What is asthma
Reading File
Searching the Web
asthma definition pathophysiology overview 2025
Finding Sources
Searching PubMed
"asthma"[MeSH Terms] AND "pathophysiology"
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Now I have rich textbook content. Let me compile the comprehensive answer.
Asthma
Definition
Asthma is a chronic inflammatory disorder of the airways characterized by three core elements:
- Reversible airway obstruction - narrowing of airways that can reverse spontaneously or with treatment
- Airway inflammation - involving many different cell types
- Bronchial hyperresponsiveness - an exaggerated reaction to a wide variety of stimuli
"Asthma is a chronic inflammatory disorder of the airways in which many different cells play a role. In patients with asthma, this inflammation causes breathlessness, chest tightness, recurrent episodes of wheezing, and cough, particularly at night."
- Textbook of Family Medicine, 9th ed.
An important clinical reminder: not all wheezing is asthma, and not all asthma has wheezing.
Pathophysiology
The mechanism involves a cascade of events:
| Step | What Happens |
|---|---|
| Trigger exposure | Allergens, irritants, exercise, infections stimulate the immune system |
| Airway inflammation | Mast cells, eosinophils, T lymphocytes, and macrophages release inflammatory mediators |
| Bronchoconstriction | Smooth muscle contraction narrows the airway lumen |
| Mucosal edema | Airway wall swelling further reduces airway diameter |
| Mucus hypersecretion | Excessive secretions block smaller airways |
| Air trapping | Obstruction is worst during expiration, leading to hyperinflation |
Chronic asthma can also cause structural airway remodeling - subepithelial fibrosis, angiogenesis, and extracellular matrix deposition. This can make some obstruction less reversible over time.
- Murray & Nadel's Textbook of Respiratory Medicine
Common Triggers
- Environmental allergens: pollen, mold, house dust mites, cockroach excreta, animal dander
- Respiratory infections (especially viral)
- Exercise
- Tobacco smoke, strong odors, air pollutants
- Cold air / climate changes
- Certain medications (aspirin, NSAIDs, beta-blockers)
- Gastroesophageal reflux (GERD)
- Emotional stress
Symptoms
- Wheezing (high-pitched whistling sound during breathing)
- Dyspnea (shortness of breath)
- Chest tightness
- Cough - often worse at night or early morning
Symptoms are characteristically variable and episodic.
Diagnosis
Diagnosis has three stages:
- Suggestive symptoms with precipitating factors
- Confirmation with testing (spirometry is the gold standard - looks for reduced FEV1/FVC ratio with reversibility after bronchodilator)
- Symptomatic improvement with appropriate asthma therapy
Peak expiratory flow rate (PEFR) can be used for monitoring at home.
Differential Diagnosis to Consider
| In Children | In Adults |
|---|---|
| Viral bronchiolitis | COPD |
| GERD | Congestive heart failure |
| Cystic fibrosis | Pulmonary embolism |
| Foreign body | ACE inhibitor-induced cough |
| Paradoxical vocal cord motion | Paradoxical vocal cord motion |
Treatment (Stepwise Approach)
Treatment follows a step-up/step-down approach based on severity:
- Reliever (rescue): Short-acting beta-2 agonists (SABAs) like salbutamol - for acute symptoms. Should be needed less than twice per week; if more frequent, step up therapy.
- Controller (maintenance): Inhaled corticosteroids (ICS) are the preferred therapy for all persistent asthma - they address the underlying inflammation.
- Add-on therapies: Long-acting beta-2 agonists (LABAs), leukotriene receptor antagonists (LTRAs), or biologics for severe/uncontrolled disease.
- Acute exacerbations: Oral corticosteroids + nebulized SABAs + ipratropium (in the emergency setting).
