Basic definition of pulmonary circulation
Reading File
Finding Sources
Reading File
Reading File
Reading File
Here is a clear, textbook-grounded definition of pulmonary circulation:
Pulmonary Circulation - Basic Definition
Pulmonary circulation is the portion of the cardiovascular system that carries deoxygenated blood from the right side of the heart to the lungs for gas exchange, and returns oxygenated blood back to the left side of the heart.
The Circuit (Step by Step)
- Right ventricle contracts and ejects deoxygenated blood into the pulmonary artery
- The pulmonary artery enters each lung at the hilum, traveling alongside the bronchi and branching with each airway generation down to the level of the respiratory bronchioles
- Blood flows through pulmonary arterioles → capillaries (surrounding the alveoli) where:
- CO₂ diffuses out of blood into the alveolar air (exhaled)
- O₂ diffuses from alveolar air into the blood
- Oxygenated blood drains into pulmonary venules → pulmonary veins, which return it to the left atrium
Key Characteristics
| Feature | Pulmonary Circulation | Systemic Circulation |
|---|---|---|
| Pressure | Low (mean ~15 mmHg) | High (mean ~95 mmHg) |
| Capillary pressure | ~10 mmHg | ~25 mmHg |
| Function | Gas exchange (lungs) | O₂/nutrient delivery (body) |
| Vessel wall | Thin, compliant | Thick, muscular |
The pulmonary circuit is entirely a low-pressure system - mean arterial pressures normally do not exceed 15 mmHg and capillary pressures do not rise above 10 mmHg. This is important because high capillary pressure would cause fluid to leak into alveoli (pulmonary edema).
Unique Feature: Hypoxic Vasoconstriction
Unlike systemic vessels (which dilate in response to low O₂), pulmonary arterioles constrict when local O₂ is low. This is called hypoxic pulmonary vasoconstriction (HPV). It serves a protective purpose: it diverts blood away from poorly ventilated (hypoxic) lung regions toward well-ventilated areas, optimizing the match between ventilation and perfusion (V/Q matching).
Anatomy Highlights (from Murray & Nadel's)
- Pulmonary arteries travel alongside the bronchi at every airway generation
- Pulmonary veins, by contrast, travel away from airways in the peripheral connective tissue
- Each small pulmonary artery supplies a specific volume of respiratory tissue; each vein drains portions of several zones
- Capillary volume: 60-200 mL, with a gas exchange surface area of 50-70 m²
Sources: Costanzo Physiology 7th Ed.; Medical Physiology (Boron & Boulpaep); Murray & Nadel's Textbook of Respiratory Medicine
Write a easy summary on physiological anatomy of the pulmonary circulation system according to guyton and hall
Finding Sources
Finding Sources
Finding Sources
Reading File
I have all the content needed directly from Guyton and Hall. Here is the easy summary:
Physiological Anatomy of the Pulmonary Circulation System
(According to Guyton and Hall - Medical Physiology)
The Lung Has TWO Circulations
The lung is unique - it actually receives blood from two separate circulations:
| Circulation | Pressure | Flow | Purpose |
|---|---|---|---|
| Bronchial (systemic) | High pressure | Low flow | Feeds lung tissues (bronchi, connective tissue) |
| Pulmonary | Low pressure | High flow | Gas exchange at alveoli |
1. Pulmonary Blood Vessels
Pulmonary Artery:
- Extends only 5 cm beyond the apex of the right ventricle, then splits into right and left branches for each lung
- Its wall is only one-third the thickness of the aorta - much thinner and more delicate
- All pulmonary arteries (even small ones) have larger diameters than equivalent systemic arteries
- Because the vessels are thin and wide, the whole pulmonary arterial tree is very distensible (compliant) - compliance averages ~7 mL/mmHg, similar to the entire systemic arterial tree
- This high compliance lets the pulmonary arteries easily accommodate the stroke volume from the right ventricle without a big pressure spike
Pulmonary Veins:
- Also short - they immediately empty blood into the left atrium
2. Bronchial Blood Vessels
- Small bronchial arteries branch off the thoracic aorta (systemic blood supply)
- They carry oxygenated blood - about 1-2% of total cardiac output
