give me extransic & INTRINSIC PATHWAY OF Clothing factore with deatail and iamge
Reading File
Finding Sources
Finding Sources
Searching Images
coagulation cascade extrinsic intrinsic pathway clotting factors diagram
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks and excellent diagrams. Let me compile the full, detailed answer.
Coagulation (Clotting) Pathways: Extrinsic & Intrinsic
Blood coagulation proceeds through a cascade of sequential zymogen activations — each activated factor (serine protease) catalyzes the next — culminating in a stable fibrin clot. There are two initiating arms (extrinsic and intrinsic) that converge on a shared common pathway.
Overview Diagram
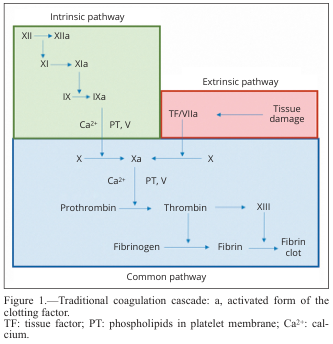
Traditional coagulation cascade. TF = tissue factor; PT = phospholipids; Ca²⁺ = calcium ions; "a" suffix = activated form.
Clotting Factors Summary Table
| Factor | Name | Type | Pathway |
|---|---|---|---|
| I | Fibrinogen | Substrate → Fibrin | Common |
| II | Prothrombin | Zymogen → Thrombin (serine protease) | Common |
| III | Tissue Factor (Thromboplastin) | Cofactor (membrane glycoprotein) | Extrinsic |
| IV | Calcium (Ca²⁺) | Cofactor | All |
| V | Labile factor / Proaccelerin | Cofactor | Common |
| VII | Proconvertin | Zymogen (Vit K-dependent) | Extrinsic |
| VIII | Antihemophilic factor A | Cofactor | Intrinsic |
| IX | Christmas factor | Zymogen (Vit K-dependent) | Intrinsic |
| X | Stuart-Prower factor | Zymogen (Vit K-dependent) | Common |
| XI | Plasma thromboplastin antecedent | Zymogen | Intrinsic |
| XII | Hageman factor | Zymogen | Intrinsic (contact) |
| XIII | Fibrin-stabilizing factor | Zymogen (transglutaminase) | Common |
| — | Prekallikrein (PK) | Contact factor | Intrinsic (contact) |
| — | HMWK (High-MW Kininogen) | Cofactor | Intrinsic (contact) |
| — | von Willebrand Factor (vWF) | Carrier/platelet adhesion | Supports intrinsic |
Vitamin K-dependent factors (synthesized in the liver, require γ-carboxylation of Glu residues): II, VII, IX, X (and proteins C, S, Z). Warfarin blocks their synthesis.
🔴 Extrinsic Pathway ("Tissue Factor Pathway")
Trigger: Vascular injury → exposure of Tissue Factor (TF / Factor III), a subendothelial transmembrane glycoprotein abundantly expressed on fibroblasts and vascular smooth muscle cells.
Step-by-Step:
Tissue injury
↓
Tissue Factor (TF) exposed on subendothelium
↓
TF + Factor VII (circulating zymogen, Vit K-dependent)
↓ [Ca²⁺ required]
TF:VIIa complex (Extrinsic Tenase complex)
↓
Activates Factor X → Factor Xa ← Enters Common Pathway
↓
(Also activates Factor IX → Factor IXa) ← Crossover to Intrinsic
Key points:
- TF acts as a cofactor for Factor VIIa, dramatically amplifying its enzymatic activity
- TF:VIIa complex activates both Factor X and Factor IX — this crossover links extrinsic and intrinsic pathways
- The reaction requires assembly on a phospholipid membrane surface in the presence of Ca²⁺
- Factor VII's Gla residues (γ-carboxyglutamate) bind Ca²⁺ and anchor it to membrane surfaces
- Assessed in the lab by Prothrombin Time (PT / INR)
🔵 Intrinsic Pathway ("Contact Activation Pathway")
Trigger: Contact of blood/plasma with a negatively charged surface (in vivo: damaged vessel collagen, platelet phospholipids; in vitro: glass).
Step-by-Step:
Contact with negatively charged surface
↓
Factor XII (Hageman factor) → Factor XIIa
(assisted by Prekallikrein + HMWK)
↓
Factor XI → Factor XIa [Ca²⁺]
↓
Factor IX → Factor IXa [Ca²⁺]
↓
Factor IXa + Factor VIIIa + Ca²⁺ + Phospholipids
= "Intrinsic Tenase Complex" (on platelet surface)
↓
Factor X → Factor Xa ← Enters Common Pathway
Key points:
- FXII, PK, HMWK form the contact activation complex — but FXII deficiency does NOT cause clinical bleeding (it is not physiologically essential in vivo)
- Factor VIII is the cofactor that, when activated to VIIIa by thrombin (feedback), dramatically accelerates IXa activity (~200,000×)
- Hemophilia A = Factor VIII deficiency; Hemophilia B = Factor IX deficiency — both cause severe bleeding because this pathway is critical for amplification in vivo
- Assessed in the lab by aPTT (activated Partial Thromboplastin Time)
🟣 Common Pathway
Both pathways converge here at Factor X activation.
