Thyroid inhibitors
Reading File
Finding Sources
Finding Sources
Searching PubMed
antithyroid drugs hyperthyroidism
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Here is the full review:
Thyroid Inhibitors
Thyroid inhibitors are compounds that interfere - directly or indirectly - with the synthesis, release, or action of thyroid hormones. They fall into four major groups:
- Antithyroid drugs (thioamides)
- Ionic inhibitors
- High-concentration iodine
- Radioactive iodine
Plus adjuvant agents that target peripheral effects.
1. Antithyroid Drugs (Thioamides / Thioureylenes)
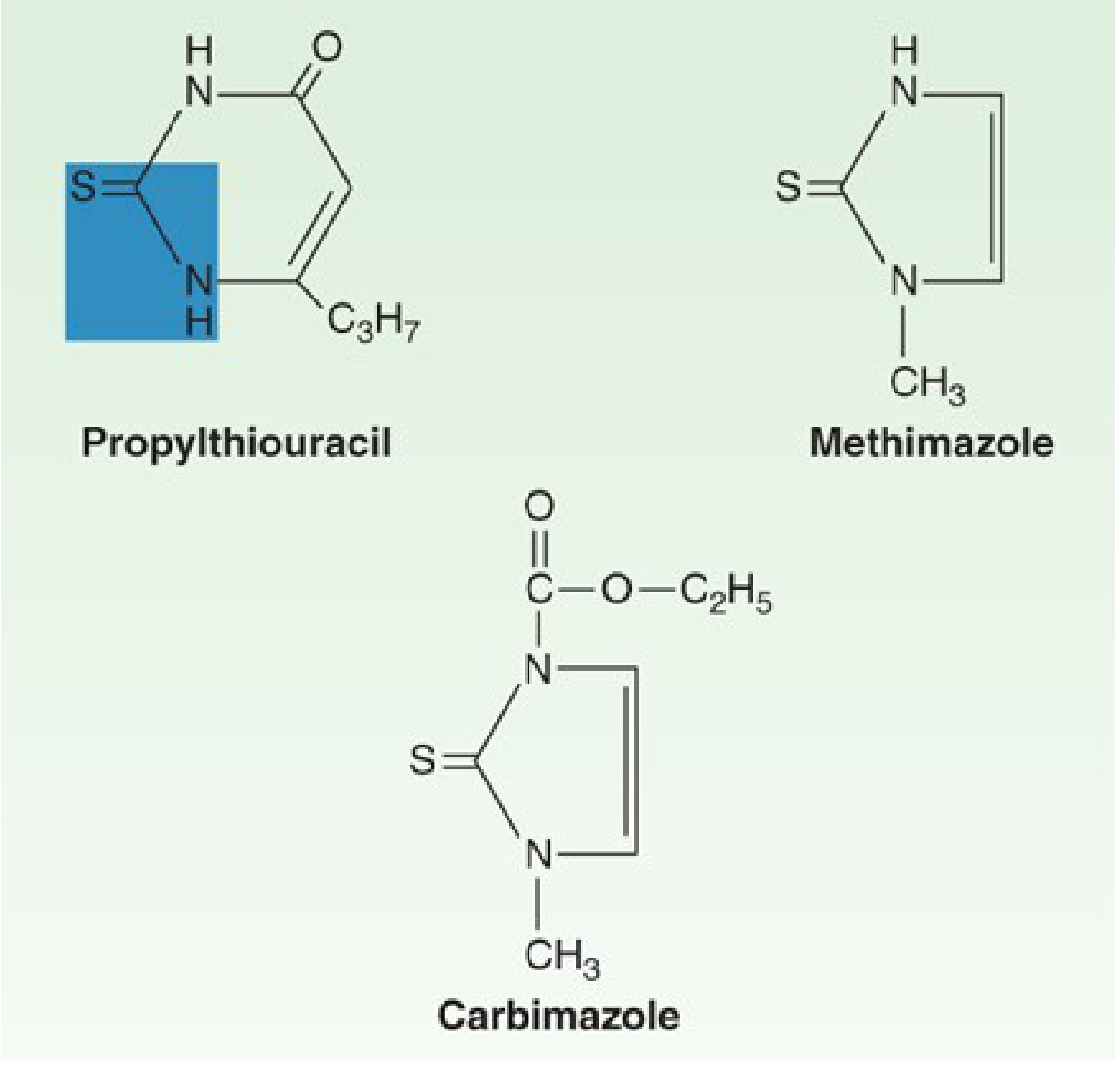
Drugs in This Class
- Propylthiouracil (PTU)
- Methimazole
- Carbimazole (a prodrug of methimazole, widely used in the UK)
The thiocarbamide group (-C=S-NH-) is essential for antithyroid activity in all three.
