Neck of femur fracture
Reading File
Finding Sources
Finding Sources
Searching PubMed
"femoral neck fracture" AND management
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed to write a comprehensive answer. Let me compile the full response.
Neck of Femur (NOF) Fracture
Overview
Fractures of the neck of the femur occur predominantly in the elderly, typically from low-energy falls, and are strongly associated with osteoporosis. They represent a major public health problem - estimates project 458,000 to over 1 million hip fractures per year in the US alone by 2050. Femoral neck fractures in young patients are a very different entity, usually resulting from high-energy mechanisms with associated injuries.
Anatomy and Blood Supply
The blood supply to the femoral head is the central concern in NOF fractures, as its disruption leads to the feared complication of avascular necrosis (AVN).
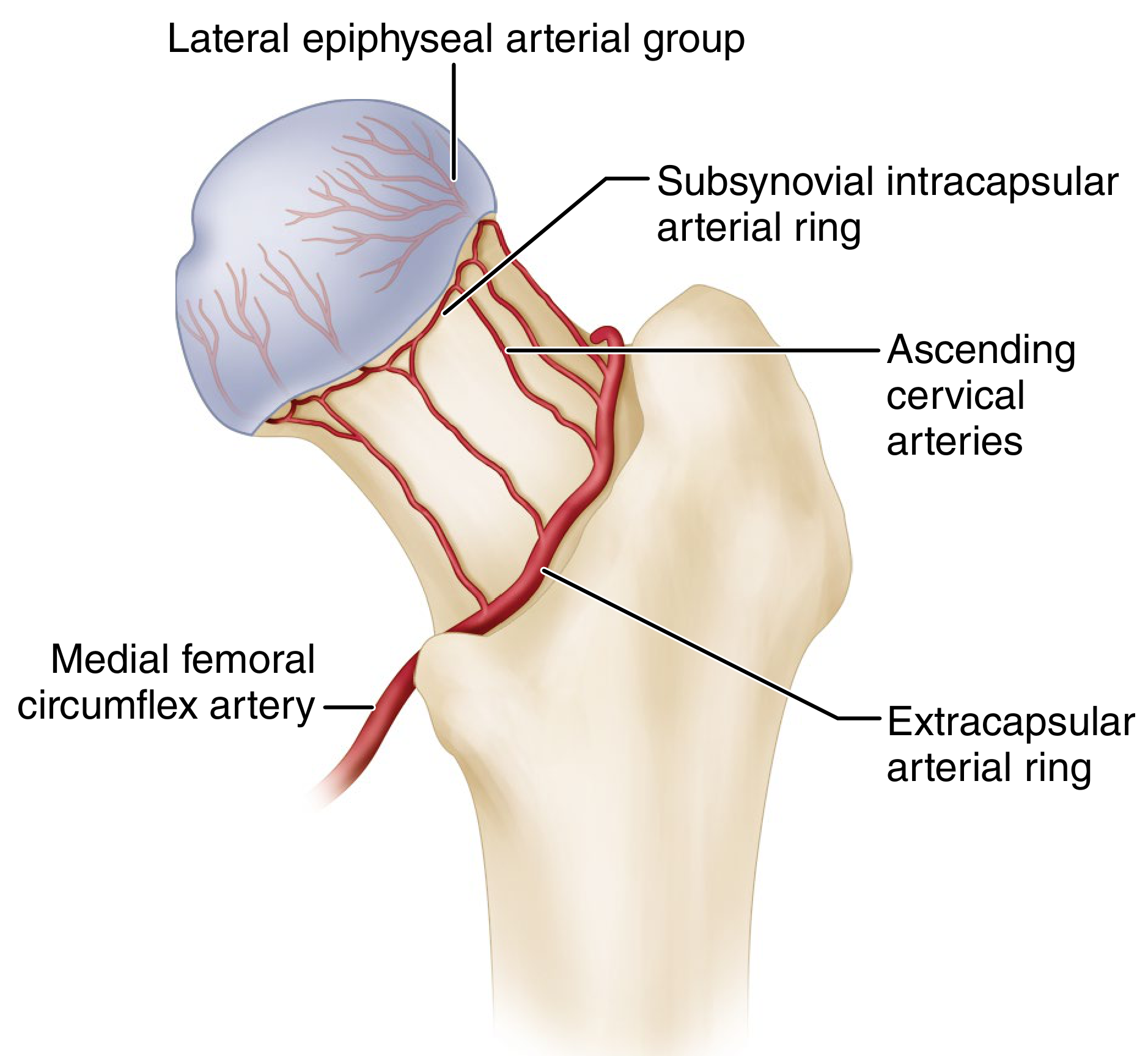
The blood supply comes from three main sources:
- Medial femoral circumflex artery (MFCA) - the dominant supply (~82% of femoral head perfusion). Its deep branch gives off the superior retinacular arteries that run in the retinacula of Weitbrecht along the femoral neck and perforate the bone 2-4 mm from the articular cartilage. These are the vessels most at risk in a subcapital fracture.