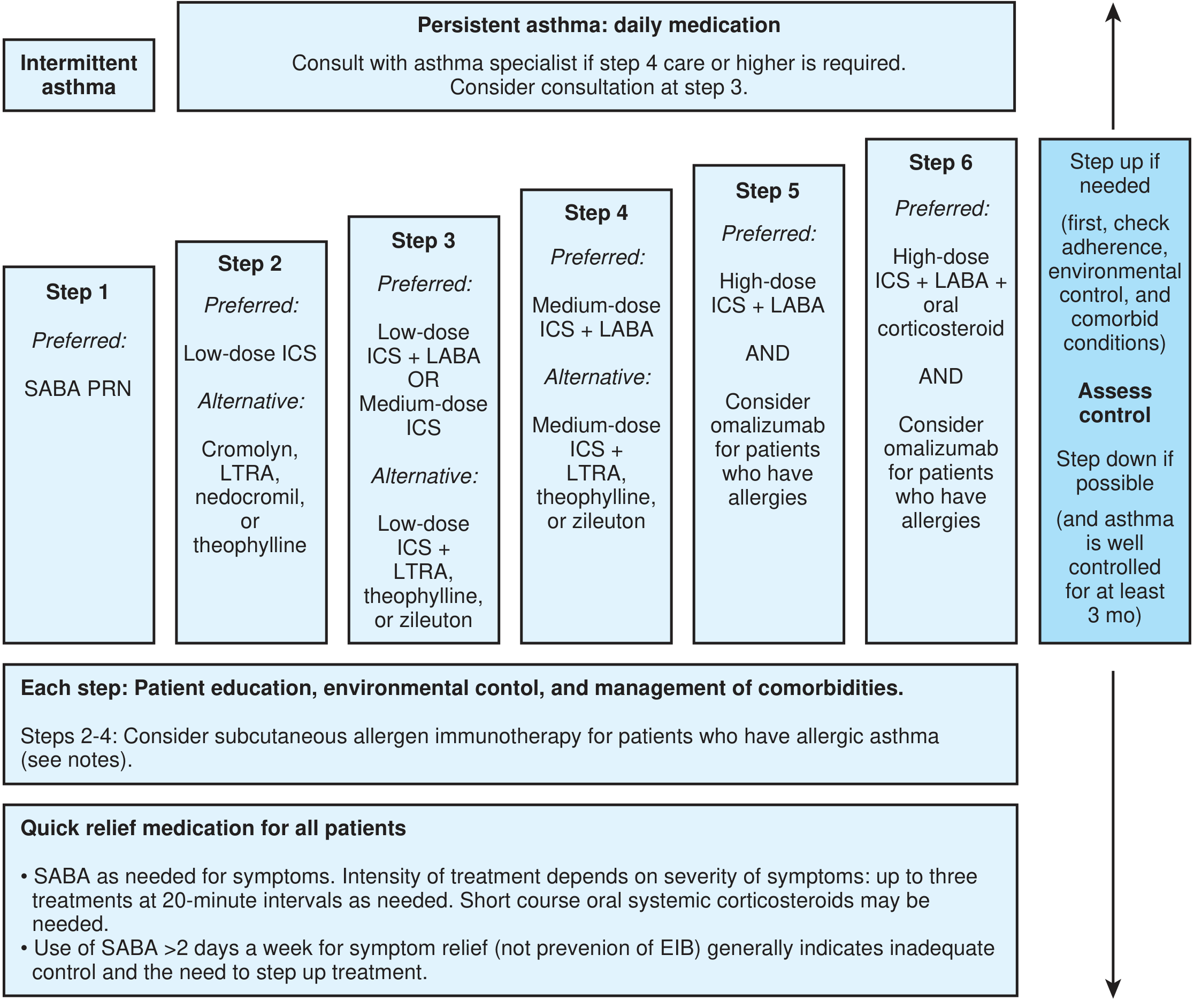
Step therapy for adults with asthma. ICS = inhaled corticosteroid; LABA = long-acting beta-agonist; LTRA = leukotriene receptor antagonist; SABA = short-acting beta-agonist.
Epidemiology
- Asthma affects approximately 26.8 million people in the United States
- It is the most common chronic disease of childhood, affecting ~4.5 million children in the US
- Prevalence increased from 1980 to 2010, but mortality and hospitalization rates have been declining since the late 1990s
- Affects over 5.4 million people in the UK
Key Takeaways
- Asthma = chronic airway inflammation + reversible obstruction + hyperresponsiveness
- Most cases are triggered by allergens or irritants; often co-exists with allergic rhinitis
- Spirometry is the diagnostic gold standard
- Inhaled corticosteroids are the cornerstone of maintenance treatment
- Good asthma control is achievable with proper identification of triggers and stepwise pharmacotherapy
Sources: Textbook of Family Medicine, 9th ed.; Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.