Paranasal air sinuses
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have rich content from multiple authoritative textbooks plus excellent anatomical diagrams. I'll compile the comprehensive answer.
Paranasal Air Sinuses
The paranasal air sinuses are four pairs of air-filled cavities within the bones of the skull that communicate with the nasal cavity. They are named after the bones in which they reside: maxillary, frontal, ethmoidal, and sphenoidal.
Anatomical Overview
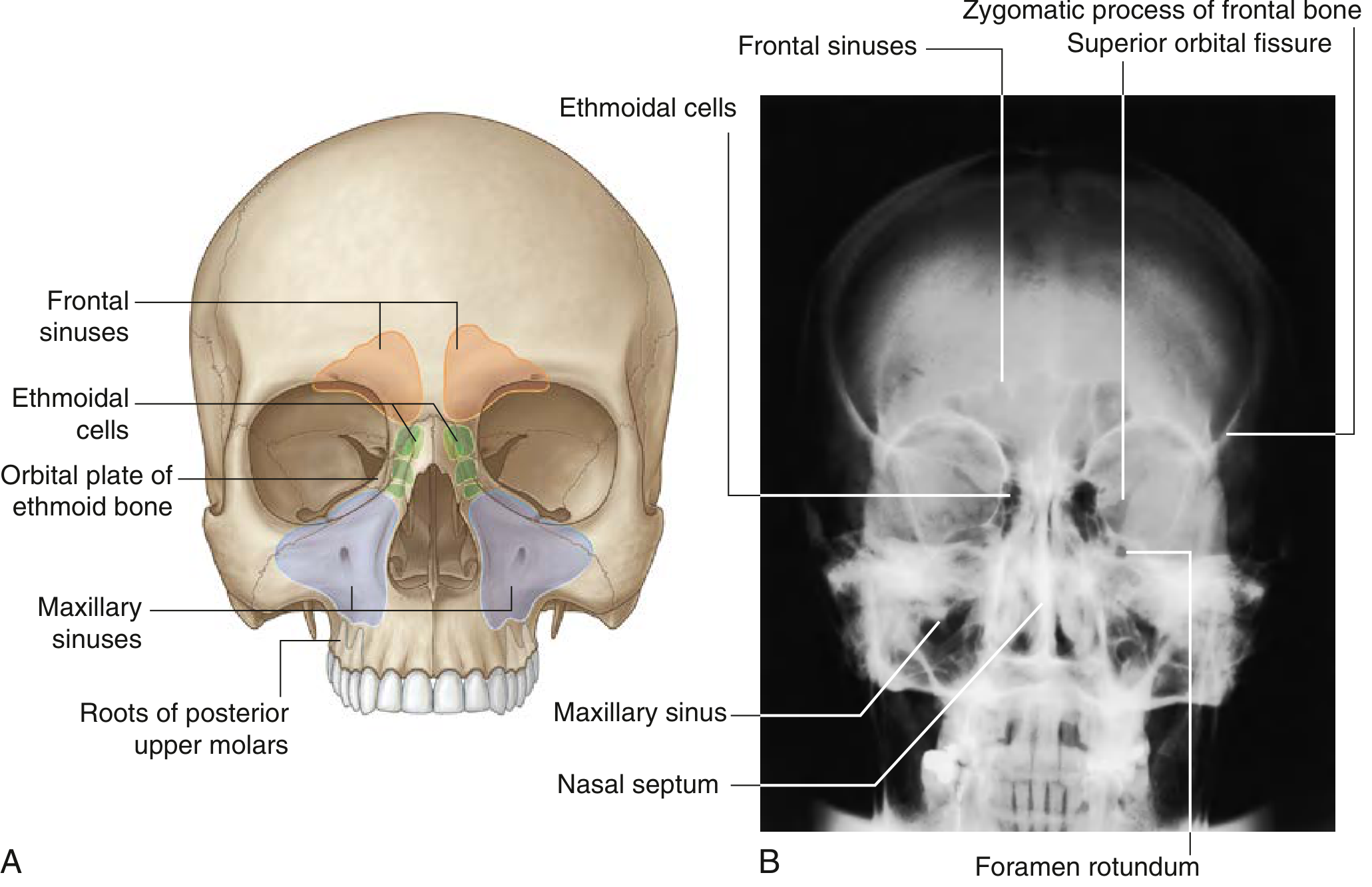
Fig. 8.238 Paranasal Sinuses - (A) Anterior view showing all four groups. (B) Posteroanterior skull radiograph. - Gray's Anatomy for Students
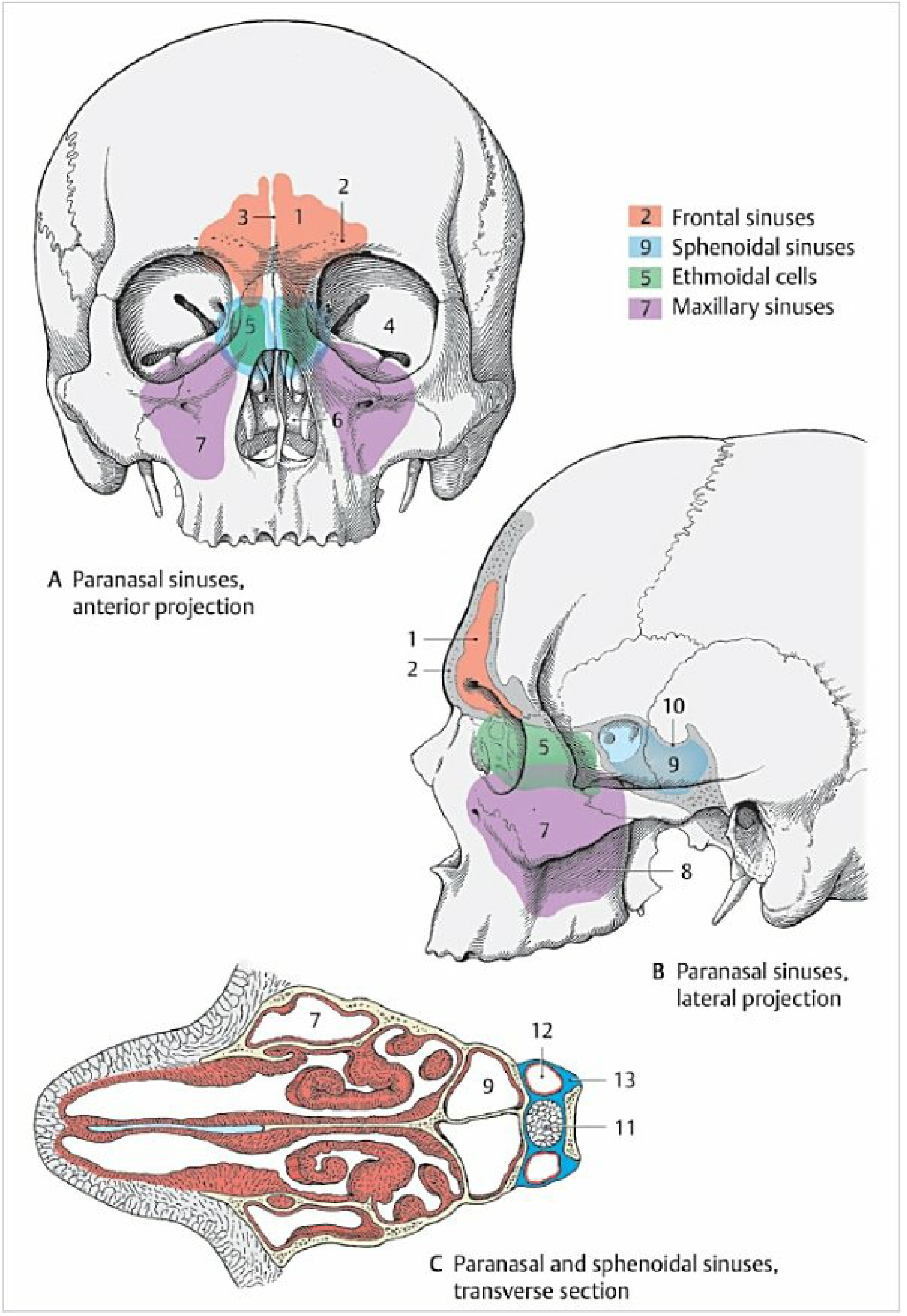
Fig. 3.5 Paranasal sinuses - anterior projection, lateral projection, and transverse section. Orange = frontal, green = ethmoidal, purple = maxillary, blue = sphenoidal. - Color Atlas of Human Anatomy Vol. 2
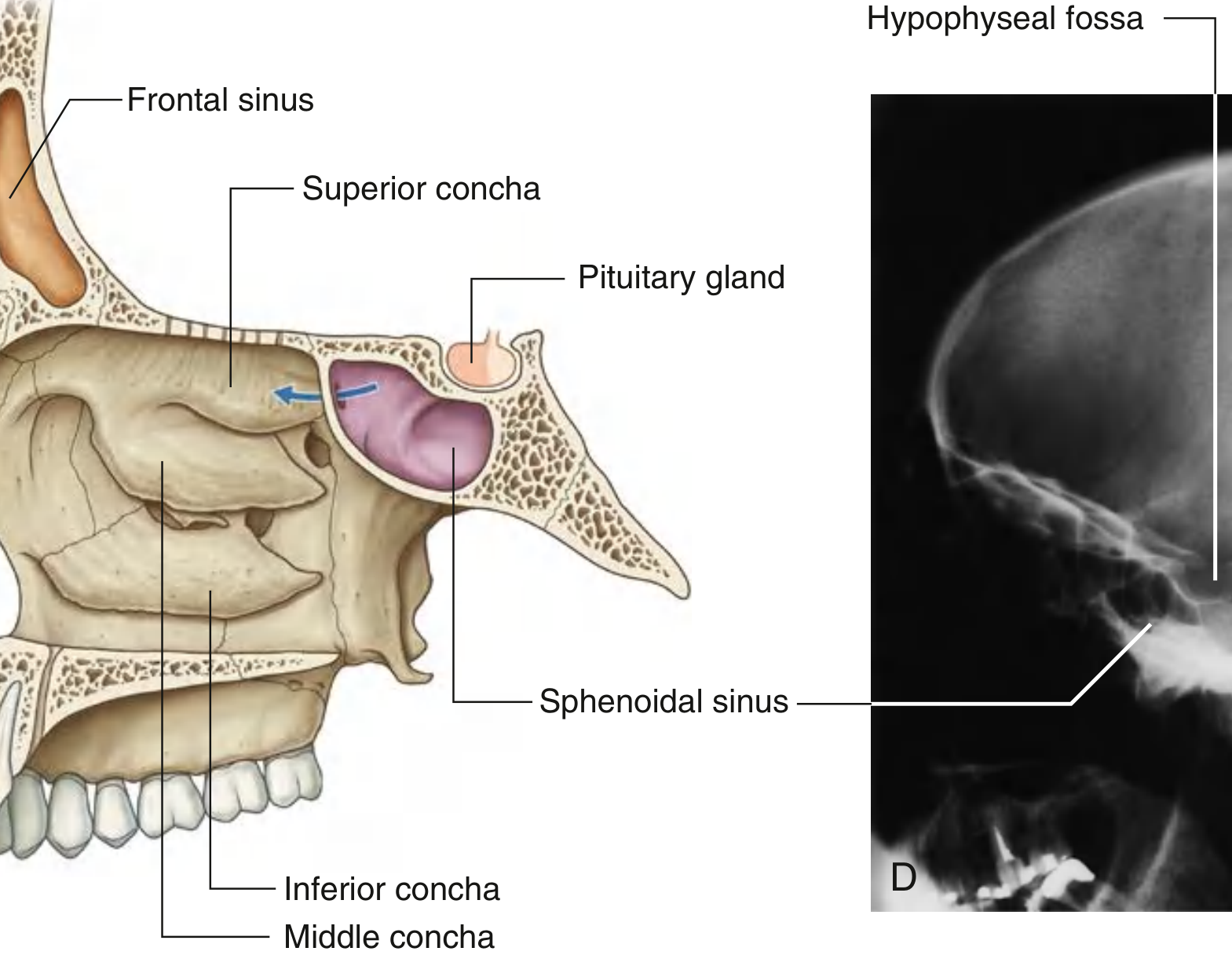
Fig. 8.238 C/D Paramedian view showing sphenoidal sinus and pituitary gland relationship. - Gray's Anatomy for Students
Common Features of All Paranasal Sinuses
All paranasal sinuses share three properties:
- Lined by respiratory mucosa - ciliated and mucus-secreting
- Open into the nasal cavities via ostia
- Innervated by branches of the trigeminal nerve [CN V]
They develop as outgrowths (diverticula) from the walls of the nasal cavities and erode into the surrounding bones, with the original openings persisting as the adult ostia.
