Physiology of appetite regulation
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"appetite regulation" AND "hypothalamus"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
I now have comprehensive data from multiple authoritative textbooks. Let me compile a thorough, well-organized answer.
Physiology of Appetite Regulation
Appetite regulation is a multi-layered system that integrates signals from the gastrointestinal tract, adipose tissue, pancreas, and the CNS to balance short-term meal initiation/termination with long-term energy homeostasis.
1. Central Command: The Hypothalamus
The hypothalamus is the primary integrating center for appetite and energy balance. Two key regions are classically defined:
- Lateral Hypothalamic Area (LHA) - the "hunger (feeding) center." Stimulation drives eating; destruction causes anorexia.
- Ventromedial/Ventral Posterior Nucleus (VMN/VPN) - the "satiety center." Stimulation inhibits eating; lesions cause hyperphagia and obesity.
Both centers receive converging input from the arcuate nucleus, which acts as the primary sensor and relay of peripheral metabolic signals.
- Costanzo Physiology 7th Ed., p. 352
2. The Arcuate Nucleus: Two Opposing Neuronal Populations
The arcuate nucleus contains two functionally antagonistic populations of neurons:
| Neuron Type | Peptides Released | Effect |
|---|---|---|
| Orexigenic | NPY (neuropeptide Y), AgRP (agouti-related protein) | Increases appetite, stimulates feeding |
| Anorexigenic | POMC (pro-opiomelanocortin), CART (cocaine- and amphetamine-regulated transcript) | Decreases appetite, increases energy expenditure |
POMC neurons release the cleavage product alpha-melanocyte stimulating hormone (α-MSH), which binds MC3R and MC4R melanocortin receptors on second-order neurons to promote satiety and activate descending sympathetic pathways that increase energy expenditure. Importantly, ~4% of individuals with severe early-onset obesity carry mutations in MC3R or MC4R.
NPY/AgRP neurons are activated by energy deficits. AgRP acts as an inverse agonist at MC3R/MC4R, directly blocking the action of α-MSH - so when orexigenic neurons are active, they not only signal hunger but also simultaneously silence the satiety pathway.
- Medical Physiology (Boron & Boulpaep), pp. 1472-1473
3. Secondary Neuron Projections
The POMC/CART and NPY/AgRP neurons project to five major second-order areas:
- Lateral Hypothalamic Area (LHA) - NPY/AgRP neurons stimulate secondary neurons that release the orexigenic peptides melanin-concentrating hormone (MCH) and orexins A and B (hypocretins). POMC neurons inhibit these.
- Ventromedial Hypothalamic Nucleus (VMN) - satiety center.
- Dorsomedial Hypothalamic Nucleus (DMN).
- Paraventricular Nucleus (PVN) - projects to the cerebral cortex and brainstem; α-MSH activates MC4R here to generate satiety signals.
- Periventricular nucleus - receives GLP-1 input.