Mechanism of Action
- Primary action: Inhibit thyroid peroxidase (TPO)-catalyzed reactions, blocking the organification of iodine (oxidation of iodide to iodine and its incorporation into tyrosine residues on thyroglobulin).
- Secondary action: Block coupling of iodotyrosines (MIT + DIT) to form T3 and T4.
- PTU only: Also inhibits the peripheral deiodination of T4 to the more active T3 (via inhibition of type 1 deiodinase - Dio1). Methimazole does NOT share this extra action.
- They do not block iodide uptake into the gland.
Potency Comparison
Methimazole is approximately 10 times more potent than PTU on a per-mg basis.
Pharmacokinetics
| Property | PTU | Methimazole |
|---|---|---|
| Absorption | Rapid; peak at 1 h; bioavailability 50-80% | Complete, but variable rate |
| Plasma half-life | ~1.5 hours | ~6 hours |
| Protein binding | Higher (more strongly bound) | Lower |
| Dosing frequency | Every 6-8 hours | Once daily (30 mg suppresses for >24 h) |
| Duration of action | A 100 mg dose inhibits organification by 60% for ~7 h | Single 30 mg dose effective for >24 h |
| Metabolism | Excreted as inactive glucuronide in urine within 24 h | 65-70% of dose excreted in urine within 48 h |
Both drugs are concentrated by the thyroid gland, so their short plasma half-lives do not fully reflect their duration of action.
Use in Pregnancy
- Both cross the placenta into the fetal thyroid (risk of fetal hypothyroidism - FDA Pregnancy Category D).
- PTU is preferred in the first trimester because it is more protein-bound and crosses the placenta less readily. Methimazole has rarely been associated with congenital malformations (aplasia cutis, choanal atresia).
- After the first trimester, methimazole is preferred due to PTU's black-box hepatotoxicity warning.
- Low concentrations of both are found in breast milk but are considered safe for nursing infants.
Special Indications for PTU Over Methimazole
PTU should be reserved for:
- First trimester of pregnancy
- Thyroid storm (both blocks new synthesis AND reduces peripheral T4-to-T3 conversion)
- Patients with adverse reactions to methimazole (excluding agranulocytosis or hepatitis, in which case neither can be used)
Adverse Effects
| Adverse Effect | Notes |
|---|---|
| Agranulocytosis | Most serious; ~0.3-0.6% incidence. Warn patients to report sore throat/fever immediately. Recent meta-analysis (PMID 40745151) examined dose-risk relationship. |
| Hepatotoxicity | PTU carries a black-box warning for severe, potentially fatal hepatitis. Methimazole more commonly causes cholestatic jaundice (milder). |
| Skin rash / urticaria | ~5% incidence; most common minor side effect |
| Arthralgia | Dose-related |
| Hypothyroidism | From over-treatment |
| Lupus-like syndrome | Rare, mainly with PTU |
2. Ionic Inhibitors (Iodide Uptake Inhibitors)
These are anions that compete with iodide for transport by the sodium/iodide symporter (NIS), blocking iodide uptake into the thyroid.
| Agent | Notes |
|---|---|
| Perchlorate (ClO4-) | Most potent; used in iodine-induced hyperthyroidism (e.g., amiodarone). A 2024 systematic review confirmed utility in thyrotoxicosis. |
| Thiocyanate (SCN-) | Found in cabbage and brassica vegetables; historically noted to cause goiter |
| Pertechnetate (TcO4-) | Used diagnostically (Tc-99m scans) |
| Fluoroborate, nitrate | Less clinically relevant |
Thiocyanate also blocks organification at high concentrations (overlaps with thioamide mechanism).
3. High-Concentration Iodine (Iodides)
Paradoxically, at high concentrations, iodide inhibits thyroid function (in contrast to trace iodine which is necessary for hormone synthesis).
Mechanisms
- Wolff-Chaikoff effect: High intrathyroidal iodide concentration acutely and transiently inhibits iodotyrosine and iodothyronine synthesis (organification blockade). Normal thyroid "escapes" from this effect after ~10-15 days by downregulating NIS.