- Lateral femoral circumflex artery (LFCA) - contributes ~18%.
- Artery of the ligamentum teres (foveal artery) - minor contributor, may become more important in elderly with atherosclerotic disease attenuating the other sources.
With increasing age, medullary blood supply is attenuated due to fatty replacement of red marrow. In an intracapsular fracture, the retinacular vessels are transected, leaving the femoral head at high risk of avascular necrosis. This does NOT occur with intertrochanteric fractures (which are extracapsular), where the retinacular vessels remain intact.
The psoas major inserts onto the lesser trochanter - when the femoral neck is fractured, it loses its fulcrum (the femoral head in the acetabulum) and pulls the femur proximally and into external rotation, causing the classic clinical deformity.
Classification
1. Anatomical Location
- Subcapital - most common; highest risk of AVN
- Transcervical - mid-neck
- Basicervical - at the base of the neck; only 2-3% of all hip fractures; variable relationship to the capsule
Most fractures are subcapital. The exact anatomical location has not been shown to influence management or outcome - degree of displacement is the more important consideration.
2. Garden Classification (most widely used)
Based on degree of displacement on AP radiograph:
| Grade | Description |
|---|---|
| Garden I | Incomplete fracture (valgus impacted) |
| Garden II | Complete fracture, nondisplaced |
| Garden III | Complete fracture, partially displaced; trabecular patterns of head and acetabulum no longer aligned but neck-head contact maintained |
| Garden IV | Complete fracture, fully displaced; trabecular patterns have realigned (head sits neutral in acetabulum) |
Interobserver reliability between all four stages is low. In practice, most surgeons simplify to two groups: undisplaced (I/II) vs displaced (III/IV) - a distinction that drives the management decision. Note: Garden I/II fractures with ≥20° of posterior tilt on the lateral radiograph should not be treated as undisplaced.
3. Pauwels Classification
Based on the angle of the fracture line relative to horizontal - predicts biomechanical forces at the fracture site:
| Type | Angle | Forces |
|---|---|---|
| Type I | 0-30° | Compressive - favourable |
| Type II | 30-50° | Mixed |
| Type III | >50° | Shear - unfavourable, high risk of non-union |
A more vertical fracture line = greater shear forces = higher risk of fixation failure. Pauwels III fractures may require alternative fixation strategies (e.g., screw-side plate devices rather than cannulated screws alone).
4. OTA/AO Classification
Alphanumeric: femoral neck = 31-B
- 31-B1: Nondisplaced to minimally displaced subcapital
- 31-B2: Transcervical (basicervical, midcervical adduction, midcervical shear)
- 31-B3: Displaced nonimpacted subcapital (Garden III/IV)
Theoretically comprehensive but not popular in clinical practice due to complexity. Surgeons are able to reliably divide into three main groups only; within-subgroup agreement is poor.
Clinical Features
- History: Fall (elderly) or high-energy trauma (young). Groin/hip pain. Inability to weight-bear.
- Examination:
- Shortened limb
- Externally rotated leg (psoas and adductors acting on detached proximal fragment)
- Pain on passive rotation
- Impacted fractures may still allow limited weight-bearing
Investigations
- Plain X-ray pelvis AP + lateral hip: First-line. May miss occult or undisplaced fractures.
- MRI: Gold standard for occult hip fractures (e.g., can show hemarthrosis and undisplaced intracapsular fracture when X-ray is normal). CT is an alternative if MRI unavailable.
- Bloods: FBC, U&E, LFTs, Ca, Mg, vitamin D, glucose, coagulation screen
- ECG, CXR: Pre-operative assessment
- Bone health: Ask about previous fragility fractures and osteoporosis treatment
Preoperative Considerations
Surgery should be prompt - delay is associated with worse outcomes. The Association of Anaesthetists recommends surgery within 36 hours. Absolute medical criteria warranting delay include:
- Hb <80 g/L
- Na <120 or >150 mmol/L; K <2.8 or >6.0 mmol/L
- Uncontrolled diabetes
- Acute/uncontrolled left ventricular failure
- Correctable arrhythmia with ventricular rate >120/min
Frailty assessment (Clinical Frailty Scale, 1-9) is important - it predicts mortality and guides surgical decision-making.
Traction is no longer routinely recommended - studies show no benefit for pain relief or fracture reduction quality, and arteriographic evidence suggests it may reduce femoral head perfusion.