Factor Xa + Factor Va + Ca²⁺ + Phospholipids
= Prothrombinase Complex (on platelet/cell membrane)
↓
Prothrombin (II) → Thrombin (IIa)
↓
Thrombin cleaves Fibrinogen (I)
→ releases Fibrinopeptide A (FPA) + Fibrinopeptide B (FPB)
→ Fibrin monomer
↓
Fibrin monomers spontaneously polymerize
↓
Thrombin activates Factor XIII → Factor XIIIa (transglutaminase)
↓
Factor XIIIa cross-links fibrin polymers covalently
↓
✅ STABLE CROSS-LINKED FIBRIN CLOT
Detailed Cascade with Lab Tests
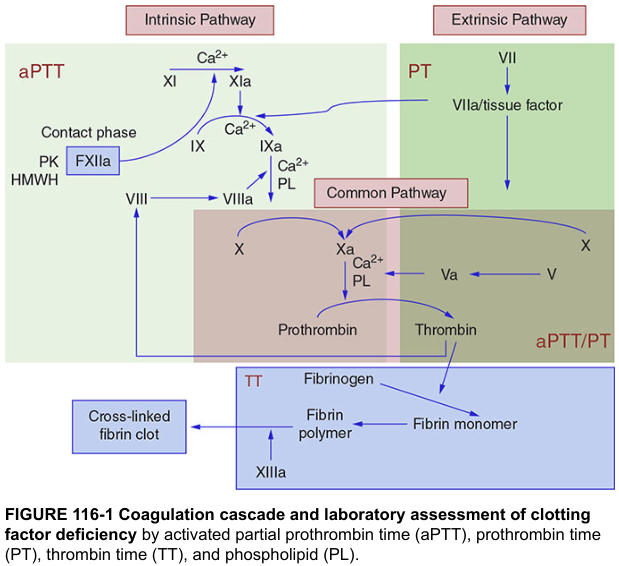
From Harrison's Principles of Internal Medicine 22e — coagulation cascade with aPTT (intrinsic + common) and PT (extrinsic + common) correlation.
Anticoagulant Drug Targets
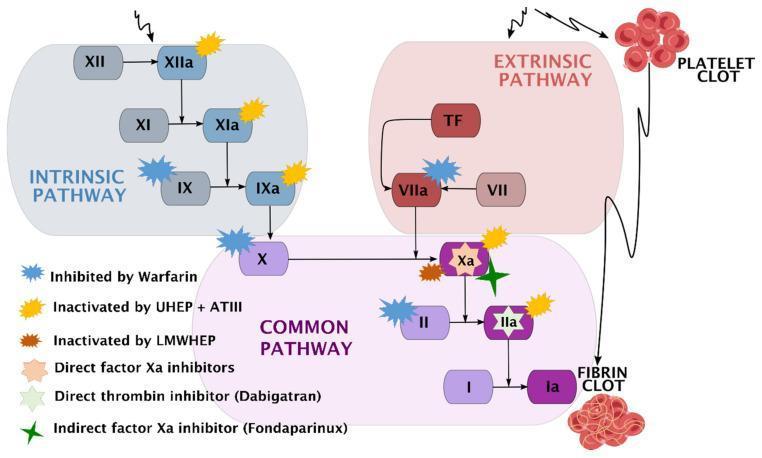
| Drug | Target | Pathway affected |
|---|---|---|
| Warfarin | Blocks Vit K-dependent synthesis (II, VII, IX, X) | Both |
| Heparin (UFH) + Antithrombin III | Inactivates IIa, Xa, IXa, XIa, XIIa | Both |
| LMWH (enoxaparin) | Primarily anti-Xa | Common + Intrinsic |
| Fondaparinux | Indirect Factor Xa inhibitor | Common |
| Rivaroxaban/Apixaban | Direct Factor Xa inhibitors | Common |
| Dabigatran | Direct thrombin (IIa) inhibitor | Common |
Extrinsic vs. Intrinsic — Quick Comparison
| Feature | Extrinsic | Intrinsic |
|---|---|---|
| Trigger | Tissue injury / TF exposure | Contact with negatively charged surface |
| Key initiator | Tissue Factor (III) + Factor VII | Factor XII, PK, HMWK |
| Speed | Fast (seconds) | Slower (minutes) |
| Main role in vivo | Primary initiation of clotting | Amplification of clot formation |
| Unique factors | VII | XII, XI, VIII (+ PK, HMWK) |
| Shared factor | IX (crossover from extrinsic) | — |
| Lab test | PT / INR | aPTT |
| Deficiency consequences | Factor VII deficiency → prolonged PT | Hemophilia A/B (VIII/IX deficiency) → prolonged aPTT + severe bleeding |
Modern View: Cell-Based Model
The classical "two-pathway" model is now understood to be an oversimplification. The current cell-based model (Sabiston Textbook of Surgery) describes three overlapping phases:
- Initiation — TF:VIIa complex (on fibroblasts/VSMC) activates small amounts of FXa and FIXa → trace thrombin
- Amplification — Trace thrombin activates platelets, Factor V, Factor VIII, and Factor XI → positive feedback
- Propagation — Full intrinsic tenase (IXa:VIIIa) on activated platelet surfaces generates a massive thrombin burst → stable fibrin clot
The intrinsic pathway is the main amplifier in vivo; the extrinsic pathway is the initiator. They are strongly interconnected: IXa and Xa from the intrinsic pathway can activate Factor VII of the extrinsic pathway, and conversely TF:VIIa activates Factor IX.
Sources:
- Harper's Illustrated Biochemistry, 32nd Ed., Figures 55-2 & 55-3
- Medical Physiology (Boron & Boulpaep), Table 18-4 & pp. 643–645
- Sabiston Textbook of Surgery, Chapter 100 (Hemostasis)
- Harrison's Principles of Internal Medicine, 22e, Figure 116-1
This is a shared conversation. Sign in to Orris to start your own chat.