Notes on all cardiac murmurs , causes mechanisms with their audio characteristics, radiation, and effects of standing, squatting, handgrip, and Valsalva,
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed. Let me compile the comprehensive notes.
Cardiac Murmurs - Complete Notes
(Sources: Harrison's Principles of Internal Medicine 22E, 2025; Fuster & Hurst's The Heart, 15th Ed; Goldman-Cecil Medicine)
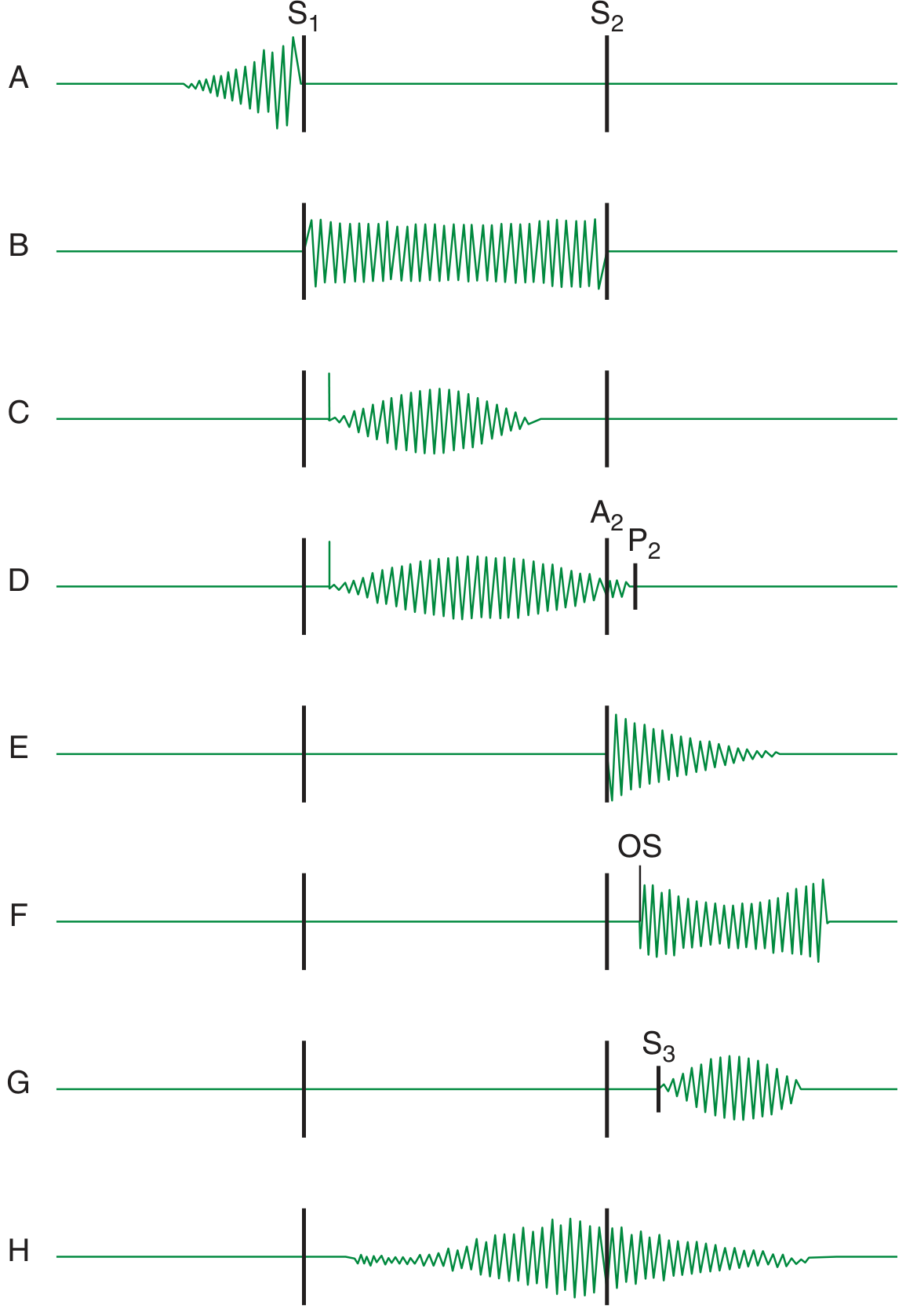
Murmur Diagram
Grading of Murmurs
| Grade | Description |
|---|---|
| I | Faint; heard only after a few seconds |
| II | Moderately loud; heard immediately |
| III | Loud; no thrill |
| IV | Loud; associated with thrill |
| V | Very loud; heard with stethoscope edge only |
| VI | Loudest; audible with stethoscope just off chest |
Mechanisms of Murmur Production
Murmurs arise from three mechanisms (Harrison's 22E, p. 327):
- Increased turbulence from accelerated blood flow through normal or abnormal orifices
- Flow through a narrowed or irregular orifice into a dilated vessel/chamber
- Backward flow through an incompetent valve, VSD, or PDA
The frequency (pitch), configuration, and intensity depend on the magnitude and variability of the pressure gradient, geometry, and compliance of the involved chambers.
