Sickle cell crises saq
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, well-sourced information to write a thorough SAQ answer on sickle cell crises. Here is the complete answer:
Sickle Cell Crises - Short Answer Question (SAQ)
1. Background: Pathophysiology of Sickle Cell Disease
Genetic basis: Sickle cell disease (SCD) results from a point mutation - substitution of glutamic acid by valine at the 6th position of the beta-globin chain, producing HbS instead of HbA. This autosomal recessive condition is most severe in homozygotes (HbSS).
Mechanism of sickling: Under deoxygenated conditions (low O2 saturation), HbS polymerizes and aggregates inside erythrocytes, distorting them into a rigid sickle shape. In homozygotes, sickling can occur at oxygen saturations as high as 85% (vs. ~40% in trait carriers).
Downstream injury (Barash Clinical Anesthesia, Table 24-22):
- RBC and platelet adhesion to endothelium
- Activation of coagulation and thrombosis
- Ischemia-reperfusion injury
- Intravascular hemolysis releasing free Hb, which scavenges NO (nitric oxide) - causing endothelial dysfunction and vasoconstriction
- Leukocyte activation and free radical injury
- TLR4-mediated inflammatory amplification by free heme
Peripheral blood film showing sickle cells:
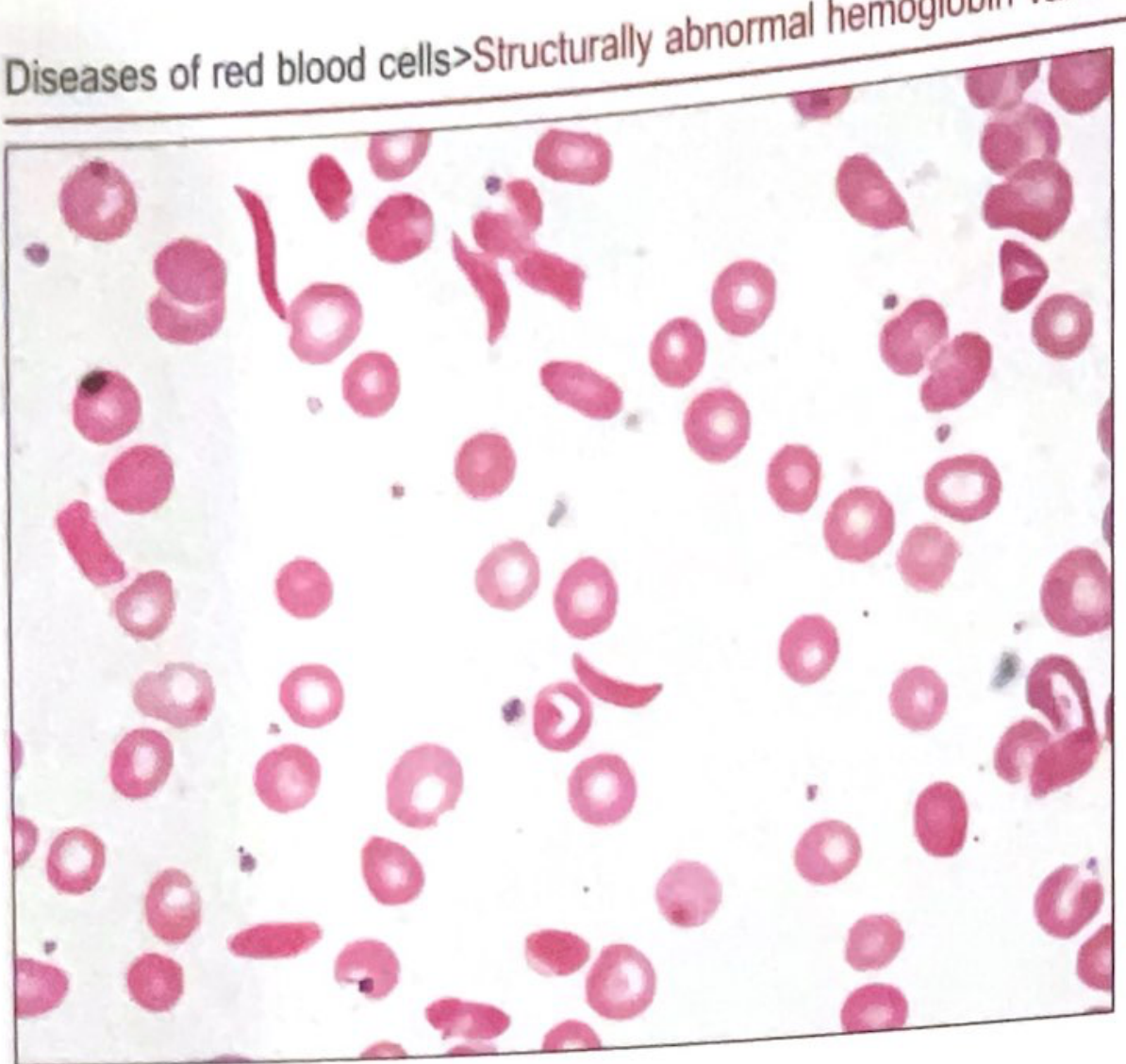
(Quick Compendium of Clinical Pathology, 5e)
2. Types of Sickle Cell Crises
A. Vaso-occlusive Crisis (VOC) - Pain Crisis
Most common type. The first and most frequent manifestation of SCD.
