Dynamic hyperinflation full details for md exams 10 marks
Reading File
Finding Sources
Finding Sources
Searching PubMed
"dynamic hyperinflation" COPD mechanism
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough MD-exam answer. Here is the complete, structured response:
Dynamic Hyperinflation - Complete Notes for MD Examination (10 Marks)
1. Definition
Dynamic hyperinflation (DH) is a progressive increase in end-expiratory lung volume (EELV) above the static functional residual capacity (FRC), occurring whenever there is insufficient time for complete exhalation before the next breath begins.
- It is synonymous with intrinsic PEEP (iPEEP / auto-PEEP)
- Auto-PEEP = alveolar pressure minus airway-opening pressure at end-expiration
- DH = the volume manifestation; auto-PEEP = the pressure manifestation of the same phenomenon
"Dynamic hyperinflation is an increase in end-expiratory lung volume above the value that would be obtained if there was complete exhalation to the static functional residual capacity." - Goldman-Cecil Medicine
2. Pathophysiology / Mechanism
2a. Core Mechanism
Under normal conditions, expiration is passive and returns EELV to static FRC. DH occurs when:
- Expiratory flow limitation (EFL) is present - expiratory flow does not increase despite increasing alveolar-to-atmospheric pressure gradient (as in COPD/asthma)
- Expiratory time is insufficient - the next inhalation begins before complete exhalation
- Each successive breath adds a "residual volume increment" - leading to a progressively rising EELV
2b. Determinants of Auto-PEEP / DH (4 key factors):
| Factor | Mechanism |
|---|---|
| High minute ventilation | Increased respiratory rate shortens expiratory time |
| Increased expiratory airway resistance | Slows expiratory flow (COPD, asthma, mucus) |
| Increased respiratory system compliance | Lung empties more slowly (emphysema) |
| Decreased expiratory time (short I:E ratio) | Less time for passive recoil |
In addition, tonic inspiratory muscle activity at end-expiration and positive-pressure ventilation settings (high RR, high tidal volume) further exacerbate DH.
2c. PEEP₁ (intrinsic PEEP)
- The resulting positive end-expiratory alveolar pressure is called PEEP₁ or auto-PEEP
- It acts as an inspiratory threshold load - the patient must first overcome PEEP₁ before generating any inspiratory flow
- The ventilator does not "see" this pressure because the pressure drop is upstream of where airway pressure is measured in the circuit
3. Causes / Clinical Settings
3a. Obstructive Airway Diseases (commonest)
- COPD (emphysema + chronic bronchitis) - loss of elastic recoil + airflow obstruction
- Acute severe asthma (status asthmaticus) - bronchoconstriction + air-trapping
- Bronchiectasis - secretion-related obstruction
3b. Mechanical Ventilation Settings
- High respiratory rate (RR > 20/min) - shortened expiratory time
- Large tidal volumes
- Short I:E ratio (insufficient expiratory phase)
- High minute ventilation
3c. Other
- Tachypnea from any cause (pain, anxiety, hypoxemia) - even without intrinsic lung disease, a very high respiratory rate can produce DH
- Post-exercise in COPD patients
4. Consequences / Physiological Effects
4a. Respiratory Effects
| Effect | Mechanism |
|---|---|
| Increased work of breathing | Raised EELV increases elastic recoil forces; auto-PEEP acts as threshold load |