Regional nerve blocks (fascia iliaca, femoral nerve) are recommended for analgesia before and after surgery.
Management
The key surgical decision depends on:
- Patient age and physiological status (biological age, not chronological)
- Fracture displacement (Garden I/II vs III/IV)
- Pre-injury mobility and function
Undisplaced Fractures (Garden I/II)
Internal fixation is preferred in most patients:
- Cannulated cannulated screws (3 partially threaded screws) - standard technique
- Placed in inverted triangle configuration for maximum rotational control
- A 4th screw (diamond configuration) may be used for significant posterior comminution
- Goal: anatomic reduction + compression across fracture site
- Sliding hip screw (Dynamic Hip Screw) - alternative, especially for basicervical fractures
- Garden alignment index used to evaluate adequacy of reduction (AP: 160-180°; lateral: ~180°)
For Garden I/II with posterior tilt ≥20°, treat as displaced.
Non-operative management (touch weight-bearing) is an option for truly undisplaced fractures but carries higher risk of displacement - most authors prefer fixation.
Displaced Fractures (Garden III/IV)
In elderly patients (physiologically old):
- Hemiarthroplasty (femoral head replacement; acetabulum left native) - most common
- Cemented hemiarthroplasty preferred (lower rate of periprosthetic fracture and better early mobilization)
- Total hip arthroplasty (THA) - for active, well-mobilizing patients with pre-existing acetabular disease or good biological age
- Better functional outcomes than hemiarthroplasty in active patients, but higher early complication rate
- Recent evidence (2025 systematic review, PMID 41303766) shows THA carries higher thromboembolic risk than hemiarthroplasty
In young patients (<65 years / physiologically young):
- Internal fixation with urgent reduction is strongly preferred to preserve the native hip
- Closed reduction (Whitman technique: traction, abduction, extension, then internal rotation) - attempt 2-3 times maximum
- Open reduction via Smith-Petersen (anterior) or Watson-Jones (anterolateral) approach if closed fails
- Capsulotomy is considered in young patients to decompress the intracapsular hematoma and potentially reduce AVN risk (no conclusive proof but done quickly and safely)
- Fully threaded screws to prevent shortening once compression achieved
Complications
Non-union
- Incidence: ~9% in young patients (higher with Pauwels III)
- Causes: inadequate reduction, poor implant position, AVN, infection
- Treatment: valgus intertrochanteric osteotomy, bone grafting, or conversion to arthroplasty
Avascular Necrosis (AVN) / Osteonecrosis
- Most important complication - results from disruption of retinacular vessels
- Incidence in young patients: ~23% overall; 27% displaced, 14% nondisplaced (meta-analysis of 18 studies)
- May present months to years post-injury with collapse of femoral head
- Treatment: core decompression (early), vascularized fibular graft, or total hip arthroplasty (late)
- Recent meta-analysis (PMID 39581960) found global incidence of AVN in adolescents after femoral neck fracture surgery is significant
Fixation Failure
- Cutout of screws, especially with varus malreduction
- More common with high Pauwels angle fractures
Peri-prosthetic Fracture
- More common with uncemented stems
General Complications
- Delirium (most common postoperative complication in elderly; CAM or 4AT screening recommended)
- VTE (DVT/PE) - prophylaxis mandatory
- Chest infection, urinary tract infection
- Pressure ulcers
- Malnutrition
Postoperative Rehabilitation
- Weight bearing as tolerated from day 1 with a frame - the standard for all frail elderly patients. Elderly patients cannot effectively limit weight-bearing and restricting it leads to rapid deconditioning.
- Physiotherapy mobilization on day 1 postoperatively, at least daily thereafter
- Nutrition supplementation (high-protein)
- Osteoporosis treatment - fragility fracture is a mandatory trigger for bone protection therapy
- Falls assessment to reduce future fracture risk
Special Notes
Osteoporosis: NOF fractures in the elderly are osteoporotic fractures. Bone mineral density assessment and anti-resorptive therapy (bisphosphonates, denosumab) must be initiated during the admission.
Intertrochanteric vs Subcapital: An intertrochanteric fracture spares the retinacular vessels (extracapsular), so fixation is feasible without AVN risk. A subcapital fracture disrupts the blood supply, making arthroplasty appropriate in the elderly.
Sources: Campbell's Operative Orthopaedics 15th Ed 2026; Rockwood and Green's Fractures in Adults 10th Ed 2025; Gray's Anatomy for Students
Recent evidence note: A 2025 systematic review (PMID 41303766) confirms THA carries higher thromboembolic risk than hemiarthroplasty in NOF fracture patients - factor this into the THA-vs-hemiarthroplasty decision in high-VTE-risk patients.
This is a shared conversation. Sign in to Orris to start your own chat.