Barbiturates according to shanbhag pharmacology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed. Here is a comprehensive answer on Barbiturates based on standard pharmacology textbook content (Goodman & Gilman and Katzung), aligned with what Shanbhag pharmacology covers:
Barbiturates - Pharmacology
Note: Shanbhag's Review of Pharmacology is not available in this library. The following covers barbiturate pharmacology comprehensively as presented in Goodman & Gilman's The Pharmacological Basis of Therapeutics and Katzung's Basic & Clinical Pharmacology - the primary references Shanbhag's text is itself based on.
1. Chemistry / Structure
Barbiturates are derivatives of barbituric acid (2,4,6-trioxohexahydropyrimidine), a six-membered pyrimidine ring:
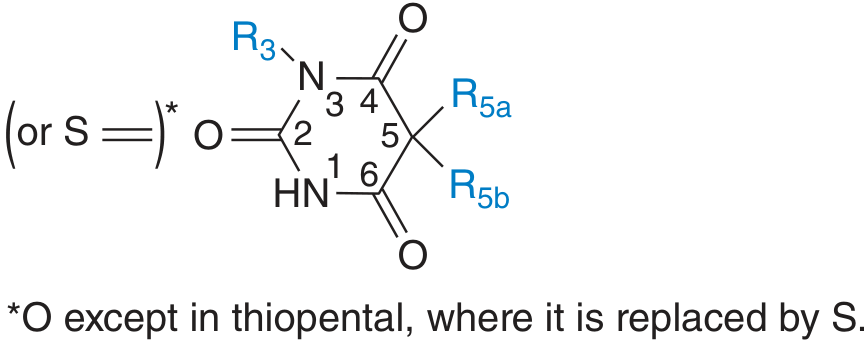
- Barbituric acid itself has no CNS depressant activity
- Activity is conferred by alkyl or aryl groups at position C5
- Replacement of O at C2 by sulfur gives thiobarbiturates (e.g., thiopental) - more lipid-soluble, faster onset, shorter duration
Structure-Activity Relationships:
- Increased lipid solubility → decreased duration, decreased latency, faster metabolism, increased hypnotic potency
- Long-chain substitutions at C5 → anticonvulsant activity
- Phenyl group at C5 → anticonvulsant property (e.g., phenobarbital)
- N-methyl substitution → shorter action (methohexital)
2. Classification
| Class | Example | Onset | Duration |
|---|---|---|---|
| Ultra-short acting | Thiopental, Methohexital | Seconds (IV) | 5-15 min |
| Short-acting | Secobarbital, Pentobarbital | 10-15 min | 3-4 h |
| Intermediate-acting | Amobarbital, Butabarbital | 45-60 min | 6-8 h |
| Long-acting | Phenobarbital, Mephobarbital | 60 min | 10-12 h |
3. Mechanism of Action
Barbiturates act primarily at GABA-A receptors (ligand-gated Cl⁻ channels):
- They enhance GABA-mediated Cl⁻ influx by binding to a specific site (distinct from the benzodiazepine site)
- At low concentrations: they increase the duration of Cl⁻ channel opening (unlike benzodiazepines which increase frequency)
- At high/anesthetic concentrations: they can directly open Cl⁻ channels even without GABA (this explains their greater danger in overdose vs. benzodiazepines)
- They also inhibit AMPA receptors (glutamate-mediated excitatory neurotransmission), contributing to CNS depression
- All excitable tissues are reversibly depressed, but CNS is most sensitive
4. Pharmacokinetics (ADME)
Absorption:
- Oral administration: Na⁺ salts absorbed faster than free acids, especially from liquid preparations
- Onset: 10-60 min orally; delayed by food
- IM injection: must be deep into large muscles (superficial injection causes pain/necrosis)
- IV: reserved for status epilepticus (phenobarbital) or anesthesia induction (thiopental, methohexital)
Distribution:
- Wide distribution throughout the body
- Readily cross the placenta (teratogenic risk)
- Highly lipid-soluble agents (thiopental, methohexital): rapid redistribution to muscle/fat after IV injection → rapid awakening in 5-15 min despite long elimination half-life (redistribution kinetics, NOT metabolism, determines duration)
Metabolism:
- Nearly complete hepatic metabolism (except phenobarbital and aprobarbital)
- Key biotransformation: oxidation of radicals at C5 - terminates biological activity
- N-glycosylation important for phenobarbital
- Other pathways: N-hydroxylation, desulfuration (thiobarbiturates → oxybarbiturates), ring opening, N-dealkylation (mephobarbital → phenobarbital, an active metabolite)