| Dyspnea / air hunger | Combination of increased WOB + respiratory muscle inefficiency |
| Respiratory muscle fatigue | Diaphragm operates at shorter-than-optimal length (flattened); zone of apposition reduced |
| Alveolar overdistension | Risk of barotrauma, pneumothorax |
| Decreased compliance (apparent) | Respiratory system compliance appears falsely low if auto-PEEP is not corrected |
| Increased dead space ventilation | Overdistended alveoli compromise perfusion |
| Hypercapnia / respiratory failure | Progressive CO₂ retention from WOB + dead space |
4b. Cardiovascular Effects
- Elevated intrathoracic pressure raises right atrial pressure
- Decreased venous return - reduced driving pressure for systemic venous return
- Right ventricular strain - increased RV afterload
- Hypotension - especially immediately after intubation/sedation when compensatory mechanisms are blunted
4c. Ventilator-Specific Effects
- Ineffective triggering - patient must generate effort to overcome auto-PEEP before the ventilator detects the inspiratory effort; "failed efforts" occur in >10% of breathing attempts in ~25% of patients on pressure support
- Underestimation of respiratory rate - the ventilator's counted rate is lower than the patient's actual rate
- Falsely low compliance measurements - if auto-PEEP is not factored in
5. Measurement / Detection
5a. Clinical Signs
- Flow at end-expiration remains detectable on the flow-time waveform (flow does not return to zero)
- End-expiratory flow velocity > 0 on the ventilator screen
- Patient making inspiratory efforts that fail to trigger the ventilator (ineffective efforts)
- Tachypnea with pursed-lip breathing
5b. Bedside Measurement (Mechanically Ventilated Patient)
End-expiratory occlusion technique:
- In a patient with no spontaneous breathing effort, occlude the expiratory port at end-expiration
- Alveolar, central airway, and ventilator circuit pressures equilibrate
- Auto-PEEP = measured pressure - set PEEP (read on the ventilator manometer)
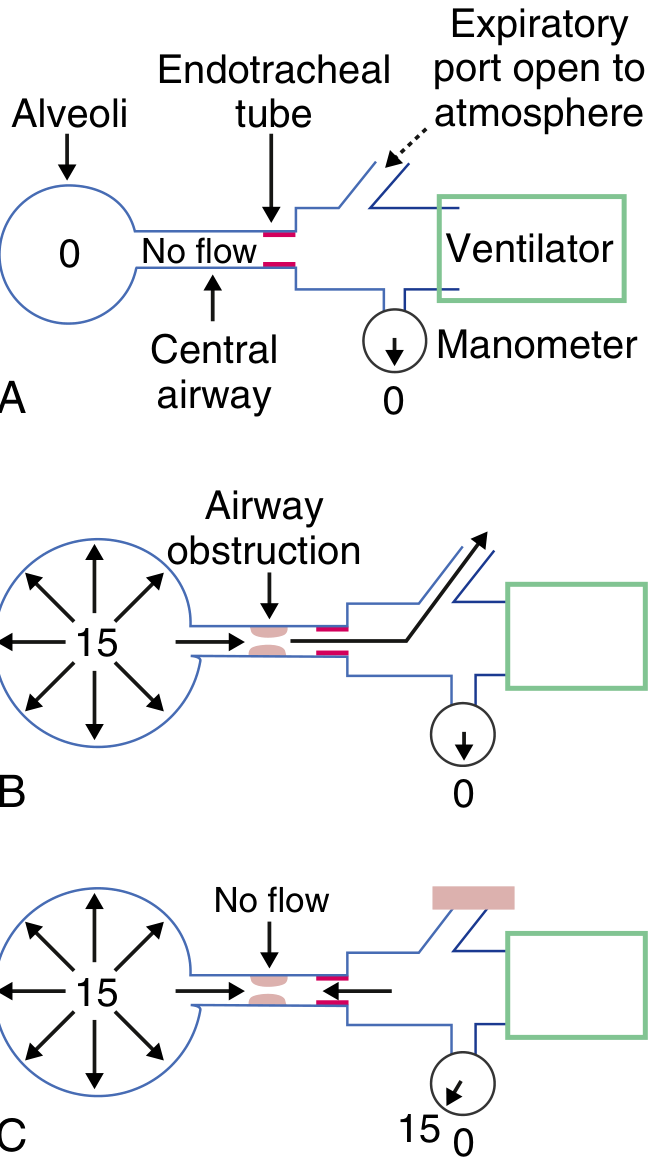
Goldman-Cecil Medicine - E-Fig 91-1: Auto-PEEP measurement. Panel A = normal; Panel B = dynamic obstruction, port open; Panel C = port occluded, auto-PEEP reads 15 cmH₂O
Prolonged expiration technique:
- Perform a prolonged expiration (20-30 seconds) to atmosphere
- Volume of gas released = volume of dynamic hyperinflation
5c. Spirometric/Exercise Surrogate
- Inspiratory capacity (IC) progressively falls as EELV rises during exercise
- IC is the most practical marker of dynamic hyperinflation during exercise testing
- IC = TLC - EELV (if TLC is constant, ↓IC = ↑EELV)
6. Clinical Implications in COPD
- Progressive exercise limitation in COPD is driven largely by DH
- DH raises WOB and exacerbates dyspnea during exertion
- Anxiety episodes can cause tachypnea → DH → more dyspnea → a vicious cycle
- Interventions reducing DH improve exercise capacity:
- Inhaled bronchodilators (LABA/LAMA) - reduce airway resistance
- Oxygen supplementation - reduces minute ventilation demand
- Pursed-lip breathing - slows respiratory rate, prolongs expiratory phase
- Lung volume reduction surgery (LVRS) - improves elastic recoil and reduces DH
- Pulmonary rehabilitation
7. Management
7a. Non-Ventilated Patient (COPD/Asthma)