Dynamic Maneuvers - Master Table
Understanding the physiology is key:
- Decreased preload (Valsalva strain phase, standing) → smaller LV cavity → narrows LVOT → reduces most murmurs; increases HOCM and MVP click moves earlier
- Increased preload (squatting, leg raise, release of Valsalva) → larger LV → widens LVOT → reduces HOCM; delays MVP click
- Increased afterload / SVR (handgrip, squatting) → increases regurgitant murmurs (MR, AR, VSD); decreases ejection murmurs (AS)
- Decreased afterload (amyl nitrite, standing) → decreases regurgitant murmurs; increases ejection murmurs
| Maneuver | Preload | Afterload | Heart Rate |
|---|---|---|---|
| Valsalva (strain) | ↓↓ | ↓ | ↑ |
| Standing (from squat) | ↓ | ↓ | ↑ |
| Squatting | ↑ | ↑ | ↓ |
| Handgrip (isometric) | slight ↑ | ↑↑ | ↑ |
SYSTOLIC MURMURS
1. Aortic Stenosis (AS)
Cause: Calcific degeneration (commonest in adults >65), bicuspid aortic valve, rheumatic disease
Mechanism: Systolic ejection obstruction at the aortic valve. During systole, blood is forced through a narrowed orifice, creating turbulence that peaks at mid-systole when transvalvular flow rate is maximum.
Audio characteristics:
- Harsh, rough, crescendo-decrescendo (diamond-shaped) ejection murmur
- High-to-medium pitched
- Best heard: right 2nd intercostal space (RUSB), with patient leaning forward
- Begins after S1 (after opening of AV), ends before A2
- Often preceded by an aortic ejection click (in pliable, non-calcified valve - bicuspid)
- S1 normal; A2 may be soft or absent in severe AS
- S4 gallop common
- Gallavardin effect: murmur sounds high-pitched and musical ("cooing/squeaking") at the apex, distinct from a separate MR murmur
Radiation: To right clavicle, right carotid artery, and neck (absence of radiation to right clavicle has a negative LR of 0.1 for AS - Miller's Anesthesia)
Associated findings: Pulsus parvus et tardus (slow-rising, low-amplitude carotid pulse), S4, paradoxical splitting of S2
| Maneuver | Effect on Murmur | Reason |
|---|---|---|
| Valsalva (strain) | Decreases | ↓ venous return → ↓ stroke volume → ↓ transvalvular flow |
| Standing | Decreases | ↓ preload |
| Squatting | Increases | ↑ preload + ↑ afterload → ↑ stroke volume |
| Handgrip | Decreases | ↑ afterload → ↓ stroke volume |
2. Hypertrophic Obstructive Cardiomyopathy (HOCM)
Cause: Asymmetric septal hypertrophy causing dynamic LVOT obstruction; systolic anterior motion (SAM) of the mitral valve
Mechanism: Dynamic obstruction worsens when the LV cavity is small (less filling). The venturi effect and SAM create a gradient that is load- and volume-dependent. Coexistent MR from SAM adds to the murmur.
