs (AP + lateral ± Merchant/sunrise)
↓
3. Reduce if still dislocated → Post-reduction films
↓
4. Is there hemarthrosis or suspected osteochondral fracture?
YES → MRI
NO → Conservative management
↓
5. Recurrent/chronic instability: CT for TT-TG measurement
↓
6. Risk stratification → Guide surgical planning
Radiography (First-Line in All Cases)
Views Required:
| View | What It Shows |
|---|
| AP (weight-bearing) | Overall alignment, fractures, loose bodies, patella position |
| True lateral (30° flexion) | Patella alta/baja; trochlear morphology (crossing sign, supratrochlear spur, double contour); Blumensaat line |
| Axial/Merchant (30-45°) | Patellar tilt and subluxation; sulcus angle; congruence angle; typically hard to obtain pre-reduction |
| Sunrise view (post-reduction) | Confirms patella centred in groove; detects residual subluxation; osteochondral fragments |
Radiographic findings in acute dislocation:
- Empty or shallow trochlear groove (AP/axial)
- Laterally displaced patella
- Soft tissue swelling/effusion
- Osteochondral fracture fragment at medial inferior patellar margin (pathognomonic avulsion) or lateral femoral condyle
- Lipohemarthrosis on horizontal-beam lateral = intra-articular fracture
Trochlear dysplasia signs on lateral X-ray:
- Crossing sign: Floor of trochlear groove crosses the anterior femoral condyle line = dysplasia present
- Supratrochlear spur: Bony prominence proximal to trochlea = Type B/D
- Double contour: Hypoplastic medial condyle line below crossing sign = Type C/D
MRI (Recommended for All Acute Dislocations with Effusion)
The International Patellofemoral Study Group recommends MRI for patients with large hemarthrosis to detect osteochondral fractures. (Rockwood and Green's, p. 3020)
| MRI Finding | Significance |
|---|
| "Kissing contusions" - lateral femoral condyle + medial patellar bone bruise | Pathognomonic of lateral patellar dislocation mechanism |
| MPFL disruption | Present in >90% of first-time dislocations; most commonly at patellar insertion |
| Osteochondral fracture | Articular cartilage injury in up to 95% of first-time dislocators; patellar side (26.5%) > femoral side (15%) |
| Loose bodies | Free chondral/osteochondral fragments requiring arthroscopic removal |
| VMO injury | Tear or haematoma in medial soft tissues |
| Cartilage mapping | Grading of chondral damage on patellar and femoral surfaces |
| TT-TG measurement | Possible on MRI but underestimates vs CT; CT preferred for this measurement |
CT Scan (For Surgical Planning - TT-TG Measurement)
TT-TG distance: measured on superimposed axial CT slices comparing the tibial tubercle (TT) centre to the deepest point of the trochlear groove (TG). This quantifies the lateral displacement of the tibial tubercle relative to the trochlear groove.
| TT-TG Value | Interpretation |
|---|
| 9-13 mm | Normal |
| 15-20 mm | Borderline; consider clinical context |
| >20 mm | Significantly abnormal; indication for tibial tubercle osteotomy |
Other CT uses:
- Precise trochlear depth and sulcus angle measurement
- Torsional profile (femoral anteversion, tibial torsion)
- Detect osseous loose bodies
- Dynamic CT to assess patellar tracking during flexion
Arthroscopy (Selective)
Reserved for:
- Large hemarthrosis with suspected loose osteochondral fragments
- Concurrent intra-articular pathology
- Pre-surgical assessment of cartilage
- Removal of free fragments
Patient-Reported Outcomes
- Kujala score (AKPS) - gold standard patellofemoral outcome tool
- IKDC - International Knee Documentation Committee
- KOOS - Knee Injury and Osteoarthritis Outcome Score
- Lysholm score
SECTION 6 — TREATMENT
A. Emergency Management: Closed Reduction
Indications: Patella still dislocated on presentation.