- Medical Physiology (Boron & Boulpaep)
4. Peripheral Signals - Long-Term (Adipostatic) Regulators
These signals reflect total body energy stores:
Leptin
- Source: Adipocytes, in proportion to fat mass
- Action: Crosses the blood-brain barrier → stimulates arcuate POMC/CART neurons AND suppresses NPY/AgRP neurons → decreases appetite + increases energy expenditure
- Time course: Intermediate- to long-term regulator (half-life ~75 min; not acutely affected by single meals)
- Receptor: LEP-R (tyrosine kinase-associated, signals via JAK2/STAT), richly expressed in arcuate nucleus
- Leptin-deficient Ob/Ob mice gain >100% body weight; parabiosis experiments were the key evidence for a blood-borne satiety factor (see classic parabiosis figure below)
- Most obese humans are not leptin-deficient but are leptin resistant (plasma levels actually rise with BMI)
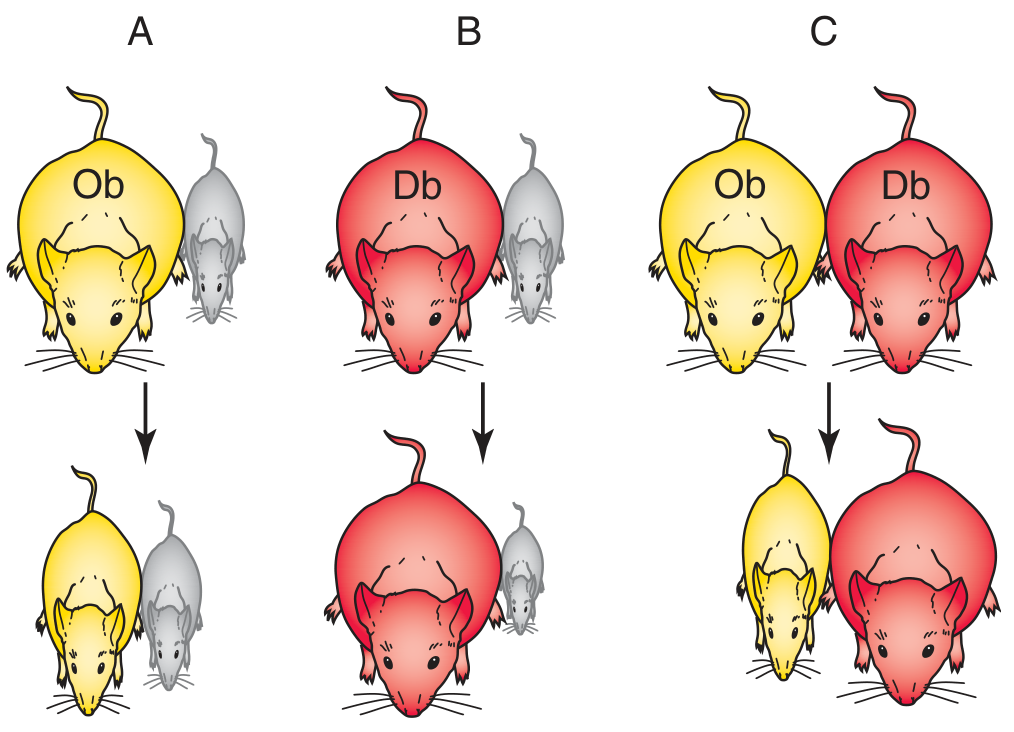
Parabiosis experiments: Ob mouse (leptin-deficient) loses weight when joined to wild-type (A). Db mouse (leptin receptor-deficient) overproduces leptin, causing the joined wild-type to starve (B). Ob mouse loses weight when joined to Db mouse because the Db mouse over-secretes leptin (C). - Medical Physiology
Insulin
-
Source: Pancreatic β cells; fluctuates throughout the day with meals
-
Action: Same as leptin - stimulates POMC neurons, suppresses NPY/AgRP neurons → decreases appetite
-
Time course: Short- to intermediate-term regulator (levels change acutely with each meal)
-
Costanzo Physiology 7th Ed., p. 352 | Medical Physiology, p. 1471
5. Peripheral Signals - Short-Term (Meal-by-Meal) Regulators
These signals reflect the current state of food ingestion and gut filling:
Ghrelin (the hunger hormone)
- Source: Gastric mucosal cells, secreted just before meals (rises during fasting)
- Action: Activates NPY/AgRP neurons and inhibits POMC neurons → increases appetite and food intake
- Unique feature: The only known circulating orexigenic (appetite-stimulating) hormone
- Ghrelin opposes leptin; starvation and weight loss strongly stimulate ghrelin secretion
Cholecystokinin (CCK)
- Source: I cells of the duodenum and jejunum, released in response to protein and fat
- Action: Binds CCK-1 receptors on vagal afferents → signals to the brainstem → promotes meal termination (satiation). Also delays gastric emptying.