Audio characteristics:
- Harsh, crescendo-decrescendo systolic ejection murmur
- Best heard: left lower sternal border and apex, NOT the base
- Does NOT radiate to carotid arteries (distinguishes from valvular AS)
- May radiate to base of heart and apex but NOT to carotid
- Accompanied by features of MR when SAM is present
Radiation: Lower sternal border to apex; rarely to carotids (this distinction is key)
| Maneuver | Effect on Murmur | Reason |
|---|---|---|
| Valsalva (strain) | Increases (hallmark) | ↓ preload → smaller LV cavity → worsens obstruction |
| Standing | Increases | ↓ preload → smaller LV |
| Squatting | Decreases | ↑ preload → larger LV → relieves obstruction |
| Handgrip | Decreases | ↑ afterload → larger LV, better filling |
Memory: HOCM is the OPPOSITE of AS for Valsalva and standing.
3. Mitral Regurgitation (MR)
Cause: Mitral valve prolapse (MVP), rheumatic disease, ischemic papillary muscle dysfunction, dilated cardiomyopathy, endocarditis, flail leaflet
Mechanism: Systolic backflow from LV into LA across an incompetent mitral valve. The LV-LA pressure gradient persists throughout systole since LV pressure always exceeds LA pressure from S1 to S2.
Audio characteristics:
- Holosystolic (pansystolic) plateau murmur - begins with S1, ends with or after A2
- High-pitched, blowing quality
- Best heard: apex (mitral area)
- S1 often soft (due to incomplete valve closure)
- S3 gallop may be present (high flow across MV in diastole)
Radiation:
- Posteriorly directed jet (anterior leaflet prolapse/flail): radiates to left axilla and left infrascapular area (classic)
- Anteriorly directed jet (posterior leaflet prolapse/flail): radiates to base/aortic area (RUSB, may mimic AS)
- Ischemic MR may radiate to the spine
| Maneuver | Effect on Murmur | Reason |
|---|---|---|
| Valsalva (strain) | Decreases | ↓ preload → ↓ regurgitant volume |
| Standing | Decreases | ↓ preload |
| Squatting | Increases | ↑ preload + ↑ afterload → ↑ regurgitant volume |
| Handgrip | Increases | ↑ afterload (SVR) → ↑ LV-LA gradient → ↑ regurgitation |
4. Mitral Valve Prolapse (MVP)
Cause: Myxomatous degeneration of mitral valve leaflets; most common in young women
Mechanism: Mid-systolic buckling of the elongated mitral leaflet(s) into the LA, producing a click, followed by regurgitation of varying degrees (late systolic murmur). The click timing is determined by LV volume - smaller LV = click moves earlier.
Audio characteristics:
- Non-ejection mid-systolic click followed by a late systolic murmur
- Click is high-pitched, sharp
- Murmur is high-pitched, blowing, late systolic (crescendo toward S2)
- Best heard: apex and left lower sternal border
Radiation: To axilla (if MR component is significant)
| Maneuver | Effect | Reason |
|---|---|---|
| Valsalva (strain) | Click moves earlier; murmur lengthens | ↓ LV volume → leaflet prolapses sooner |
| Standing | Click moves earlier; murmur lengthens | ↓ LV volume |
| Squatting | Click moves later; murmur shortens | ↑ LV volume → delays prolapse |
| Handgrip | Click moves later; murmur shortens | ↑ LV volume |
Memory: Smaller LV = click earlier, longer murmur. Bigger LV = click later, shorter murmur.
5. Tricuspid Regurgitation (TR)
Cause: Functional (RV dilation from pulmonary hypertension), rheumatic, endocarditis (IVDU), carcinoid, Ebstein anomaly
Mechanism: Systolic backflow from RV to RA. Similar to MR but right-sided.
Audio characteristics:
- Holosystolic, high-pitched, blowing
- Best heard: left lower sternal border (LLSB) / xiphoid area
- Carvallo's sign: murmur increases with inspiration (Rivero-Carvallo sign) - inspiration increases RV filling → ↑ RV-RA gradient
- S3 of right origin may be present
Radiation: May radiate to right sternal border; typically localized
| Maneuver | Effect | Reason |
|---|---|---|
| Valsalva (strain) | Decreases | ↓ RV preload |
| Standing | Decreases | ↓ preload |
| Squatting | Increases | ↑ preload |
| Handgrip | Increases | ↑ afterload |
| Inspiration | Increases (key feature) | ↑ venous return to right heart |
6. Ventricular Septal Defect (VSD)
Cause: Congenital (membranous or muscular); post-infarction (acute ischemic VSD)
Mechanism: Left-to-right shunt from LV to RV through a septal defect during systole. The high-pressure gradient (LV vs RV) is maintained throughout systole, producing a holosystolic murmur.