- They supply the supporting tissues: connective tissue, septa, large and small bronchi
- After nourishing these tissues, this blood drains into the pulmonary veins (not back to the right atrium)
- This means the left ventricle outputs ~1-2% more blood than the right ventricle at any given time
3. Lymphatics
- Lymph vessels run throughout the lung's supportive tissues, starting around the terminal bronchioles
- They travel to the hilum of the lung and drain mainly into the right thoracic lymph duct
- They serve two important purposes:
- Remove particulate matter (dust, debris) that enters the alveoli
- Carry away leaked plasma proteins from lung capillaries - this actively prevents pulmonary edema
Simple Summary Diagram
Right Ventricle
↓
Pulmonary Artery (thin walls, large diameter, very distensible)
↓ splits into Right & Left branches
Alveolar Capillaries → Gas Exchange (O₂ in, CO₂ out)
↓
Pulmonary Veins (short)
↓
Left Atrium → Left Ventricle → Body
Bronchial arteries (from aorta) → feed lung tissues → drain into pulmonary veins
Lymphatics → run alongside bronchioles → remove proteins & particles → prevent edema
Why This Anatomy Matters
The thin, wide, distensible design of the pulmonary vessels keeps blood pressure very low in the lungs. This is essential - if pulmonary capillary pressure were too high, fluid would be forced into the alveoli (pulmonary edema), blocking gas exchange.
Source: Guyton and Hall Textbook of Medical Physiology, Chapter 39 - Pulmonary Circulation, Pulmonary Edema, and Pleural Fluid
Physiological anatomy of the pulmonary circulation system easy one shot
Reading File
Here is the complete one-shot easy summary straight from Guyton and Hall:
Physiological Anatomy of the Pulmonary Circulation System
(Guyton & Hall - Medical Physiology)
The Lung Has 2 Circulations
| Bronchial Circulation | Pulmonary Circulation | |
|---|---|---|
| Pressure | High | Low |
| Flow | Low (1-2% cardiac output) | High (entire cardiac output) |
| Blood type | Oxygenated | Deoxygenated |
| Job | Feed lung tissues | Gas exchange |
Part 1 - Pulmonary Blood Vessels
Pulmonary Artery
- Leaves the right ventricle, extends only 5 cm, then splits into right and left branches
- Wall is only 1/3 the thickness of the aorta
- All pulmonary arteries (even small ones) have wider diameters than equivalent systemic arteries
- Because they are thin + wide = very distensible (stretchy)
- Compliance averages ~7 mL/mmHg (same as the entire systemic arterial tree)
- This stretchiness lets them easily absorb each stroke volume without a big pressure rise
Pulmonary Veins
- Also very short
- Drain directly into the left atrium
Part 2 - Bronchial Blood Vessels
- Small bronchial arteries branch off the thoracic aorta
- Carry oxygenated blood = only 1-2% of cardiac output
- Supply the lung's support structures: connective tissue, septa, bronchi
- After use, this blood drains into the pulmonary veins (NOT back to the right atrium)
- Result: left ventricular output is 1-2% more than right ventricular output at all times
Part 3 - Lymphatics
- Found in all supportive tissues of the lung
- Start around terminal bronchioles → travel to the hilum → drain into the right thoracic lymph duct
- Two jobs:
- Remove dust and particulate matter from alveoli
- Drain away leaked plasma proteins from lung capillaries → prevents pulmonary edema
One-Line Takeaway for Each Component
Pulmonary artery - thin, wide, stretchy → absorbs stroke volume at low pressure Pulmonary veins - short → quick return to left atrium Bronchial vessels - feed lung tissues, drain into pulmonary veins Lymphatics - clean the lung, prevent fluid buildup
Source: Guyton and Hall Textbook of Medical Physiology, Chapter 39
Pressures in the pulmonary circulatory system one shot easy
Reading File
Loading Image
Loading Image
Here is the complete one-shot easy summary:
Pressures in the Pulmonary Circulatory System
(Guyton & Hall - Medical Physiology)
The Big Picture First
The entire pulmonary system runs at very low pressure compared to the systemic circulation. Think of it as a gentle, low-resistance loop - just enough pressure to push blood through the lungs and back.