Size Order (Largest to Smallest)
- Maxillary sinus
- Frontal sinus
- Sphenoid sinus
- Ethmoid sinus (cells)
(KJ Lee's Essential Otolaryngology)
1. Maxillary Sinuses
- Location: Largest sinuses; completely fill the bodies of the maxillae
- Shape: Pyramidal - apex directed laterally, base forming the medial wall (adjacent to nasal cavity)
- Opening: Near the top of the base, into the center of the semilunar hiatus in the middle nasal meatus (an unfavorably high position that impedes drainage when supine)
- Relationships:
- Roof (superolateral surface): Related to the orbit above
- Anterolateral surface: Related to roots of upper molar and premolar teeth, and the face anteriorly
- Posterior wall: Related to the infratemporal fossa
- Nerve supply: Infraorbital and alveolar branches of the maxillary nerve [V2]
- Blood supply: Branches of the infraorbital and superior alveolar branches of the maxillary arteries
2. Frontal Sinuses
- Location: Most superior sinuses; one on each side in the frontal bone under the forehead
- Shape: Triangular - base oriented vertically at the midline above the bridge of the nose, apex directed laterally about one-third of the way along the upper margin of the orbit
- Variable in size; can be asymmetric or absent
- Opening: Drains onto the lateral wall of the middle meatus via the frontonasal duct, which penetrates the ethmoidal labyrinth and continues as the ethmoidal infundibulum at the front end of the semilunar hiatus
- Nerve supply: Branches of the supraorbital nerve (from ophthalmic nerve [V1])
- Blood supply: Branches of the anterior ethmoidal arteries
3. Ethmoidal Cells (Ethmoid Sinuses)
- Location: Fill the ethmoidal labyrinth on each side, between the orbit laterally and the nasal cavity medially
- Structure: Not a single cavity - a variable number of individual air chambers (cells)
- Separated from the orbit by the thin orbital plate (lamina papyracea) of the ethmoid bone
- Three groups based on drainage location:
- Anterior ethmoidal cells - open into the ethmoidal infundibulum or frontonasal duct (middle meatus)
- Middle ethmoidal cells - open onto the ethmoidal bulla or the lateral wall above it (clinically grouped with anterior cells)
- Posterior ethmoidal cells - open into the superior nasal meatus
- Walls may be completed by adjacent bones (frontal, maxillary, lacrimal, sphenoid, palatine)
- Nerve supply: Anterior and posterior ethmoidal branches of the nasociliary nerve [V1], plus maxillary nerve [V2] via orbital branches from the pterygopalatine ganglion
- Blood supply: Anterior and posterior ethmoidal arteries
- Notable cell - Agger nasi: The most anterior ethmoidal cell; projects anterior to the axilla of the middle turbinate, forming a bulge in the lateral nasal wall. Its posterior limit forms the anterior border of the frontal recess.