Technique:
- Analgesia (oral/IV; conscious sedation usually not needed)
- Patient supine, hip flexed to relax hamstrings
- Gently and slowly extend the knee while simultaneously applying inferomedially-directed pressure to the patella
- If difficult: gentle downward pressure on the lateral patellar border to "open" the medial facet
- A "click" is felt/heard as the patella seats into the trochlea
- Neurovascular check immediately after reduction
- Post-reduction radiographs (AP + lateral + sunrise) to confirm centring and exclude osteochondral fracture
Post-reduction care:
- Knee immobilizer in full extension
- Weight bear as tolerated with crutches
- Orthopedic follow-up within 1-2 weeks
- Ice + elevation + NSAIDs for pain/swelling
B. Conservative (Non-Operative) Management
Indicated for: First-time dislocation without osteochondral fracture. (Campbell's, p. 1861; Rockwood and Green's, p. 3020)
| Phase | Timeline | Treatment |
|---|
| Phase 1 - Acute protection | 0-2 weeks | Knee immobilizer in extension; partial weight-bearing; cryotherapy; NSAIDs; isometric quad sets |
| Phase 2 - Rehabilitation | 2-6 weeks | Transition to patellar-stabilizing brace; progressive ROM; closed-chain quadriceps exercises with VMO emphasis; hip abductor/ER strengthening; patellar taping; proprioception training |
| Phase 3 - Return to sport | 6-12 weeks | Full ROM, no effusion, quad strength ≥80% of contralateral side; sport-specific training |
Outcomes of conservative treatment:
- Recurrence rate: 15-44% (Rockwood & Green) to 15-75% (Campbell's)
- No long-term functional difference vs surgery in first-time dislocators without osteochondral injury
C. Surgical Treatment
Indications for surgery:
| Indication | Evidence Level |
|---|
| Displaced osteochondral fracture / free loose body | Strong - most authors agree |
| Recurrent instability (≥2 dislocations) | Strong |
| Large complete MPFL avulsion on MRI | Relative indication |
| Patellar subluxation on Merchant view post-reduction | Relative |
| First-time dislocation in high-risk anatomy (Dejour B/D, TT-TG >20 mm) | Relative - growing consensus |
| High-level athletes with predisposing anatomy | Relative |
| Persistent pain/laxity after failed conservative management | Strong |
Surgical Procedure 1: MPFL Reconstruction (Proximal Realignment)
The current gold standard for recurrent lateral patellar instability.
Principle: Restore the medial soft tissue restraint by reconstructing the MPFL with a tendon graft.