Pressure at Each Station
1. Right Ventricle
- Systolic: ~25 mmHg (only 1/5th of the left ventricle's ~120 mmHg)
- Diastolic: ~0-1 mmHg
- The right ventricle is a low-pressure pump - it does far less work than the left ventricle
2. Pulmonary Artery
- Systolic: 25 mmHg (matches right ventricle during contraction)
- Diastolic: 8 mmHg
- Mean: 15 mmHg
- When the pulmonary valve closes after systole, right ventricular pressure drops sharply - but pulmonary artery pressure falls slowly because blood continues flowing through the lungs
3. Pulmonary Capillaries
- Mean: ~7 mmHg
- Extremely low - this is intentional. If capillary pressure were too high, fluid would be forced into the alveoli causing pulmonary edema
4. Left Atrium & Pulmonary Veins
- Mean: ~2 mmHg (range: 1-5 mmHg)
- The lowest pressure in the whole circuit - blood drains easily into the left atrium
All Pressures at a Glance
| Location | Systolic | Diastolic | Mean |
|---|---|---|---|
| Right Ventricle | 25 mmHg | 0-1 mmHg | - |
| Pulmonary Artery | 25 mmHg | 8 mmHg | 15 mmHg |
| Pulmonary Capillaries | - | - | 7 mmHg |
| Left Atrium | - | - | 2 mmHg |
The Guyton Diagrams
Fig. 39.1 - Right ventricle vs. aorta pressure comparison:
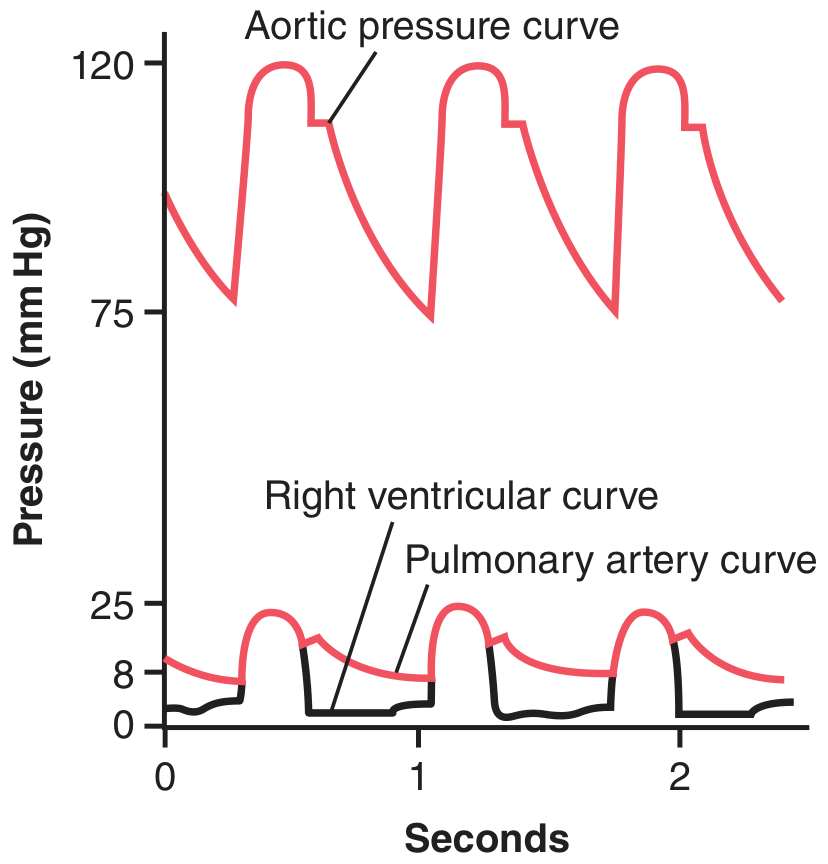
Notice how tiny the right ventricle/pulmonary artery pressures (bottom curves, peaking at ~25 mmHg) are compared to the aortic pressure (top curve, ~120 mmHg).