Precipitants:
- Cold exposure
- Dehydration
- Infection
- Alcohol
- Hypoxia (altitude, unpressurised flight)
- Acidosis
Mechanism: Sickled cells obstruct the microcirculation, causing musculoskeletal ischemia. Vaso-occlusion involves not just HbS polymerization but also activated vascular endothelium, altered NO metabolism, hypercoagulability, and ischemia-reperfusion injury.
Features: Severe pain in bones, joints, abdomen, back. Dactylitis (hand-foot syndrome) in infants.
Management:
- Mild: oral analgesics, rest, hydration
- Severe: IV opioids (morphine or hydromorphone), IV fluids, supplemental O2, RBC transfusion in refractory cases, consider regional analgesia
Long-term complications:
- Autosplenectomy (recurrent splenic infarction)
- Avascular necrosis (hip most common, then shoulder)
- Papillary necrosis + renal complications
- Stroke/TIA (up to 30% of HbSS patients)
- Liver infarction
- Pulmonary hypertension (in ~10-30% of adults)
B. Acute Chest Syndrome (ACS)
Most common cause of death in SCD. Second most common reason for hospitalization.
Definition: New pulmonary opacity involving at least one complete lung segment, with at least one of: chest pain, fever, tachypnea, wheezing, cough - in a patient with SCD.
Causes: Fat embolism (from infarcted bone marrow), pulmonary infection, thromboembolism, hypoventilation from rib/sternum infarct.
Features:
- Chest pain, dyspnea, cough, wheezing
- Fever, tachypnea
- Hypoxemia
- New pulmonary infiltrates on chest X-ray
- Leukocytosis
Mortality: 1-20%.
Management:
- Supplemental O2
- IV hydration
- Analgesia
- Incentive spirometry / respiratory support
- Empirical antibiotics (pending sputum cultures)
- RBC transfusion (simple or exchange) for severe/refractory cases
- Note: Postoperative ACS incidence = 10-20% after abdominal surgery. Preoperative transfusion and postoperative spirometry reduce risk.
C. Aplastic Crisis
Cause: Transient arrest of erythropoiesis, almost always due to Parvovirus B19 infection (can also be folic acid deficiency).
Features:
- Acute fall in Hb below baseline
- Low or absent reticulocyte count (key differentiator)
- Viral prodrome often present
- Can precipitate heart failure in severe anemia
Management:
- Simple RBC transfusion if severe anemia
- Isolation (parvovirus is infectious)
- IV fluids
- Do not transfuse for asymptomatic anemia unless reticulocyte count is low
Indications for emergency transfusion (Quick Compendium of Clinical Pathology, 5e): stroke, retinal artery occlusion, splenic sequestration crisis, ACS, aplastic crisis.
D. Splenic Sequestration Crisis
Epidemiology: Occurs primarily in infants and young children (before autosplenectomy is complete). Rare in adults.
Mechanism: Sudden pooling of blood in the spleen due to partial or complete occlusion of venous drainage, causing rapid expansion of the spleen.