Audio characteristics:
- Holosystolic, harsh, loud (often grade IV-V with thrill)
- High-pitched
- Best heard: left lower sternal border (LLSB), 3rd-4th interspace
- Thrill is common at LLSB
- Small VSDs ("maladie de Roger") may produce the loudest murmurs
Radiation: Across the precordium; right sternal border
| Maneuver | Effect | Reason |
|---|---|---|
| Valsalva (strain) | Decreases | ↓ preload → ↓ L-R gradient |
| Standing | Decreases | ↓ preload |
| Squatting | Increases | ↑ SVR → ↑ L-R gradient |
| Handgrip | Increases | ↑ SVR → ↑ LV-RV pressure difference |
7. Pulmonary Stenosis (PS)
Cause: Congenital (most common), rheumatic (rare), carcinoid syndrome
Mechanism: Obstruction to RV outflow at the pulmonary valve. Flow turbulence peaks mid-systole. The murmur extends longer than AS because RV takes longer to overcome obstruction - the murmur can extend through or beyond A2 (into P2 territory).
Audio characteristics:
- Crescendo-decrescendo ejection murmur
- Best heard: left 2nd intercostal space (LUSB)
- Preceded by pulmonary ejection click (disappears/decreases on inspiration - unique to PS; all other right-sided sounds increase on inspiration)
- Murmur increases with inspiration
- In severe PS: murmur peaks late in systole, P2 is soft or absent, wide splitting of S2
Radiation: To left shoulder and upper left chest
| Maneuver | Effect | Reason |
|---|---|---|
| Valsalva (strain) | Decreases | ↓ RV filling |
| Standing | Decreases | ↓ preload |
| Squatting | Increases | ↑ preload |
| Inspiration | Increases | ↑ RV filling |
DIASTOLIC MURMURS
8. Aortic Regurgitation (AR) - Chronic
Cause: Bicuspid AV, rheumatic disease, aortic root dilation (Marfan, HTN, dissection), endocarditis, ankylosing spondylitis
Mechanism: Diastolic backflow from aorta into LV across an incompetent aortic valve. Pressure gradient exists throughout diastole (highest early, declining progressively as LV fills and aortic pressure falls) → decrescendo murmur.
Audio characteristics:
- Early diastolic, decrescendo (starts immediately after A2)
- High-pitched, blowing quality ("cooing" or "blowing")
- Best heard: left sternal border (3rd ICS), patient leaning forward, breath held in expiration
- Austin Flint murmur: a low-pitched mid-diastolic rumble at the apex (functional MS from AR jet hitting anterior mitral leaflet)
- Peripheral signs: wide pulse pressure, water-hammer (Corrigan's) pulse, Quincke's pulsations, De Musset's sign, Traube's sign, Duroziez's sign
Radiation: Along left sternal border; to apex
Acute severe AR (distinctive features):
- Murmur is SHORT, LOW-PITCHED, and early diastolic (LV pressure rises quickly → gradient disappears early)
- Peripheral signs of high pulse pressure are absent
- Premature mitral valve closure → soft S1
- Tachycardia common
| Maneuver | Effect | Reason |
|---|---|---|
| Valsalva (strain) | Decreases | ↓ aortic pressure → ↓ gradient |
| Standing | Decreases | ↓ preload + ↓ diastolic BP |
| Squatting | Increases | ↑ DBP/SVR → ↑ aortic-LV gradient |
| Handgrip | Increases | ↑ SVR → ↑ diastolic aortic pressure → ↑ regurgitation |
| Lean forward + expiration | Enhances auscultation | Best position to hear it |
9. Pulmonary Regurgitation (PR) - Graham Steell Murmur
Cause: Most commonly pulmonary hypertension causing annular dilation; also endocarditis, post-surgical (repaired TOF), congenital
Mechanism: Diastolic backflow from pulmonary artery into RV. The PA-RV pressure gradient during diastole drives backflow.