Fig. 39.2 - Pressure drop across the pulmonary circuit:
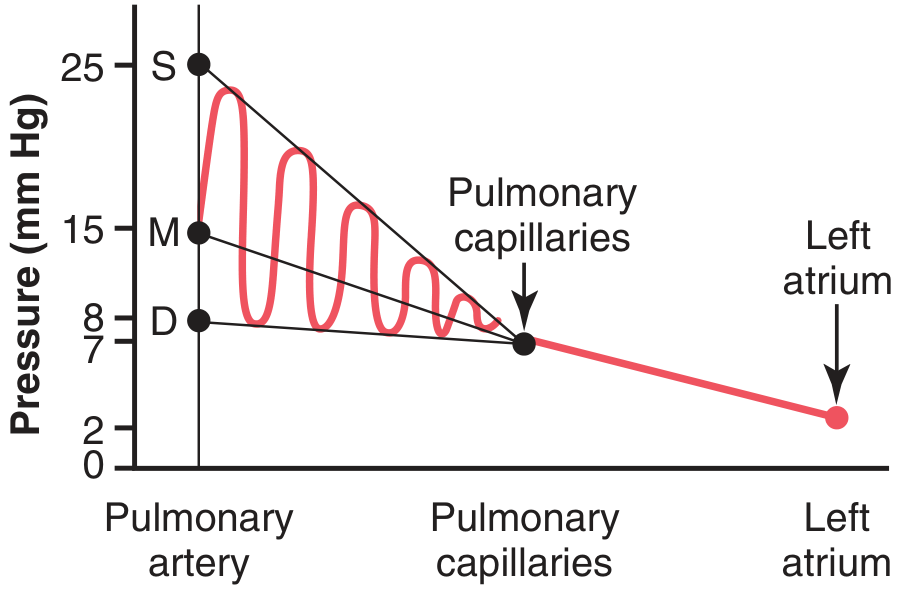
Pressure falls steadily from pulmonary artery (S=25, M=15, D=8) → capillaries (~7) → left atrium (~2).
How Left Atrial Pressure is Measured (Wedge Pressure)
The left atrium is hard to catheterize directly. Instead, doctors use the pulmonary wedge pressure:
- A catheter is passed through a peripheral vein → right atrium → right ventricle → pulmonary artery → wedged into a small pulmonary artery branch
- When wedged, blood flow stops and the catheter "sees" pressure from the pulmonary capillaries onward
- Wedge pressure reads ~5 mmHg - only 2-3 mmHg higher than true left atrial pressure
- This technique is used clinically to detect left heart failure (rising left atrial pressure shows up as rising wedge pressure)
Why Low Pressure Matters
- Pulmonary capillary pressure (~7 mmHg) stays below plasma oncotic pressure (~28 mmHg)
- This means fluid is held inside the capillaries and does NOT leak into alveoli
- If left atrial pressure rises (e.g., left heart failure) → backs up into pulmonary capillaries → pressure exceeds oncotic pressure → pulmonary edema
One-Line Memory Aid
RV = 25/1 → PA = 25/8 (mean 15) → Capillaries = 7 → Left Atrium = 2 Pressure keeps dropping as blood flows toward the left heart.
Source: Guyton and Hall Textbook of Medical Physiology, Chapter 39
Blood volume of the lungs easy summardy
Finding Sources
Reading File
Blood Volume of the Lungs
(Guyton & Hall - Medical Physiology, Chapter 39)
Normal Blood Volume
- Total lung blood volume = ~450 mL = about 9% of total body blood volume
- How is it distributed?
| Location | Volume |
|---|---|
| Pulmonary capillaries | ~70 mL |
| Pulmonary arteries | ~190 mL (half of remaining) |
| Pulmonary veins | ~190 mL (half of remaining) |
Lungs Act as a Blood Reservoir
The lungs are not just passive - they can store or release blood depending on the body's needs. Lung blood volume can range from half-normal to twice-normal in different conditions.
Examples:
- Blowing hard (e.g., playing a trumpet) → builds up high pressure in lungs → pushes ~250 mL of blood OUT of pulmonary vessels into systemic circulation
- Hemorrhage (blood loss) → lungs automatically shift blood into systemic vessels to help compensate
This makes the lungs act like a built-in blood bank for the body.