Features:
- Acutely enlarged spleen
- Hb 2+ g/dL below baseline
- Life-threatening hypotension and hypovolemic shock
- Often triggered by viral illness
Management:
- IV fluid resuscitation
- Type and screen
- Admit for serial abdominal exams
- RBC transfusion in 5-10 mL/kg aliquots - caution: autotransfusion from spleen on recovery can cause rebound rise in Hb and hyperviscosity
- Recurrent severe cases: splenectomy
E. Hyperhemolytic Crisis
Features: Sudden, severe exacerbation of anemia with increased hemolysis.
- May be caused by concomitant G6PD deficiency
- Elevated bilirubin, elevated LDH, hemoglobinuria
3. Summary Table of Crises
| Crisis | Key Feature | Reticulocytes | Cause | Emergency Tx |
|---|---|---|---|---|
| Vaso-occlusive | Severe bone/tissue pain | Normal/raised | Microvascular occlusion | Analgesia, fluids, O2 |
| Acute chest syndrome | Pulmonary infiltrate + hypoxia | Normal | Fat embolism, infection | O2, antibiotics, exchange transfusion |
| Aplastic | Sudden severe anemia | Low/absent | Parvovirus B19 | Simple transfusion, isolation |
| Sequestration | Splenomegaly + shock | Raised | Venous splenic occlusion | Fluids, careful transfusion |
| Hyperhemolytic | Worsening anemia + jaundice | Raised | G6PD deficiency | Supportive |
4. Long-term / Chronic Complications of SCD
- Stroke (up to 30% of HbSS)
- Pulmonary hypertension (10-30% of adults)
- Proliferative retinopathy
- Renal disease - isosthenuria, gross hematuria, papillary necrosis, nephrotic syndrome, renal medullary carcinoma
- Avascular necrosis of femoral/humeral head
- Priapism (sustained painful erection >4 hr - treat with analgesia, hydration, O2, urology referral for aspiration)
- Autosplenectomy - functional asplenia increasing risk of encapsulated organism sepsis
5. Management Principles
Acute
- IV fluids (avoid dehydration)
- Supplemental oxygen
- Strong analgesia (IV morphine/hydromorphone for severe VOC)
- Antibiotics if infection suspected
Preventive / Chronic
| Intervention | Purpose |
|---|---|
| Hydroxyurea (hydroxycarbamide) | Induces HbF (target >20%), reduces frequency of painful crises and ACS, reduces transfusion requirements. Monitor for myelosuppression. Teratogenic - contraception required. |
| Penicillin V prophylaxis | Reduces pneumococcal sepsis risk (from age 3 months, when HbF wanes) |
| Vaccinations | Pneumococcal (PCV13 <2 yrs; PPV23 ≥2 yrs), meningococcal, Hib, influenza (annual) |
| Folic acid | Replaces folate consumed by chronic hemolysis |
| Chronic transfusion | Children with abnormal transcranial Doppler (TCD) velocities for stroke prevention; target HbS <30% in children, <50% in adults |
| Stem cell transplant | Only curative therapy; requires matched sibling donor |
6. Key SAQ Points
- Mutation: Glu → Val at 6th position of beta-globin chain (HbS)
- Most common crisis: Vaso-occlusive (pain crisis)
- Most common cause of death: Acute chest syndrome
- Aplastic crisis cause: Parvovirus B19 - distinguished by absent reticulocytes
- Sequestration crisis: Infants/young children; life-threatening; avoid over-transfusion
- Hydroxyurea mechanism: Increases HbF, which prevents intracellular sickling
- Autosplenectomy makes patients vulnerable to encapsulated bacteria (S. pneumoniae, H. influenzae, N. meningitidis)
- Altitude/hypoxia can precipitate VOC even in pressurised aircraft
Sources: Emery's Elements of Medical Genetics and Genomics; Quick Compendium of Clinical Pathology, 5e; Barash Clinical Anesthesia, 9e; Morgan & Mikhail's Clinical Anesthesiology, 7e; Murray & Nadel's Respiratory Medicine; Harriet Lane Handbook, 23e; Swanson's Family Medicine Review
This is a shared conversation. Sign in to Orris to start your own chat.