- Phenobarbital (~25%) and aprobarbital (nearly all): excreted unchanged in urine
Excretion:
- Renal excretion of phenobarbital can be greatly increased by:
- Osmotic diuresis
- Alkalinization of urine (phenobarbital is a weak acid, pKa ~7.2; alkaline urine ionizes it → traps in urine → ion trapping)
- This is the basis for treating phenobarbital overdose with sodium bicarbonate
Drug Interactions - Enzyme Induction:
- Chronic barbiturate use markedly induces hepatic microsomal enzymes: CYP1A2, CYP2C9, CYP2C19, CYP3A4, glucuronyl transferase
- This accelerates metabolism of many drugs: warfarin, oral contraceptives, corticosteroids, other barbiturates, vitamin K and D, steroid hormones, cholesterol, bile salts
- Self-induction partly accounts for pharmacokinetic tolerance
- Also induces ALA synthase (mitochondrial) - dangerous in porphyria
5. Pharmacological Effects
Central Nervous System
- Dose-dependent CNS depression: sedation → hypnosis → anesthesia → coma → death
- Non-selective: depress all CNS functions (unlike benzodiazepines which have a ceiling effect)
- No analgesia - some barbiturates may actually lower pain threshold (hyperalgesia) - important point; pain can cause paradoxical excitement
- Reduce sleep latency; decrease REM sleep (REM rebound on withdrawal)
- EEG: increase beta waves at low doses; suppress EEG activity at anesthetic doses
Cerebrovascular effects (at anesthetic doses):
- Decrease cerebral blood flow (CBF), cerebral blood volume (CBV), and intracranial pressure (ICP)
- Decrease cerebral metabolic rate (CMRO2) - dose-dependent, up to burst suppression
- Useful in management of raised ICP and space-occupying lesions
- Neuroprotection from focal cerebral ischemia (stroke, surgical)
- NOT effective for global ischemia (cardiac arrest)
- Anticonvulsant (except methohexital which activates epileptic foci - useful in ECT)
Cardiovascular System
- Depression of myocardial contractility (direct negative inotropic effect)
- Peripheral vasodilation → fall in systemic blood pressure
- Less baroreceptor reflex inhibition than propofol → compensatory tachycardia limits hypotension
- Rapid IV injection can cause cardiovascular collapse before anesthesia (apnea, laryngospasm)
- Risk greater with hypovolemia, cardiac tamponade, cardiomyopathy
Respiratory System
- Respiratory depressants: decrease minute ventilation (reduced tidal volume and rate)
- Decrease ventilatory response to hypercapnia and hypoxia
- Usual induction dose causes transient apnea
- Hypnotic doses contraindicated in pulmonary insufficiency
- Barbiturates do NOT produce muscle relaxation
Hepatic Effects
- Acute: inhibit CYPs and biotransformation of other drugs
- Chronic: induce smooth ER proliferation and CYP enzymes (see enzyme induction above)
- Trigger ALA synthase → absolutely contraindicated in acute intermittent porphyria and porphyria variegata
Renal Effects
- Severe oliguria or anuria in acute poisoning - secondary to marked hypotension
6. Therapeutic Uses
| Indication | Drug | Notes |
|---|---|---|
| Anesthesia induction | Thiopental, methohexital | Largely replaced by propofol |
| Status epilepticus | Phenobarbital IV | Still used |
| Epilepsy (long-term) | Phenobarbital, primidone | Second-line; generalized tonic-clonic, partial seizures |
| Sedation/hypnosis | Amobarbital, secobarbital | Largely replaced by BZDs |
| Raised ICP | Thiopental (pentobarbital coma) | Barbiturate coma for refractory ICP |