Audio characteristics:
- Early diastolic, decrescendo - begins immediately after P2
- High-pitched, blowing ("Graham Steell murmur" when due to pulmonary hypertension)
- Best heard: left 2nd-3rd ICS (LUSB), radiates along left sternal border
- Increases with inspiration (more RV filling)
- Without pulmonary hypertension: softer, lower pitched, harder to appreciate
- Must distinguish from AR: both are decrescendo early diastolic at left sternal border - key feature is P2 vs A2 timing, and signs of pulmonary hypertension (RV heave, loud P2)
Radiation: Along left sternal border
| Maneuver | Effect | Reason |
|---|---|---|
| Inspiration | Increases | ↑ RV filling |
| Valsalva | Decreases | ↓ RV preload |
| Squatting | Increases | ↑ preload |
10. Mitral Stenosis (MS)
Cause: Almost exclusively rheumatic heart disease; rarely congenital, systemic lupus, carcinoid, mucopolysaccharidoses
Mechanism: Obstruction at the mitral valve produces a persistent left atrial (LA) to LV pressure gradient during diastole. Flow across the valve generates a low-frequency rumble. Maximum flow occurs in early diastole (rapid ventricular filling) and at end-diastole (atrial contraction = presystolic accentuation, absent in AF).
Audio characteristics:
- Low-pitched diastolic rumble ("rolling thunder")
- Best heard: apex, with bell of stethoscope (low frequency), patient in left lateral decubitus position
- Opening snap (OS): high-pitched, immediately after S2 (P2); interval P2-OS inversely proportional to severity (shorter OS = more severe)
- Rumble starts after OS; in sinus rhythm, presystolic accentuation just before S1
- S1 loud (if valve pliable; soft if calcified)
- S2: loud P2 if pulmonary hypertension develops
- Duration of rumble parallels severity
Radiation: Does not radiate; localized to apex
| Maneuver | Effect | Reason |
|---|---|---|
| Exercise / tachycardia | Increases (heard better, symptoms worsen) | ↑ trans-mitral gradient |
| Left lateral position | Enhances auscultation | Brings mitral valve closer to chest wall |
| Valsalva | Decreases | ↓ LA-LV gradient |
| Squatting | Increases | ↑ venous return → ↑ trans-mitral flow |
| Inspiration (right-sided) | - | Not a right-sided murmur |
11. Tricuspid Stenosis (TS)
Cause: Almost exclusively rheumatic (almost always with MS); carcinoid; rarely congenital
Mechanism: RA-RV diastolic gradient (analogous to MS but right-sided). Gradient is much lower than MS.
Audio characteristics:
- Low-pitched diastolic rumble
- Best heard: lower left sternal border (4th ICS) or xiphoid area
- Increases with inspiration (Carvallo's sign on diastolic side)
- Opening snap may be present (earlier than MS opening snap)
- Presystolic accentuation in sinus rhythm
Radiation: Minimal
| Maneuver | Effect | Reason |
|---|---|---|
| Inspiration | Increases | ↑ RA-RV gradient with ↑ venous return |
| Valsalva | Decreases | ↓ right heart filling |
CONTINUOUS MURMURS
12. Patent Ductus Arteriosus (PDA)
Cause: Failure of ductus arteriosus to close; associated with prematurity, rubella infection, high altitude
Mechanism: Persistent left-to-right shunt from aorta to pulmonary artery, present both in systole and diastole (because aortic pressure exceeds PA pressure throughout the cardiac cycle).
Audio characteristics:
- Continuous "machinery" murmur - peaks at S2 then continues into diastole
- Harsh, rumbling, with a "humming" or "machinery" quality
- Best heard: left infraclavicular area (2nd ICS, below left clavicle)
- Peaks around S2 (loudest at S2, then diminishes in diastole)
- Wide pulse pressure, bounding pulses
Radiation: To left shoulder, neck
| Maneuver | Effect | Reason |
|---|---|---|
| Squatting | Increases | ↑ SVR → ↑ aortic-PA gradient |
| Valsalva | Decreases diastolic component | ↓ venous return |
13. Venous Hum
Cause: Turbulent jugular venous flow; physiological (normal children, pregnant women, high-output states)
Mechanism: Turbulent blood flow in the internal jugular vein, continuous since venous flow occurs throughout the cycle.