What Happens in Heart Disease?
When the left heart fails (or mitral valve is diseased - stenosis or regurgitation):
- Blood cannot drain properly from the lungs into the left heart
- Blood dams up in the pulmonary circulation
- Pulmonary blood volume can increase by up to 100%
- This raises pulmonary vascular pressure → leads to pulmonary edema
Key ratio to remember:
Systemic circulation volume is 9x larger than pulmonary volume. So a small shift of blood into the lungs causes a big rise in pulmonary pressure, but only a mild drop in systemic pressure.
One-Line Summary
The lungs hold ~450 mL of blood (9% of total), act as a flexible reservoir that can shift blood in or out as needed - but when the left heart fails, blood backs up into the lungs and causes dangerous pressure rises.
Source: Guyton and Hall Textbook of Medical Physiology, Chapter 39
Blood flow through the lungs and its distribution summarry easy
Reading File
Reading File
Loading Image
Loading Image
Blood Flow Through the Lungs and Its Distribution
(Guyton & Hall - Medical Physiology, Chapter 39)
Basic Rule
Pulmonary blood flow = Cardiac output
Whatever the heart pumps out goes entirely through the lungs. The pulmonary vessels behave like distensible tubes - they widen when pressure rises and narrow when pressure falls.
How Blood is Distributed to the Right Areas
The lung has a smart self-regulating system. Blood must go to alveoli that are well-ventilated (have good O₂) - not to areas where ventilation is poor. Here is how it works:
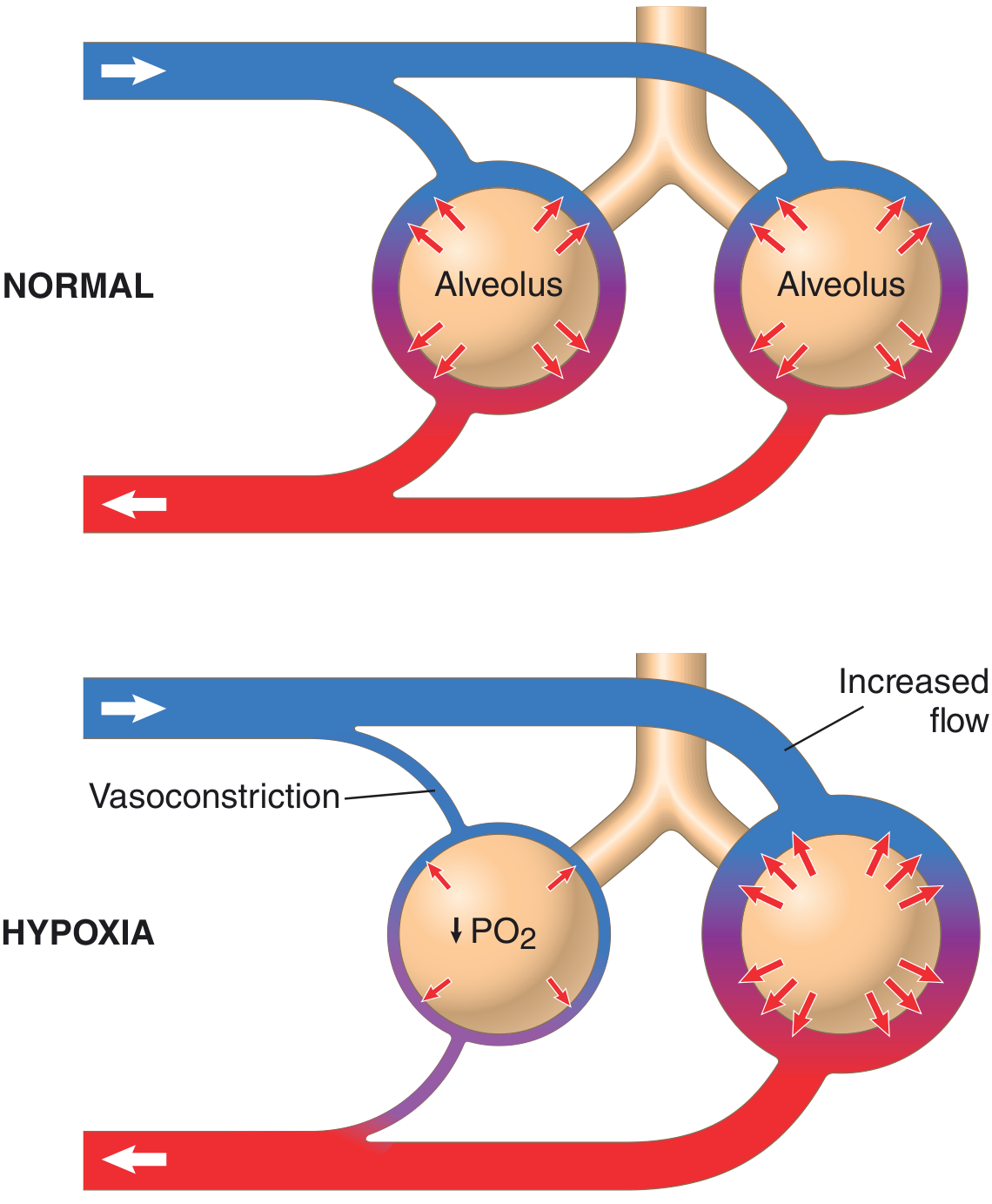
Hypoxic Pulmonary Vasoconstriction
When O₂ in an alveolus drops below 70% of normal (PO₂ < 73 mmHg), the blood vessels next to that alveolus constrict. This is the opposite of what systemic vessels do (they dilate in low O₂).
Mechanism (3 steps):
- Low O₂ → inhibits K⁺ channels in pulmonary smooth muscle → cell membrane depolarizes → Ca²⁺ channels open → Ca²⁺ floods in → vasoconstriction
- Low O₂ → triggers release of vasoconstrictors (endothelin, reactive oxygen species)
- Low O₂ → reduces nitric oxide (a vasodilator) from lung tissue
Result: Blood is diverted away from poorly ventilated alveoli toward well-ventilated ones. This is called V/Q matching - automatic and brilliant.
Effect of Gravity - The 3 Zones of Pulmonary Blood Flow
In an upright person, blood flow is NOT equal throughout the lung. Gravity creates a pressure difference from top to bottom. Blood flow at the base (bottom) is about 5x greater than at the apex (top) when standing at rest.
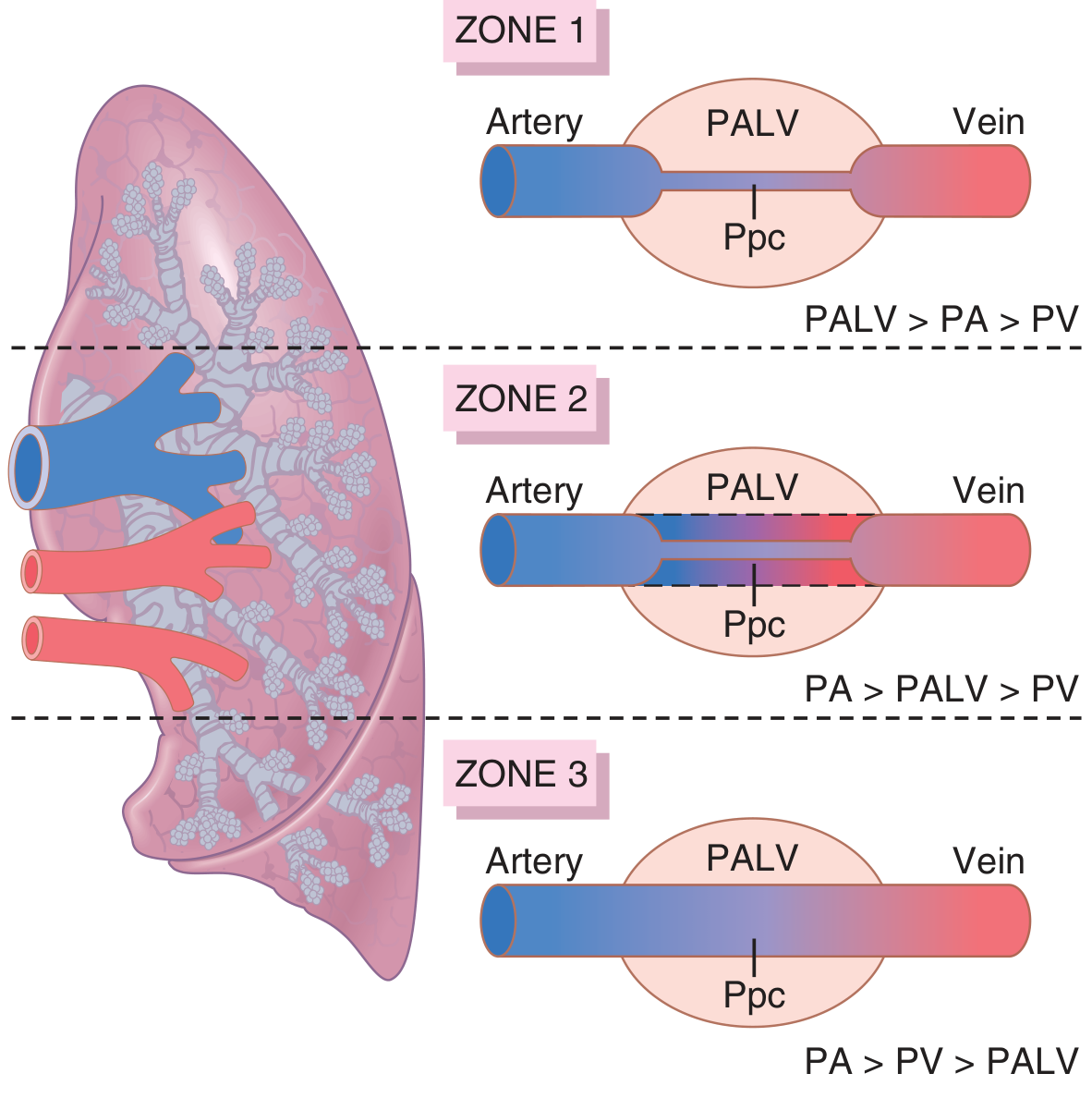
This is explained by the West Zones (Zones 1, 2, 3):
| Zone | Location | Condition | Blood Flow |
|---|---|---|---|
| Zone 1 | Apex (top) | Alveolar pressure > arterial pressure | No flow (capillaries collapsed) |
| Zone 2 | Middle | Arterial pressure > alveolar > venous pressure | Intermittent flow (only during systole) |
