Hi
Hi! How can I help you today?
Malaria microbiology
Reading File
Finding Sources
Searching PubMed
"malaria" AND "Plasmodium"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive answer. Here is the full review of malaria microbiology.
Malaria - Microbiology
The Organism
Malaria is caused by Plasmodium species, which are coccidian/sporozoan (Apicomplexa) parasites of blood cells. Like other coccidia, they require two hosts: the mosquito for sexual reproduction and humans/animals for asexual reproduction. They account for ~216 million episodes with approximately 500,000 deaths annually, 90% of which occur in Africa.
Five Human Species
| Species | Disease | Features |
|---|---|---|
| P. falciparum | Malignant tertian malaria | Most dangerous; 48-hr cycle |
| P. vivax | Benign tertian malaria | 48-hr cycle; hypnozoites; Duffy antigen receptor |
| P. ovale | Benign tertian/ovale malaria | 48-hr cycle; hypnozoites |
| P. malariae | Quartan malaria | 72-hr cycle |
| P. knowlesi | Simian/quotidian malaria | 24-hr cycle (shortest); zoonosis from macaques in SE Asia |
- Medical Microbiology 9e, Table 73.1
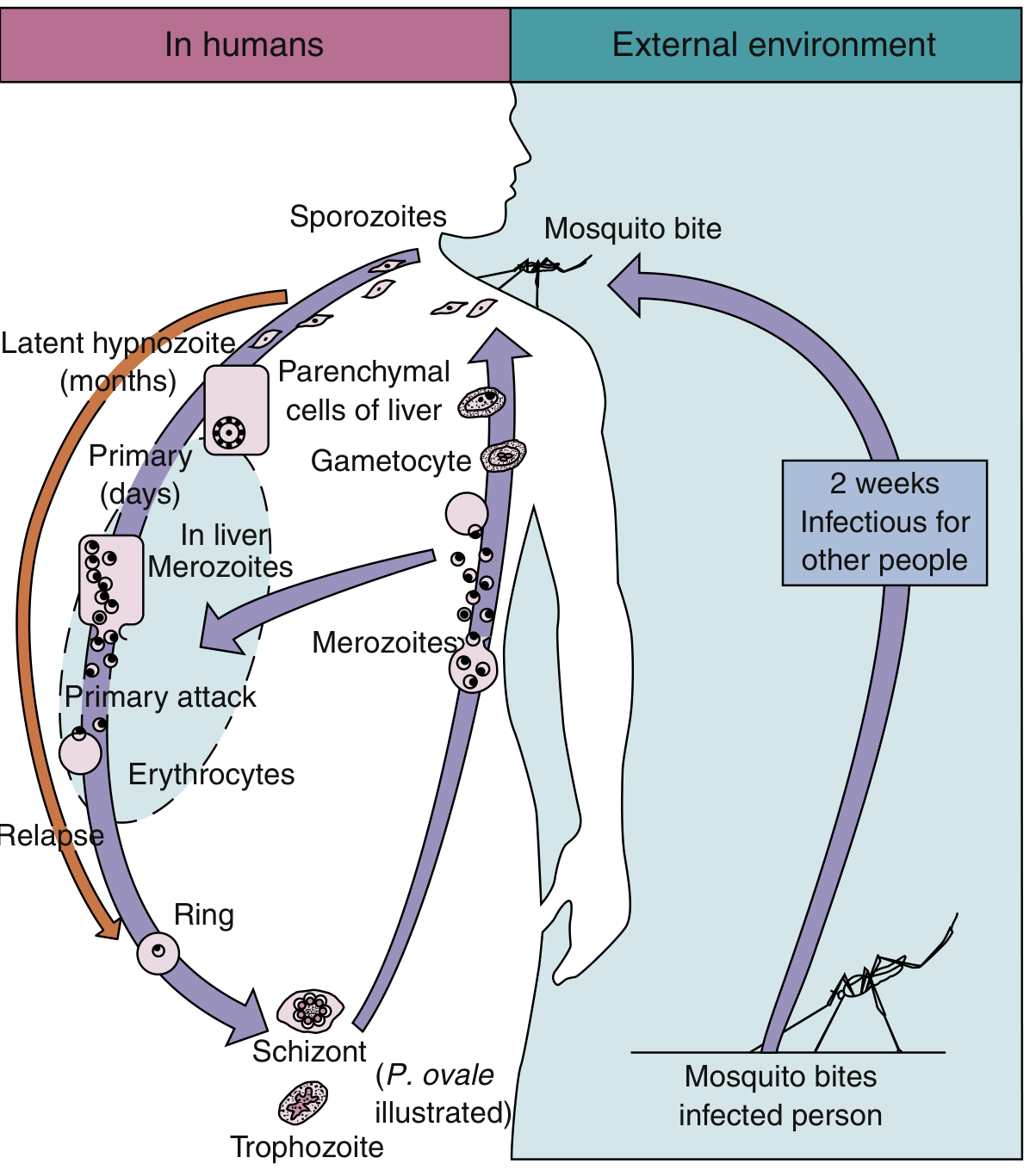
Life Cycle
Step 1 - Mosquito Bite (Sporozoite Inoculation)
An infected female Anopheles mosquito introduces sporozoites into the human bloodstream via its saliva. Within minutes, sporozoites travel to the liver.