- Proof of physiologic role: CCK receptor antagonists increase meal size
- Note: CCK causes satiation (stops the current meal) but does not affect satiety (duration until next meal)
GLP-1 (Glucagon-like Peptide-1)
- Source: L cells of the ileum and colon, released in response to luminal nutrients
- Action: Stimulates insulin secretion (incretin effect) + delays gastric emptying + inhibits appetite. GLP-1 receptors are found in the arcuate nucleus, PVN, and dorsomedial hypothalamus.
- Central administration of GLP-1 also suppresses food intake.
- Basis for GLP-1 receptor agonists (semaglutide, liraglutide) as anti-obesity treatments.
Peptide YY (PYY 3-36)
- Source: L cells of the ileum and colon, secreted after meals (in proportion to caloric intake)
- Action: Acts on Y2 receptors in the arcuate nucleus to decrease hunger. Also inhibits ghrelin secretion. Signals that digestion is complete.
Amylin
- Source: Pancreatic β cells (co-secreted with insulin)
- Action: Acts on the GI tract and hypothalamus to inhibit appetite. Its analog pramlintide is used clinically.
Summary table of GI satiety/hunger signals:
| Peptide | Source | Timing | Effect |
|---|---|---|---|
| Ghrelin | Gastric mucosa | Pre-meal (fasting) | Orexigenic (increases appetite) |
| CCK | Duodenum/jejunum | During meal | Satiation (meal termination via vagus) |
| GLP-1 | Ileum/colon L cells | During/after meal | Anorexigenic + incretin |
| PYY 3-36 | Ileum/colon L cells | After meal | Anorexigenic; inhibits ghrelin |
| Amylin | Pancreatic β cells | During meal | Anorexigenic |
- Sleisenger & Fordtran's GI and Liver Disease | Costanzo Physiology 7th Ed. | Goldman-Cecil Medicine
6. Brain Regions Beyond the Hypothalamus
Appetite regulation extends well beyond the hypothalamus:
| Region | Role | Key Neurotransmitters |
|---|---|---|
| Hypothalamus | Energy homeostasis | POMC, NPY, AgRP, CART, norepinephrine, GABA |
| Ventral striatum | Reward aspects of food (hedonic eating) | Dopamine |
| Prefrontal cortex | Impulse control, executive function | Dopamine, norepinephrine, glutamate |
| Brainstem / NTS | Integrates vagal GI signals (CCK, gastric distension) | GLP-1 |
| Cortex | Social meaning of eating | - |
- Goldman-Cecil Medicine, p. 2371
7. Key Integrating Concept: Hunger vs. Satiety Balance
The balance between the NPY/AgRP (orexigenic) and POMC/CART (anorexigenic) arms of the arcuate nucleus is the final common pathway:
- Energy deficit (low leptin, low insulin, high ghrelin) → NPY/AgRP neurons dominate → hunger, increased food intake, decreased energy expenditure
- Energy surplus (high leptin, high insulin, high PYY/GLP-1) → POMC/CART neurons dominate → satiety, decreased food intake, increased energy expenditure via sympathetic activation
This bidirectional gating mechanism, modulated continuously by both long-term adipostatic signals and short-term meal-derived signals, maintains energy homeostasis.
8. Clinical Relevance
- Leptin resistance is present in the majority of obese individuals (plasma leptin is elevated but ineffective)
- MC4R mutations account for the most common form of monogenic human obesity (~4% of severe early-onset cases)
- Bariatric surgery markedly lowers ghrelin and raises PYY/GLP-1 - contributing to its appetite-suppressing effects beyond mere restriction
- GLP-1 receptor agonists (semaglutide, liraglutide) exploit the central anorexigenic GLP-1 pathway for obesity treatment
- Orexin (hypocretin) deficiency in the LHA causes narcolepsy - illustrating the overlap between appetite regulation and sleep/wake circuits
Sources:
- Costanzo Physiology, 7th Ed., pp. 350-353
- Medical Physiology (Boron & Boulpaep), pp. 1471-1474
- Goldman-Cecil Medicine, p. 2371
- Sleisenger & Fordtran's GI and Liver Disease, pp. 1937-1950
- Principles of Neural Science (Kandel), 6th Ed.