Technique:
- Graft: gracilis or semitendinosus tendon (autograft or allograft)
- Patellar attachment: suture anchors or bone tunnels at superomedial patellar border
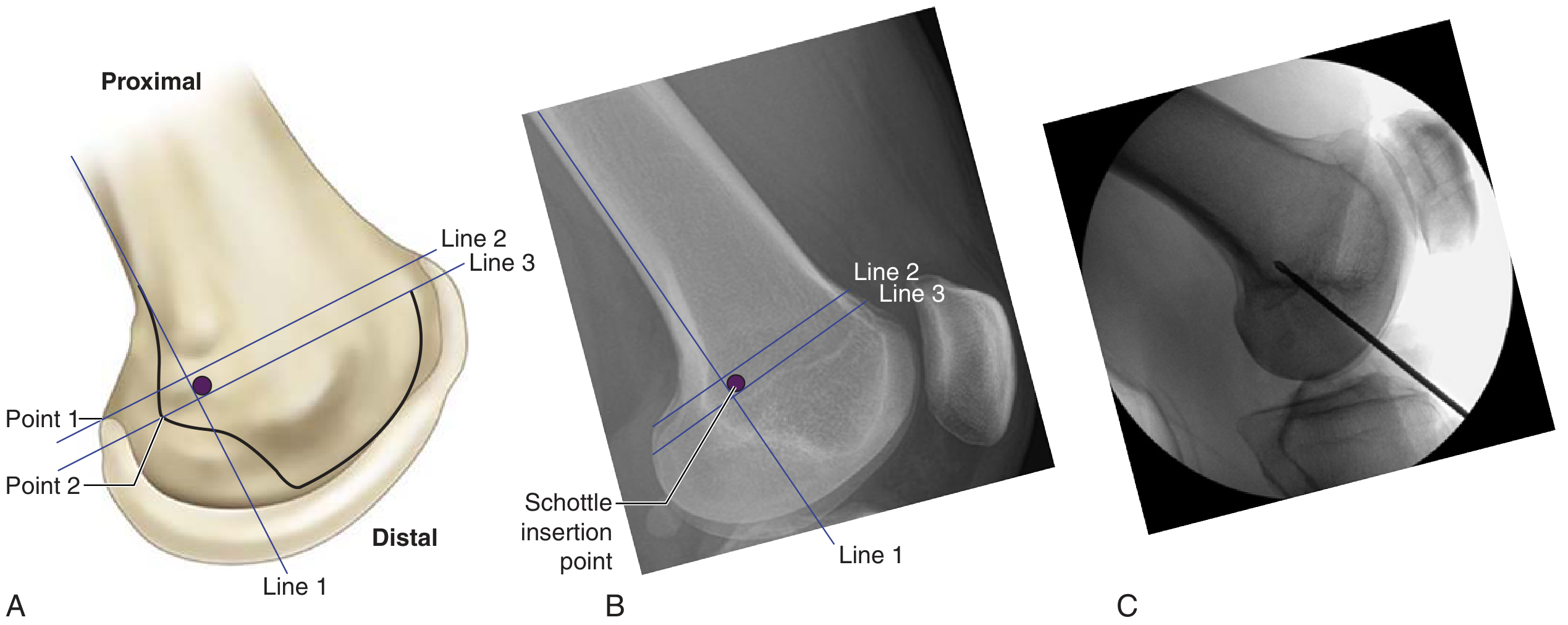
- Femoral attachment: Schottle's point (anatomically critical)
Schottle's point - the anatomic origin of the MPFL on the medial femoral condyle. (A) Anatomical diagram: 1 mm anterior to the posterior cortex line, 2.5 mm distal to the posterior medial femoral condyle, proximal to Blumensaat line. (B) Lateral radiograph landmarks. (C) Intraoperative fluoroscopy for tunnel confirmation. Incorrect placement causes isometry failure: too proximal = graft tight in flexion; too distal = graft loose in flexion.
- Miller's Review of Orthopaedics 9th Ed, p. 366
Procedures that have fallen out of favour:
- Isolated lateral release (contraindicated for instability - causes medial iatrogenic dislocation)
- VMO advancement (Green procedure)
- Medial retinacular plication alone
Surgical Procedure 2: Tibial Tubercle Osteotomy (Distal Realignment)
Indicated when: TT-TG >20 mm, or symptomatic distal patellar chondromalacia (anteriorization component offloads the distal pole).
Main techniques:
| Procedure | Components | Primary Indication |
|---|
| Fulkerson osteotomy (anteromedialization - AMZ) | Osteotomy moves TT anteriorly + medially | TT-TG >20 mm + distal patellar chondromalacia |
| Elmslie-Trillat | Purely medial transfer of TT | Isolated TT-TG elevation without chondral disease |
| Maquet | Anterior transfer only (rarely used now) | Isolated patellar chondromalacia |
Contraindication to medialization: Proximal patellar arthrosis of the medial facet (would impinge the medially transferred patella against medial osteophytes).
Surgical Procedure 3: Trochleoplasty
- Indicated for: High-grade trochlear dysplasia with supratrochlear bump (Dejour Type B, D, and V3.0 Type 3) where the bony deformity is too severe for soft tissue procedures alone
- Technique: Bereiter sulcus-deepening trochleoplasty - the supratrochlear bump is resected/levelled by elevating a thin osteochondral flap, deepening the underlying groove, then reseating the cartilage flap
- Usually combined with MPFL reconstruction
- Technically demanding; requires significant surgical expertise
- Indicated when: central bump >5 mm on MRI (V3.0 Type 3)
Current Treatment Algorithm (2024-2026)
ACUTE FIRST-TIME DISLOCATION
↓
Osteochondral fracture present?