Audio characteristics:
- Soft, low-pitched continuous hum
- Best heard: right supraclavicular space, with patient sitting up
- Abolished by: turning head to ipsilateral side, light jugular vein compression, lying down
- Distinguished from PDA by location (neck vs subclavicular) and abolition with position/compression
14. Mammary Souffle
Cause: Hyperdynamic flow in mammary arteries during pregnancy and lactation
Mechanism: Arterial turbulence in mammary vasculature from high-output state.
Audio characteristics:
- Continuous or systolic murmur
- Heard over the breast, bilateral
- Abolished by firm stethoscope pressure or lying down
INNOCENT / FUNCTIONAL MURMURS
15. Still's Murmur (Physiological Systolic)
Cause: Normal physiological turbulence; most common innocent murmur in children (ages 2-6)
Audio characteristics:
- Short, mid-systolic, grade I-II/VI
- Vibratory, musical, "twanging string" quality
- Best heard: left lower sternal border
- Disappears with Valsalva and sitting up
- No radiation, no thrill, normal S1/S2
16. Pulmonary Flow Murmur
Cause: Normal or increased pulmonary flow (pregnancy, anemia, thyrotoxicosis, athletes)
Audio characteristics:
- Soft, crescendo-decrescendo, early to mid-systolic
- Best heard: LUSB (pulmonary area)
- Harsh, medium-pitched
- Increases in high-output states; no radiation, normal S2
SUMMARY COMPARISON TABLES
Systolic Murmurs at a Glance
| Murmur | Location | Timing | Character | Radiation | Pitch |
|---|---|---|---|---|---|
| AS | RUSB | Mid-systolic (ejection) | Harsh, crescendo-decrescendo | Right neck/carotid | Medium-high |
| HOCM | LLSB/apex | Mid-systolic (ejection) | Harsh, crescendo-decrescendo | NOT carotids | Medium |
| MR | Apex | Holosystolic | Blowing, plateau | L axilla (or base) | High |
| MVP | Apex/LLSB | Late systolic (with click) | Blowing | Axilla | High |
| TR | LLSB/xiphoid | Holosystolic | Blowing | R sternal border | High |
| VSD | LLSB (3rd-4th) | Holosystolic | Harsh | Across precordium | High |
| PS | LUSB | Mid-systolic | Crescendo-decrescendo | Left shoulder | Medium |
Diastolic Murmurs at a Glance
| Murmur | Location | Timing | Character | Radiation | Pitch |
|---|---|---|---|---|---|
| AR | LSB (3rd ICS) | Early diastolic | Blowing, decrescendo | LSB to apex | High |
| PR (Graham Steell) | LUSB | Early diastolic | Blowing, decrescendo | LSB | High |
| MS | Apex | Mid-late diastolic (rumble) | Rumbling, after OS | None | Low |
| TS | LLSB | Mid-late diastolic | Rumbling | None | Low |
Dynamic Maneuvers - Complete Summary
| Murmur | Valsalva (Strain) | Standing | Squatting | Handgrip |
|---|---|---|---|---|
| AS | ↓ | ↓ | ↑ | ↓ |
| HOCM | ↑ (hallmark) | ↑ | ↓ | ↓ |
| MR | ↓ | ↓ | ↑ | ↑ |
| MVP click | Earlier click, longer murmur | Earlier click, longer murmur | Later click, shorter murmur | Later click |
| TR | ↓ (↑ inspiration) | ↓ | ↑ | ↑ |
| VSD | ↓ | ↓ | ↑ | ↑ |
| PS | ↓ (↑ inspiration) | ↓ | ↑ | variable |
| AR | ↓ | ↓ | ↑ | ↑ |
| PR | ↓ (↑ inspiration) | ↓ | ↑ | - |
| MS | ↓ | ↓ | ↑ | - |
Key Mnemonics and Distinguishing Pearls
-
HOCM vs AS - Both are crescendo-decrescendo systolic at LLSB/apex, but:
- HOCM: increases with Valsalva and standing; doesn't radiate to carotids; decreases with squatting
- AS: decreases with Valsalva; radiates to carotids; Gallavardin effect at apex
-
MR vs TR (both holosystolic):
- MR: apex; radiates to axilla; increases with expiration, handgrip
- TR: LLSB; increases with inspiration (Carvallo's sign); no axilla radiation
-
AR vs PR (both early diastolic decrescendo at left sternal border):
- AR: A2 timing; wide pulse pressure; increases with handgrip/squatting
- PR: P2 timing; signs of pulmonary HTN; increases with inspiration
-
MS Opening Snap: P2-OS interval inversely proportional to severity. Short = severe (high LA pressure snaps valve early).