4. Sphenoidal Sinuses
- Location: Paired, within the body of the sphenoid bone
- Opening: Via apertures high on their anterior walls, into the sphenoethmoidal recess (posterior roof of nasal cavity)
- Relationships: Clinically the most dangerous - closely related to:
- Above: Cranial cavity, pituitary gland, optic chiasm
- Laterally: Cavernous sinuses, internal carotid arteries
- Below and in front: Nasal cavities
- Nerve supply: Posterior ethmoidal branch of ophthalmic nerve [V1]; maxillary nerve [V2] via pterygopalatine ganglion
- Blood supply: Branches of the pharyngeal arteries from the maxillary arteries
Clinical point - Transsphenoidal approach to the pituitary: Because only thin shelves of bone separate the sphenoidal sinuses from the nasal cavities below and hypophyseal fossa above, the pituitary gland is surgically approached through the nasal roof → anteroinferior sphenoid bone → sphenoidal sinus → top of sphenoid → hypophyseal fossa. - Gray's Anatomy for Students, p. 1215
Drainage Summary (Ostia)
| Sinus | Drainage site |
|---|---|
| Frontal | Middle meatus (via frontonasal duct → ethmoidal infundibulum) |
| Anterior ethmoidal cells | Middle meatus (ethmoidal infundibulum) |
| Middle ethmoidal cells | Middle meatus (onto/above ethmoidal bulla) |
| Maxillary | Middle meatus (semilunar hiatus) |
| Posterior ethmoidal cells | Superior meatus |
| Sphenoidal | Sphenoethmoidal recess |
Development and Embryology
Paranasal sinuses develop as diverticula (outgrowths) from the walls of the nasal cavities and become pneumatic extensions into adjacent bones. Their original openings persist as the adult ostia.
Order of development (in utero to postnatal):
| Sinus | Development |
|---|---|
| Ethmoid | First to develop in utero; most developed at birth (all cells present, not full size). Anterior ethmoid from middle meatus; posterior from superior meatus. |
| Maxillary | Present (small) at birth; grows slowly until puberty; fully developed after all permanent teeth erupt in early adulthood. |
| Sphenoid | Absent at birth; pneumatization begins at ~1 year, when posterior ethmoidal cells grow into the sphenoid. Adult size reached by age 12. |
| Frontal | Last to begin and complete development. Absent at birth; forms at ~2 years when the two most anterior ethmoidal cells grow into the frontal bone. Visible on X-ray by age 7. Pneumatization continues into early adulthood. |
Only ethmoid and maxillary sinuses are present at birth.
Growth of the paranasal sinuses is important in:
- Altering the size and shape of the face during infancy and childhood
- Adding resonance to the voice during adolescence
(The Developing Human - Clinically Oriented Embryology, p. 529-530)
Functions (Proposed)
The physiological role of the paranasal sinuses remains uncertain, but proposed functions include:
- Vocal resonance
- Reduction of skull weight (pneumatization)
- Humidification and air conditioning of inspired air
- Heat insulation for the brain
- Physical buffer against facial injury
- Nitric oxide (NO) production - the respiratory epithelium contains large amounts of nitric oxide synthase; NO produced in the sinuses plays a role in ciliary beat frequency and host defense
(Scott-Brown's Otorhinolaryngology; Histology: A Text and Atlas)
Clinical Relevance
-
Sinusitis: Infections of the nasal mucosa can spread through the sinus ostia. Poorer circulation and unfavorably placed openings (e.g., the maxillary ostium near the roof of the sinus) impair drainage and promote chronic inflammation.
-
Orbital complications: Inflammation of the ethmoidal cells can spread to the orbit by penetrating the thin orbital plate (lamina papyracea) of the ethmoid bone.
-
Sphenoidal sinus surgery: Surgical access to the pituitary gland uses a transsphenoidal approach through the sinus.
-
Dental sinusitis: The close relationship of maxillary sinus floor to roots of upper molars/premolars means dental infections can cause maxillary sinusitis (and vice versa).
-
Frontal sinus absent: The frontal sinus may be absent entirely - a normal variant of no clinical significance.
(Color Atlas of Human Anatomy Vol. 2, p. 182; Gray's Anatomy for Students, p. 1215; Cummings Otolaryngology)
This is a shared conversation. Sign in to Orris to start your own chat.