Pharmacotherapy of obesity
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"obesity" AND "pharmacotherapy" AND "GLP-1"
Searching the Web
obesity pharmacotherapy 2024 2025 approved drugs semaglutide tirzepatide guidelines
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive data from Harrison's 22E (2025), Lippincott Pharmacology, Miller's Anesthesia, and multiple supporting textbooks, plus current guidelines (EASO 2025, Canadian 2025). I have enough to write a thorough, well-organized answer.
Pharmacotherapy of Obesity
Pharmacotherapy is indicated as an adjunct to lifestyle modification (diet + exercise + behavioral therapy) when BMI ≥30 kg/m², or ≥27 kg/m² with at least one weight-related comorbidity (hypertension, type 2 diabetes, dyslipidemia, OSA). The goal is not solely weight loss - current guidelines (EASO 2025, Canadian 2025) emphasize a complications-guided approach: reducing cardiovascular events, improving heart failure, reversing metabolic dysfunction, and improving quality of life.
Overview: FDA-Approved Agents for Long-Term Use
The FDA-approved agents for chronic weight management in adults (as of 2025):
| Drug | Class | Route | Dose | Approx. Placebo-Subtracted Weight Loss |
|---|---|---|---|---|
| Orlistat | Lipase inhibitor | Oral | 120 mg TID | ~2.7-4.1% |
| Phentermine/topiramate ER | Adrenergic + anticonvulsant | Oral | Up to 15/92 mg daily | ~8-10% |