YES → Surgery (fix or remove fragment)
NO → Conservative management
↓
RECURRENT INSTABILITY / SURGICAL CANDIDATE
↓
Step 1: ALWAYS include MPFL reconstruction (ruptured >90% of cases)
↓
Step 2: Evaluate TT-TG distance (CT)
↓
TT-TG <20 mm TT-TG >20 mm
MPFL alone MPFL + tibial tubercle
osteotomy (medialization)
↓
Step 3: Evaluate trochlear dysplasia (Dejour)
↓
Type A/C (no bump) Type B/D or V3.0 Type 3 (bump)
No trochleoplasty Add trochleoplasty
↓
Step 4: Evaluate patella height
↓
Patella alta (CDI >1.2) Target: PHI <1.16 post-op
Consider tubercle SPE >38%, TT-TG 8-14 mm post-op
distalization
D. Specific Management of Rare Dislocation Types
| Type | Specific Management |
|---|
| Medial dislocation (iatrogenic) | Medial retinacular release + lateral retinacular reconstruction; address over-corrected anatomy |
| Superior dislocation | Manual closed reduction (flex the knee while applying inferior pressure); surgical osteophyte removal if recurs; common in osteoarthritic knees |
| Habitual dislocation | Typically requires surgery: MPFL reconstruction + trochleoplasty; lateral retinacular lengthening if the distal ITB/VL is too tight |
| Permanent dislocation | Surgical: requires complete lateral soft tissue release + reconstruction; high complexity |
| Congenital dislocation | Often associated with syndromes (Down, Larsen, nail-patella syndrome); early surgical correction before gait patterns are established |
| Intra-articular dislocation | May require surgical reduction + fixation/removal of osteochondral fragment |
SECTION 7 — COMPLICATIONS
| Complication | Detail |
|---|
| Osteochondral fracture | Up to 95% articular cartilage injury in first-time dislocators |
| Recurrent instability | 15-75% after conservative management; highest in young patients with dysplasia |
| Post-traumatic patellofemoral osteoarthritis | Long-term consequence of cartilage damage |
| Iatrogenic medial instability | After over-aggressive lateral release; disabling |
| MPFL graft failure | Incorrect tunnel position (non-isometric placement); over-tensioning |
| Stiffness/loss of flexion | Especially after tibial tubercle osteotomy or prolonged immobilization |
| Osteotomy non-union / hardware issues | After tibial tubercle osteotomy |
| Saphenous nerve injury | At risk in medial surgical approaches |
| Patellar fracture | Complication of patellar tunnel MPFL technique |
SECTION 8 — SUMMARY TABLE
| Parameter | Key Points |
|---|
| Most common type | Lateral dislocation (~95%) |
| Peak incidence | Age 10-17 years; 29/100,000/year |
| Most important risk factor | Trochlear dysplasia |
| Strongest instability predictor | TT-TG >20 mm |
| MPFL rupture rate in acute dislocation | >90% |
| First-line imaging | AP + lateral + post-reduction sunrise X-ray |
| MRI indications | Hemarthrosis, suspected osteochondral fracture, effusion present |
| CT indication | TT-TG measurement for surgical planning |
| First-line treatment | Closed reduction + immobilizer + physiotherapy |
| Surgery - first-time dislocation | Only if osteochondral fracture/loose body, or high-risk anatomy |
| Surgery - recurrent instability | MPFL reconstruction ± TTO ± trochleoplasty |
| TT-TG normal | 9-13 mm |
| Recurrence rate (conservative) | 15-75% |
| Gold standard surgical procedure | MPFL reconstruction at Schottle's point |
Sources cited:
- Campbell's Operative Orthopaedics, 15th Ed 2026, p. 1861 - patellar dislocations, treatment
- Miller's Review of Orthopaedics, 9th Ed, pp. 364-366 - patellar instability, Dejour classification, MPFL, surgical techniques
- Rockwood and Green's Fractures in Adults, 10th Ed 2025, pp. 3019-3021 - acute patellar dislocations, preferred treatment
- Rosen's Emergency Medicine, pp. 720-721 - clinical features, closed reduction technique
- Tintinalli's Emergency Medicine - pediatric patellar dislocations
- Patellar instability: current approach (PMC 2026) - Dejour V3.0 classification, 2024 updated treatment algorithm