- Inhibition of hormone release: The most clinically important acute effect - rapid, efficacious in severe thyrotoxicosis.
- Reduces gland vascularity, causes follicular cells to shrink, and allows colloid reaccumulation.
Clinical Uses
- Preoperative preparation for thyroidectomy (firms the gland, reduces vascularity)
- Thyrotoxic crisis (thyroid storm) - combined with thioamides and propranolol
- Radiation emergency - 130 mg KI blocks thyroidal uptake of radioactive iodine fallout
Preparations & Doses
- Lugol's solution (5% iodine + 10% KI): ~8 mg iodine/drop; dose 2-6 drops three times daily
- KISS (Potassium iodide saturated solution): 50 mg/drop; dose 1-2 drops three times daily
- Thyroshield (OTC): 130 mg/2 mL for radiation emergencies
Limitations
- Beneficial effect disappears after ~10-15 days (escape phenomenon)
- Does not completely control hyperthyroidism on its own
- Susceptible patients (pre-existing thyroid disorders) may develop iodine-induced hypothyroidism (failure to escape Wolff-Chaikoff)
Adverse Effects (Iodism)
- Brassy/metallic taste, hypersalivation, burning in mouth/throat
- Angioedema, laryngeal edema (life-threatening)
- Serum sickness-type reactions: fever, arthralgia, lymphadenopathy, eosinophilia
- Thrombotic thrombocytopenic purpura (rare)
4. Radioactive Iodine (131I)
- Taken up by thyroid via NIS (same as stable iodine)
- Emits beta radiation (primarily responsible for thyroid tissue destruction) and gamma radiation
- Causes progressive, permanent destruction of thyroid follicular cells
- Used for definitive treatment of Graves' disease and toxic nodular goiter
- Contraindicated in pregnancy and breastfeeding
- A 2025 network meta-analysis (PMID 40891035) compared mortality risks among RAI, antithyroid drugs, and surgery for hyperthyroidism.
5. Adjuvant Agents (No Direct Thyroid Effect)
These drugs do not block thyroid hormone synthesis but control the peripheral manifestations of thyrotoxicosis:
| Drug | Mechanism | Use |
|---|---|---|
| Propranolol (beta-blocker) | Blocks sympathetic overactivation; also inhibits peripheral T4-to-T3 conversion at high doses | Symptom control (tachycardia, tremor, anxiety) in thyroid storm and pre-op prep |
| Ca2+ channel blockers | Control heart rate | For beta-blocker intolerance |
| Amiodarone | Inhibits peripheral deiodination (T4->T3); contains 37% iodine by weight | Also causes iodine-induced thyroid dysfunction (both hypo- and hyperthyroidism) |
| Lithium | Inhibits hormone release from the gland | Second-line in thyrotoxicosis; narrow therapeutic window |
| Oral cholecystographic agents | Inhibit peripheral deiodination | Historical use in thyroid storm |
| Glucocorticoids | Inhibit peripheral deiodination; suppress TSH | Adjunct in thyroid storm |
Summary Table: Agents That Disrupt Thyroid Hormone Pathways
| Mechanism | Agents |
|---|---|
| Block iodide uptake (NIS) | Perchlorate, fluoroborate, thiocyanate, nitrate |
| Block organification | Thioamides (PTU, methimazole, carbimazole), thiocyanate, sulfonamides |
| Block coupling reaction | Sulfonamides, thioamides |
| Inhibit hormone release | Lithium salts, high-dose iodide |
| Inhibit peripheral T4-to-T3 deiodination | PTU, amiodarone, oral cholecystographic agents |
| Accelerate hepatic metabolism of T4/T3 | Phenobarbital, rifampin, carbamazepine, phenytoin, sertraline, bexarotene |
| Destroy thyroid tissue | Radioactive iodine (131I) |
Sources:
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed. - Ch. 47 (Thyroid and Antithyroid Drugs), pp. 970-975
- Katzung's Basic and Clinical Pharmacology, 16th ed. - Ch. 38 (Thyroid and Antithyroid Drugs), pp. 1079-1090
- Recent evidence: Agranulocytosis dose-risk [PMID 40745151], Perchlorate review [PMID 38195966], Mortality comparison RAI/ATD/surgery [PMID 40891035]
This is a shared conversation. Sign in to Orris to start your own chat.