| Naltrexone/bupropion SR | Opioid antagonist + NE/DA reuptake inhibitor | Oral | 32/360 mg daily | ~4-5% |
| Liraglutide 3.0 mg | GLP-1 RA | SC daily | 3.0 mg/day | ~5-6% |
| Semaglutide 2.4 mg | GLP-1 RA | SC weekly | 2.4 mg/week | ~12-15% |
| Tirzepatide | Dual GLP-1/GIP RA | SC weekly | 5/10/15 mg/week | ~12-21% |
| Setmelanotide | MC4R agonist | SC daily | Titrated | For rare MC4R pathway defects only |
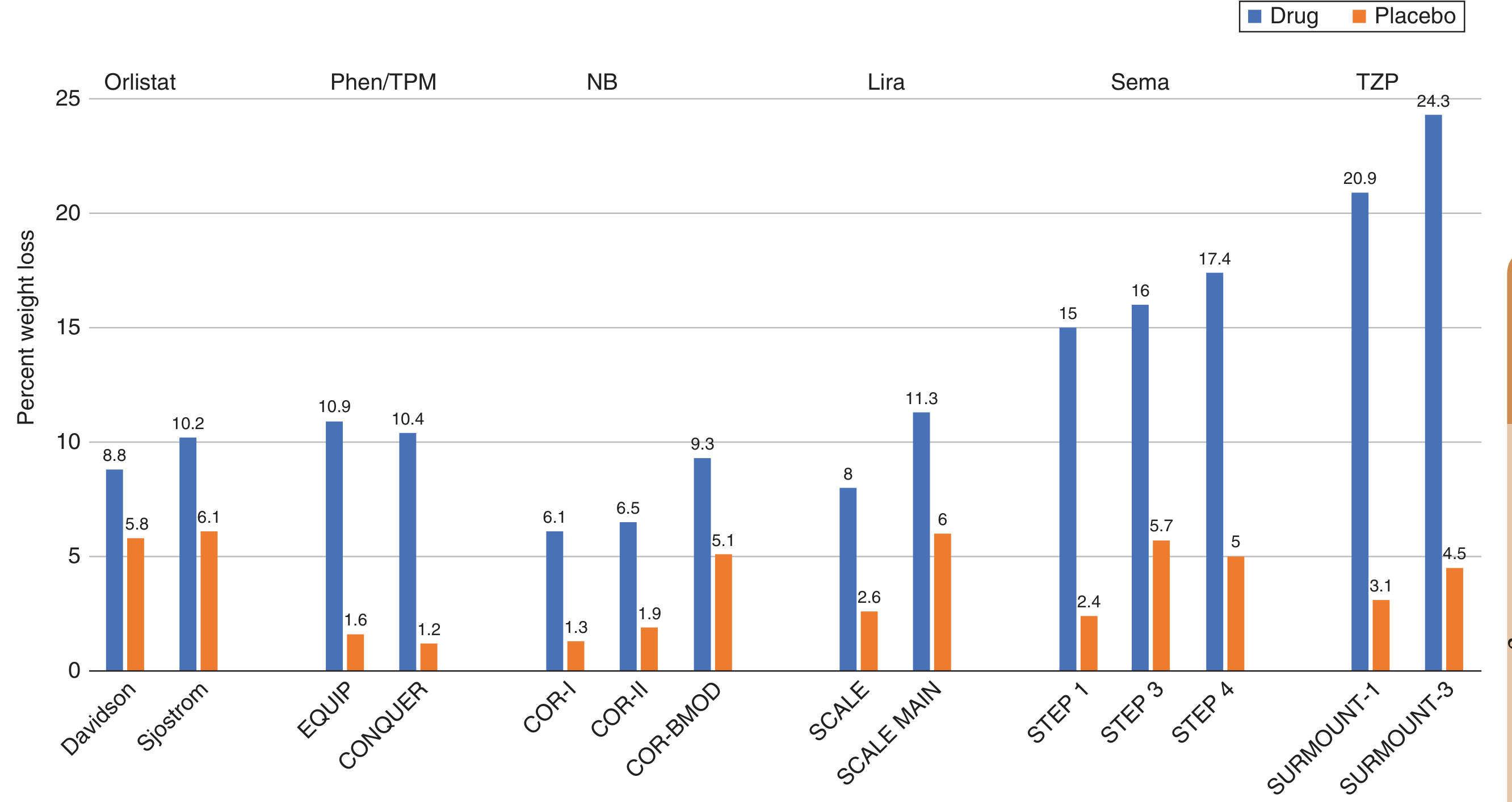
Figure from Harrison's Principles of Internal Medicine 22E (2025) - one-year mean weight loss (drug vs. placebo) across pivotal trials for each approved antiobesity medication.
1. Orlistat (Xenical; OTC: Alli)
Class: Gastrointestinal lipase inhibitor
Mechanism: A synthetic, hydrogenated derivative of lipostatin (from Streptomyces toxytricini). Forms a covalent bond with the active site of pancreatic, gastric, and carboxylester lipases in the GI lumen, preventing hydrolysis of dietary triglycerides into absorbable fatty acids. Blocks ~30% of dietary fat absorption. Fecal fat returns to normal within 48-72 h of stopping.
Dose: 120 mg three times daily with meals (prescription); 60 mg TID (OTC)
Weight loss: ~2.7-4.1% placebo-subtracted at 1 year. Also modestly lowers blood glucose and improves lipids.
Adverse effects: All GI - oily spotting, flatulence, fecal urgency, steatorrhea, fecal incontinence. These improve with dietary fat restriction. Fat-soluble vitamin (A, D, E, K, β-carotene) malabsorption - supplementation is required.