-
MVP timing rule: Any maneuver that decreases LV volume (standing, Valsalva, dehydration) moves the click earlier and lengthens the murmur. Any maneuver that increases LV volume (squatting, handgrip) moves the click later and shortens the murmur.
-
Left vs Right sided: Right-sided murmurs (TR, PS, TS, PR) increase with inspiration; left-sided murmurs (MR, AS, MS, AR) are louder in expiration.
-
Acute MR vs Chronic MR: Acute MR (papillary rupture, endocarditis) may have a short, decrescendo murmur that fades before S2 (as LA pressure equilibrates rapidly with LV) - can be easily missed.
Harrison's Principles of Internal Medicine 22E (2025), Chapter 44 - Approach to the Patient with a Heart Murmur, pp. 327-335; Fuster & Hurst's The Heart, 15th Ed, Chapter 2 - Cardiac Auscultation; Goldman-Cecil Medicine, Chapter on Heart Murmurs
Search for recorded audio examples of cardiac murmurs for auscultation practice
Searching the Web
cardiac murmur audio examples auscultation practice free online
Searching the Web
heart sounds murmur recordings medical education website stethoscope
Here's a curated collection of the best free resources for cardiac murmur audio practice:
Cardiac Murmur Audio - Best Resources for Auscultation Practice
YouTube Videos (Audio + Visual Learning)
This Geeky Medics video covers all major murmurs with real audio examples and accentuation maneuvers - widely used for OSCE prep:
This Rhesus Medicine video covers every murmur (AS, AR, MS, MR, PS, PR, TS, TR) with dedicated audio clips for each, with clear timestamps:
Dedicated Auscultation Websites
1. EasyAuscultation.com - easyauscultation.com/heart-sounds
- 100+ real and simulated heart sound recordings
- Free reference guide filterable by auscultation area
- Drills and quizzes with repetition training
- Phonocardiogram waveform shown alongside audio
- Best for: rapid-fire repetition practice
2. PracticalClinicalSkills.com - practicalclinicalskills.com/heart-sounds
- Structured free course: 12 lessons from normal sounds through all major murmurs (AS, AR, MR, MS, MVP, innocent murmur, S3, S4)
- Each lesson has text + recording + anatomical animation
- Quizzes and completion certificates available
- Best for: systematic learning from scratch
3. University of Washington Physical Diagnosis - depts.washington.edu/physdx/heart/demo.html
- Real patient recordings from a medical school
- Covers: AS (early and late), MR, PS, AR/AI, MS, benign murmur, ASD, VSD, PDA, split S2, S3, S4, pericardial rub
- Best for: authentic clinical recordings
App-Based (Mobile)
3M Littmann Learning App - littmann.com/en-us/home/education
- High-fidelity recordings from the makers of Littmann stethoscopes
- Covers heart and lung sounds
- Some content free; full library requires subscription
- Best for: high-quality audio closest to real stethoscope acoustics
Recommended Practice Sequence
- Start with PracticalClinicalSkills for structured lessons with text context
- Use EasyAuscultation for drills and quizzes to reinforce recognition
- Watch the Rhesus Medicine YouTube video to match audio to physiology
- Use the UW Physical Diagnosis site for authentic clinical recordings
- Test yourself using the quiz features on EasyAuscultation without looking at the answer first
The key to mastery is repeated exposure - research on cardiac auscultation training consistently shows that spaced repetition with audio drills significantly improves recognition accuracy compared to passive listening alone.
This is a shared conversation. Sign in to Orris to start your own chat.