Step 2 - Hepatic (Exoerythrocytic) Stage
Two sporozoite surface proteins - thrombospondin-related adhesive protein and circumsporozoite protein - bind to proteoglycans (heparan sulfate) on hepatocyte surfaces. The sporozoites enter hepatocytes and differentiate into merozoites over 8-25 days (varies by species).
Key feature - Hypnozoites: P. vivax and P. ovale can establish dormant hepatic forms called hypnozoites ("sleeping forms"). These can persist for months to years and cause relapse of infection long after the initial illness. P. malariae does not form hypnozoites but can cause recrudescence from persistent low-level blood-stage infection.
Step 3 - Erythrocytic Stage
After infected hepatocytes rupture, merozoites are released into the bloodstream. A lectin-like molecule on the merozoite surface binds to sialidated glycophorin (a red cell transmembrane protein), allowing invasion into RBCs within a "digestive vacuole."
Inside the RBC, the parasite progresses through:
- Ring form (early trophozoite)
- Trophozoite (mature; digests hemoglobin producing hemozoin/malarial pigment)
- Schizont (divides to form up to 24 merozoites depending on species)
- Merozoite release - rupture of the RBC liberates merozoites to infect new RBCs
Some trophozoites differentiate into male and female gametocytes instead, which are taken up by a feeding mosquito to restart the sexual cycle.
Step 4 - Mosquito Stage (Sexual Cycle)
In the mosquito midgut, male and female gametocytes fuse to form an oocyst on the gut wall. Sporozoites develop within the oocyst and migrate to the mosquito's salivary glands, ready to infect a new human host (~2 weeks).
Life cycle diagram (Robbins Pathology, Fig. 10.8 - P. falciparum):

Life cycle overview (Medical Microbiology 9e, Fig. 73.1 - showing hypnozoite relapse pathway):
Pathogenesis
P. falciparum - Mechanisms of Severe Disease
P. falciparum is uniquely dangerous because of cytoadherence:
- Infected RBCs express PfEMP1 (Plasmodium falciparum Erythrocyte Membrane Protein 1), an adhesion molecule that concentrates in knob-like extensions on the RBC surface.
- PfEMP1 binds to endothelial adhesion molecules - ICAM-1, VCAM-1, and CD36 - causing parasitized RBCs to arrest in capillary beds (sequestration).
- This prevents the parasite from circulating through the spleen (where it would be destroyed) but causes microvascular obstruction.
In cerebral malaria, this process involves cerebral vessels, which become engorged and occluded - mainly affecting children in endemic areas, with high fatality.
Fever Periodicity
Episodic shaking chills and fever coincide with synchronized RBC lysis releasing merozoites:
- 24 hours - P. knowlesi (quotidian fever)
- 48 hours - P. vivax, P. ovale, P. falciparum (tertian fever)
- 72 hours - P. malariae (quartan fever)
Anemia
Hemolytic anemia from direct RBC destruction. A characteristic brown pigment called hematin (hemozoin) - derived from hemoglobin digestion - accumulates in and discolors the spleen, liver, lymph nodes, and bone marrow.