Key points:
-
Only peripherally acting agent (minimal systemic absorption <1%)
-
Approved for children ≥12 years
-
FDA-approved for OTC use (2007)
-
No cardiovascular or CNS effects
-
Harrison's Principles of Internal Medicine 22E, p. 3236 | Miller's Anesthesia 10e
2. Phentermine / Topiramate ER (Qsymia)
Class: Sympathomimetic amine + anticonvulsant (combination)
Mechanism:
- Phentermine (Schedule IV): Releases norepinephrine and dopamine and inhibits their reuptake in the CNS → suppresses appetite and increases resting metabolic rate. Most commonly prescribed single antiobesity drug in the USA.
- Topiramate ER: Anticonvulsant; independently causes weight loss (mechanism not fully established - likely includes glutamate receptor modulation and carbonic anhydrase inhibition). Added to counteract phentermine's stimulant effects (sedation from topiramate balanced by phentermine).
Dose: Start 3.75/23 mg daily, titrate to max 15/92 mg daily
Weight loss: ~8-10% placebo-subtracted at 1 year (EQUIP and CONQUER trials)
Rule of thumb: If patient does not achieve ≥5% weight loss at 12 weeks on maximum dose, discontinue.
Adverse effects: Dry mouth, paresthesias (tingling of extremities), insomnia, headache, constipation, palpitations, dysgeusia. Do not stop abruptly - risk of precipitating seizures.
Contraindications:
-
Pregnancy (topiramate causes cleft palate and other birth defects) - pregnancy test required before starting; use effective contraception
-
Glaucoma, hyperthyroidism, MAOIs within 14 days
-
Uncontrolled hypertension (phentermine component)
-
Harrison's 22E | Lippincott Pharmacology, p. 756
3. Naltrexone / Bupropion SR (Contrave)
Class: Opioid receptor antagonist + dopamine/NE reuptake inhibitor
Mechanism: Works via the mesolimbic reward system and the hypothalamic melanocortin pathway:
- Bupropion stimulates hypothalamic POMC neurons (anorexigenic) → triggers α-MSH release → satiety. Bupropion also inhibits dopamine/NE reuptake.
- Naltrexone blocks the autoinhibitory opioid feedback that POMC neurons exert on themselves - normally, β-endorphin (a POMC product) feeds back to inhibit POMC activity. Naltrexone removes this brake, amplifying bupropion's effect on POMC neurons. Together, they curb food cravings and reward-driven eating.
Dose: Titrated to 32 mg naltrexone / 360 mg bupropion SR per day (divided BID)
Weight loss: ~4-5% placebo-subtracted. ~20% of patients achieve ≥10% weight loss (COR trials).
Adverse effects: Nausea, headache, dry mouth, dizziness, constipation, hypertension, tachycardia. Black box warning: risk of suicidal ideation (bupropion component). Increased blood pressure and pulse.
Contraindications:
-
Seizure disorders or any condition predisposing to seizures (bupropion lowers seizure threshold)
-
Uncontrolled hypertension
-
Chronic opioid use (naltrexone will precipitate withdrawal)
-
MAOIs within 14 days
-
Pregnancy
-
Harrison's 22E | Lippincott Pharmacology
4. Liraglutide 3.0 mg (Saxenda)
Class: GLP-1 receptor agonist (GLP-1 RA)
Mechanism: Synthetic analogue of human GLP-1. Binds GLP-1 receptors in the arcuate nucleus, brainstem, and GI tract → reduces hunger, increases satiety, slows gastric emptying → decreased caloric intake. Also stimulates insulin secretion and inhibits glucagon (incretin effect). Note: the diabetes dose is 1.8 mg; the obesity dose is 3.0 mg daily.
Dose: SC injection, titrated from 0.6 mg/day up to 3.0 mg/day over 5 weeks
Weight loss: ~5-6% placebo-subtracted (SCALE trials). ~33% of patients achieve >10% weight loss. The SCALE MAIN trial showed 11.3% mean total weight loss vs. 6.0% for placebo.
Adverse effects: Nausea, vomiting, diarrhea, constipation (usually transient), elevated heart rate, acute gallbladder disease, pancreatitis. Black box warning: risk of thyroid C-cell tumors in rodents (unknown relevance in humans).