| Zone 3 | Base (bottom) | Arterial pressure > venous > alveolar pressure | Continuous flow (all the time) |
Key: Capillaries are squeezed from outside by alveolar air pressure. If alveolar pressure wins over blood pressure, the capillary collapses and blood stops.
Normally (at rest, standing): only Zone 2 and Zone 3 exist
- Zone 2 = apex (intermittent flow)
- Zone 3 = all lower areas (continuous flow)
- Zone 1 = does NOT normally exist (would require dangerously low blood pressure or artificial ventilation with very high airway pressure)
What Happens During Exercise?
During exercise, cardiac output rises and pulmonary artery pressure increases. This extra pressure recruits previously closed capillaries at the apex → Zone 2 expands upward → blood flow becomes much more uniform throughout the entire lung.
Simple Summary
| Concept | What Happens |
|---|---|
| Total flow | = Cardiac output |
| Low O₂ in alveolus | Vessels constrict → blood diverted away |
| High O₂ in alveolus | Vessels open → blood flows there |
| Bottom of lung | Most blood flow (gravity helps) |
| Top of lung | Least blood flow (gravity works against it) |
| Exercise | Flow becomes more even top to bottom |
One-Line Takeaway
The lungs send blood where O₂ is good (hypoxic vasoconstriction) and gravity pulls most blood to the base - creating three flow zones from top to bottom.
Source: Guyton and Hall Textbook of Medical Physiology, Chapter 39
This is a shared conversation. Sign in to Orris to start your own chat.