| Neonatal seizures | Phenobarbital | Drug of choice |
7. Adverse Effects
- Aftereffects (Hangover): Residual drowsiness, mood distortion, impaired fine motor skills, nausea, vomiting, vertigo - may persist next day
- Paradoxical excitement: Excitement/inebriation-like state instead of sedation; common in elderly, debilitated patients, and N-methyl barbiturates; also with pain (lower pain threshold)
- Hypersensitivity: Allergic reactions more common in asthma, urticaria, angioedema; localized edema (eyelids, cheeks, lips); erythematous dermatitis; rarely exfoliative dermatitis from phenobarbital (can be fatal, associated with fever, delirium, liver damage)
- Tolerance and Dependence: Both pharmacokinetic (enzyme induction) and pharmacodynamic tolerance develop; physical dependence causes severe withdrawal (more dangerous than opioid withdrawal - can be fatal with grand mal seizures)
- Abuse potential: High (Schedule IV/II drugs)
- Porphyria crisis: Absolutely contraindicated in acute intermittent porphyria
8. Tolerance and Dependence
- Pharmacokinetic tolerance: Enzyme induction → increased metabolism of barbiturate itself
- Pharmacodynamic tolerance: CNS adaptation at receptor level
- Physical dependence: Abrupt withdrawal after chronic use causes a dangerous abstinence syndrome:
- Anxiety, insomnia, tremors, delirium, grand mal seizures, hyperthermia
- Can be life-threatening (unlike opioid withdrawal)
- Treatment: gradual dose tapering, substitution with long-acting barbiturate (phenobarbital)
9. Acute Barbiturate Poisoning (Overdose)
Clinical features:
- Mild: drowsiness, slurred speech, ataxia, nystagmus, emotional lability
- Severe: stupor → deep coma → respiratory arrest
- Flaccid coma + small reactive pupils + hypothermia + hypotension - hallmark (few other causes)
- Respiratory depression is the primary cause of death
Management:
- Airway, breathing, circulation (supportive)
- Activated charcoal (if early)
- Alkalinization of urine (sodium bicarbonate) + forced diuresis → enhances excretion of phenobarbital
- Hemodialysis for severe cases
- No specific antidote (unlike benzodiazepines which have flumazenil)
- Caution: Rapid lowering of levels in chronic users can precipitate withdrawal seizures
Coma blisters: A dermatological sign - blisters at pressure points in barbiturate-induced coma (also called "coma bullae" or barbiturate blisters)
10. Contraindications
- Acute intermittent porphyria / porphyria variegata (absolute)
- Pulmonary insufficiency (hypnotic doses)
- Severe hepatic impairment
- Rapid IV injection in hemodynamically compromised patients
- Known hypersensitivity
11. Key Comparisons: Barbiturates vs. Benzodiazepines
| Feature | Barbiturates | Benzodiazepines |
|---|---|---|
| GABA-A effect | Increase duration of Cl⁻ channel opening; direct opening at high doses | Increase frequency of Cl⁻ channel opening |
| Ceiling effect | No - can cause coma/death | Yes - safer in overdose |
| Enzyme induction | Yes (CYPs) | No |
| Antidote | None | Flumazenil |
| Analgesia | No (hyperalgesia possible) | No |
| Dependence | Severe, dangerous withdrawal | Less severe |
| Current use | Limited; anesthesia, epilepsy | Preferred for anxiety/insomnia |
Sources: Goodman & Gilman's The Pharmacological Basis of Therapeutics, 14th ed., Chapter 22; Katzung's Basic & Clinical Pharmacology, 16th ed., Chapter 22 & 25
This is a shared conversation. Sign in to Orris to start your own chat.