Contraindications: Personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia type 2 (MEN2).
Approved: Children ≥12 years old.
5. Semaglutide 2.4 mg (Wegovy) - "Second-Generation"
Class: GLP-1 receptor agonist
Mechanism: Same as liraglutide but with chemical modifications enabling once-weekly dosing and a longer half-life. Reduces hunger via central GLP-1 receptors (arcuate, PVN, brainstem), decreases gastric emptying, and independently improves cardiovascular outcomes.
Dose: SC injection once weekly, titrated from 0.25 mg/week over 16-20 weeks to 2.4 mg/week. (Approved for type 2 diabetes at up to 2.0 mg/week SC since 2017; approved for obesity at 2.4 mg/week in 2021 for adults, 2022 for adolescents.)
Weight loss (STEP program):
- STEP 1-4: 6.2-14.8% placebo-subtracted at 68 weeks
- STEP 5: 12.6% at 104 weeks
- STEP TEENS: 16.1% BMI reduction in adolescents vs. +0.6% for placebo
Key cardiovascular trial - SELECT: 20% relative reduction in major adverse cardiovascular events (MACE) in patients with preexisting CVD and overweight/obesity (without diabetes). This led to semaglutide being the first weight-loss drug approved to reduce CV events (BMI ≥27 + established CVD).
STEP-HFpEF: Improved heart failure symptoms, physical function, and reduced inflammation in HFpEF patients.
Adverse effects and contraindications: Same as liraglutide (nausea/vomiting most common; contraindicated in MTC or MEN2 history).
- Harrison's 22E, p. 3236-3237 | Sabiston Surgery
6. Tirzepatide (Zepbound) - "Third-Generation" Dual Agonist
Class: Dual GLP-1 / GIP (gastric inhibitory polypeptide) receptor agonist
Mechanism: The first-in-class dual incretin agonist. Engineered from the native GIP sequence with agonist activity at both GLP-1R and GIPR. Half-life ~117 h (allows once-weekly dosing). GLP-1R affinity is ~5x weaker than native GLP-1, but GIP receptor agonism appears to act synergistically with GLP-1R activation in the brain - producing greater weight loss than GLP-1 agonism alone. GIP also acts on adipose tissue directly to improve lipid metabolism.
Dose: SC once weekly - 2.5 mg starting dose, titrated by 2.5 mg/month to maximum 15 mg/week
Weight loss (SURMOUNT program):
- SURMOUNT-1: ~20.9% total body weight loss at 15 mg (vs. 3.1% placebo) at 72 weeks
- SURMOUNT-3: ~24.3% total body weight loss at 15 mg
- Placebo-subtracted weight loss ranged from 11.6% to 21.4% across SURMOUNT 1-4 trials
Approvals: Type 2 diabetes (2022); chronic weight management in adults (2023). Now recommended by EASO (2025) and Canadian guidelines (2025) as first-line for obesity with comorbidities.
Additional indications: HFpEF with obesity (SUMMIT trial); MASH/metabolic liver disease.
Adverse effects: Same GI profile as GLP-1 RAs (nausea, diarrhea, constipation, vomiting - mild, transient). Contraindicated in personal/family history of MTC or MEN2.
- Harrison's 22E, p. 3237 | Robbins Pathology | Sabiston Surgery
7. Setmelanotide (Imcivree)
Class: MC4R agonist
Mechanism: Directly activates MC4R melanocortin receptors (the receptor normally activated by α-MSH downstream of POMC neurons). Bypasses the defective upstream signaling in rare genetic obesity syndromes.
Indication: Specifically for monogenic obesity due to:
- POMC deficiency
- Proprotein convertase subtilisin/kexin type 1 (PCSK1) deficiency
- Leptin receptor (LEPR) deficiency
Dose: SC daily; approved for children ≥6 years old
This drug exemplifies the precision medicine approach to obesity - targeting the exact molecular defect rather than broadly suppressing appetite.