Species-Specific Features
P. vivax
- Invades only young, immature erythrocytes (reticulocytes)
- Receptor: Duffy blood group antigen (though Duffy-negative individuals in Madagascar have recently been found to be susceptible via an unknown mechanism)
- RBC features: enlarged RBCs, Schüffner dots (pink granules), amoeboid ring-shaped trophozoite, schizonts with up to 24 merozoites, round gametocytes
- Causes hypnozoite-mediated relapse
- Most geographically widespread species (tropics, subtropics, temperate zones); >80% of cases in South America and SE Asia
- Despite the "benign" label, can cause severe complications: delirium, seizures, renal failure, pulmonary edema, ARDS - similar to falciparum malaria
P. falciparum
- Invades RBCs of all ages
- Causes highest parasite burden and most deaths
- Only species with knobs on infected RBCs (PfEMP1)
- Peripheral smear: multiple ring forms per RBC, "appliqué/accolé" forms, banana-shaped gametocytes (the only stage seen in peripheral blood normally)
- No hypnozoites; no relapse (but can recrudesce)
P. malariae
- Invades old erythrocytes
- 72-hour (quartan) cycle
- Smear: "band forms" (bar forms), "rosette" schizonts with up to 8-10 merozoites
- No hypnozoites; can persist for decades as low-level blood infection (recrudescence)
- Associated with nephrotic syndrome in children (immune complex deposition)
P. ovale
- Similar to P. vivax; forms hypnozoites
- Schizonts with oval/fimbriated RBCs
P. knowlesi
- Zoonosis from macaques in Southeast Asia
- 24-hour cycle - can cause rapid, severe disease
- Can infect RBCs at all developmental stages
- Resembles P. malariae on smear (causes diagnostic confusion)
Laboratory Diagnosis
| Method | Details |
|---|---|
| Thick & thin blood smear | Gold standard; thick smear for detection, thin smear for species ID; Giemsa stain |
| RDT (Rapid Diagnostic Test) | Detects P. falciparum HRP2 antigen or pan-Plasmodium pLDH; fast, field-friendly |
| PCR | Most sensitive; useful for low parasitemia and mixed infections |
| Serology | Cross-reacts among species; used for epidemiology, not acute diagnosis |
Note: RDTs are not recommended for P. malariae diagnosis specifically.
Morphology Summary (Blood Smear)
| Feature | P. vivax | P. falciparum | P. malariae | P. ovale |
|---|---|---|---|---|
| RBC size | Enlarged | Normal | Normal/small | Oval, fimbriated |
| Schüffner dots | Yes | No (Maurer clefts) | No | Yes |
| Gametocyte shape | Round | Banana/crescent | Round | Round |
| Max merozoites in schizont | ~24 | ~24 | ~8-10 | ~8 |
| Distinctive feature | Amoeboid trophozoite | Multiple rings/cell; appliqué forms | Band forms | Oval RBCs |
Key Virulence Factors
- Circumsporozoite protein - hepatocyte adhesion; target of the RTS,S (Mosquirix) vaccine
- PfEMP1 - cytoadherence and antigenic variation (encoded by ~60 var genes, allowing immune evasion)
- Hemozoin (malaria pigment) - activates Toll-like receptor 9, driving systemic inflammation and fever
- Rosetting - P. falciparum-infected RBCs bind uninfected RBCs, worsening microvascular obstruction
Recent evidence alert: A 2024 review on artemisinin-resistant malaria (White & Chotivanich, Clin Microbiol Rev) highlights emerging resistance to artemisinin in P. falciparum (kelch13 mutations), particularly in SE Asia and now Africa - a significant update to treatment considerations. A 2025 broad review "Malaria: past, present, and future" provides current epidemiology and vaccine/drug pipeline updates.
- Medical Microbiology 9e (Murray), Ch. 73
- Robbins & Kumar Basic Pathology, Ch. 10
This is a shared conversation. Sign in to Orris to start your own chat.