- Bronchodilators (SABA + SAMA nebulization) - reduce airway resistance and time constant
- Systemic corticosteroids - reduce airway inflammation and secretions
- Heliox - low-density gas mixture, reduces turbulent flow, improves expiratory flow
- Pursed-lip breathing - self-PEEP stenting of airways, slows RR, prolongs expiration
- NIV/BiPAP - external PEEP offsets auto-PEEP, reduces inspiratory threshold load
- Positioning - upright reduces abdominal load on diaphragm
7b. Mechanically Ventilated Patient
Core principle: minimize minute ventilation + maximize expiratory time
| Strategy | Rationale |
|---|---|
| Low respiratory rate (10-14/min) | Most effective measure to reduce DH; rates <10 not recommended (causes unacceptable hypercapnia) |
| Low tidal volume (≤ 8 mL/kg predicted body weight) | Reduces minute ventilation |
| Prolonged expiratory time (high I:E ratio, e.g., 1:3 or 1:4) | Allows more complete lung emptying |
| Permissive hypercapnia | Accept elevated PaCO₂; target pH >7.2 rather than normalizing CO₂ |
| Bronchodilators + suctioning | Reduce expiratory resistance |
| Applied external PEEP (extrinsic PEEP) | Set at ~75-85% of measured auto-PEEP to "stent" the airway; reduces inspiratory threshold load without worsening DH |
| Sedation and paralysis (initial phase) | Eliminates tonic respiratory muscle activity; allows controlled low-RR ventilation |
Permissive hypercapnia target: Accept PaCO₂ elevation so long as pH > 7.2
Ventilator settings in acute COPD (Rosen's Emergency Medicine):
- Mode: Volume assist-control
- RR: 10-14/min
- TV: ≤ 8 mL/kg predicted BW
- Inspiratory time: 0.8-1.0 seconds
- PEEP: 5 cmH₂O
- SpO₂ target: 88-92%
8. Auto-PEEP and Triggering Failure (High-Yield for Exams)
- If auto-PEEP = 10 cmH₂O and trigger sensitivity is set at -2 cmH₂O, the patient must generate -12 cmH₂O effort to trigger the ventilator
- Failed triggers = patient effort does not produce a breath; seen on flow-time waveform as small deflections without delivered breaths
- Solution: apply external PEEP ≈ 75-85% of auto-PEEP to reduce the threshold the patient must overcome
9. Summary - High-Yield Points for Exam
| Point | Key Fact |
|---|---|
| Definition | ↑ EELV above static FRC due to incomplete expiration |
| Pressure correlate | Auto-PEEP (intrinsic PEEP) |
| Main cause | COPD, acute severe asthma, MV with high RR |
| Best bedside measure (MV) | End-expiratory occlusion pressure |
| Surrogate during exercise | ↓ Inspiratory capacity (IC) |
| Cardiovascular danger | ↓ Venous return → hypotension (esp. post-intubation) |
| Ventilator management | ↓ RR (10-14/min), ↓ TV, ↑ E time, permissive hypercapnia |
| Triggering failure cause | Patient must overcome auto-PEEP before triggering |
| Treatment (pharmacologic) | Bronchodilators, steroids, heliox |
| Non-pharmacologic | Pursed-lip breathing, NIV, LVRS |
Sources:
- Goldman-Cecil Medicine International Edition (2 vol.), p. 1064-1065
- Murray & Nadel's Textbook of Respiratory Medicine (2 vol.) - Expiratory Flow Limitation chapter, p. 716
- Fishman's Pulmonary Diseases and Disorders (2 vol.) - Natural History of COPD chapter
- Murray & Nadel's - Oxygen Cost of Breathing chapter
- Rosen's Emergency Medicine - Respiratory Failure & Invasive Ventilation chapter, p. 948
This is a shared conversation. Sign in to Orris to start your own chat.