- Harrison's 22E | Miller's Anesthesia 10e
8. Short-Term Agents (Not for Chronic Use)
Phentermine alone (Schedule IV): Adrenergic agonist; approved only for short-term use (~3 months). Most widely prescribed single antiobesity drug in the USA. Increases NE and dopamine release → appetite suppression. Avoid in uncontrolled hypertension, CAD, hyperthyroidism, agitation, or within 14 days of MAOIs.
Diethylpropion (Schedule IV): Similar adrenergic mechanism to phentermine; approved short-term.
9. Treatment Algorithm and Current Guidelines
Indications for pharmacotherapy:
- BMI ≥30 kg/m², OR
- BMI ≥27 kg/m² + at least one weight-related comorbidity
Drug selection - 2025 EASO/Canadian framework (complications-guided):
| Clinical Context | Preferred Agent |
|---|---|
| Obesity alone (no major comorbidity) | Semaglutide or tirzepatide |
| Obesity + T2DM or prediabetes | Tirzepatide (greatest metabolic benefit) or semaglutide |
| Obesity + established CVD (ASCVD) | Semaglutide 2.4 mg (SELECT trial - 20% MACE reduction) |
| Obesity + HFpEF | Semaglutide or tirzepatide (STEP-HFpEF, SUMMIT trials) |
| Obesity + MASH/fatty liver | Tirzepatide first-line (semaglutide likely to join - ESSENCE trial 2025) |
| Cannot access injectables | Phentermine/topiramate ER or naltrexone/bupropion |
| Rare MC4R pathway defect | Setmelanotide |
Key rules:
- All pharmacotherapy should accompany lifestyle intervention (not replace it)
- If <5% weight loss at 12 weeks on maximum tolerated dose → reassess, consider switching
- These drugs generally require long-term or indefinite use - weight regain is the norm on discontinuation
- GLP-1 RA/tirzepatide: hold 1-2 weeks before elective surgery (delayed gastric emptying → aspiration risk)
10. Drugs Withdrawn from Market
- Lorcaserin (serotonin 2C agonist) - withdrawn 2020 due to increased cancer risk
- Sibutramine (SNRI) - withdrawn 2010 due to increased CV events (SCOUT trial)
- Rimonabant (CB1 antagonist) - never approved in USA; withdrawn in Europe 2008 due to severe psychiatric adverse effects (depression, suicidality)
Summary: Mechanism-Based Classification
PERIPHERAL ACTION
└── Orlistat (lipase inhibitor - GI only)
CENTRAL/HYPOTHALAMIC
├── Phentermine, diethylpropion (NE/DA release - short-term)
├── Naltrexone/bupropion (POMC pathway + mesolimbic reward)
└── Setmelanotide (MC4R agonist - genetic obesity)
INCRETIN-BASED (GI + CNS)
├── Liraglutide 3.0 mg (GLP-1 RA - daily SC)
├── Semaglutide 2.4 mg (GLP-1 RA - weekly SC) ← CV outcomes benefit
└── Tirzepatide 15 mg (dual GLP-1/GIP RA - weekly SC) ← greatest weight loss
COMBINATION (CNS)
└── Phentermine/topiramate ER (adrenergic + anticonvulsant)
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Ch. 414
- Lippincott Illustrated Reviews: Pharmacology, Ch. 22
- Miller's Anesthesia 10e, Ch. on Pharmacotherapy for Weight Loss
- Sabiston Textbook of Surgery (Glucagon-Like Peptide-1 Receptor Agonists)
- EASO Framework for Pharmacological Treatment of Obesity, Oct 2025
- Canadian Clinical Practice Guideline 2025
- PMID 40952752 (GLP-1 RA in pediatric obesity, 2025 meta-analysis)
Physiology of calcium metabolism
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.