Case Study: on pre-operative airway assessment before ENT surgery.
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching PubMed
preoperative airway assessment ENT surgery difficult intubation
I now have rich, textbook-sourced content from Miller's Anesthesia, Morgan & Mikhail, Barash, Scott-Brown's, and Cummings. I have enough to write a thorough, clinically grounded case study. Let me compose it now.
Case Study: Pre-operative Airway Assessment Before ENT Surgery
Patient Presentation
Patient: Mr. Ahmed K., 58-year-old male
Presenting complaint: Progressive hoarseness for 4 months, occasional dysphagia, and exertional stridor
Planned procedure: Direct laryngoscopy + biopsy of a suspected supraglottic laryngeal mass (ENT surgery under general anaesthesia)
PMH: Type 2 diabetes mellitus (BMI 36 kg/m²), obstructive sleep apnoea (OSA) on CPAP, previous radiotherapy to the neck 5 years ago for an unrelated nodal mass, hypertension
Medications: Metformin, ramipril, CPAP nightly
Why Airway Assessment Is Especially Critical in ENT Surgery
Difficult airways are encountered far more frequently in patients undergoing ENT surgery than in the general surgical population. In a series of 1,200 consecutive ENT and general surgical patients, the overall prevalence of difficult intubation (defined as requiring specialist equipment) was 4.2% - but this rose to 12.3% in ENT cancer surgery, compared with only 2.0% in general surgical patients. This confirms the clinical impression that difficult intubation is significantly more common in head and neck cases, particularly in those following extensive surgery, flap reconstruction, post-operative radiotherapy, or with an obstructed airway. (Scott-Brown's Otorhinolaryngology, Vol. 1)
The Fourth National Airway Project (NAP4), run by the Royal College of Anaesthetists and auditing over 3 million anaesthetics, reported an incidence of adverse airway events of 1:22,000 and death related to an airway event of 1:180,000 - placing airway management failure among the most preventable causes of anaesthetic mortality.
Step 1: History - The First Layer of Airway Assessment
A thorough history often provides the most important clues before the patient ever opens their mouth.
Key questions to ask:
| Domain | Relevance in this patient |
|---|---|
| Previous anaesthetic records | Any prior difficult intubation, dental trauma, prolonged sore throat, or unplanned ITU stay after a previous anaesthetic signals a potentially difficult airway |
| Head and neck surgery/radiotherapy | This patient has prior neck radiotherapy - this causes fibrosis, reduced tissue compliance, restricted mouth opening (trismus), and altered anatomy |
| Current pathology | Supraglottic mass with hoarseness and stridor - highly concerning for partial airway obstruction |
| OSA | Predicts redundant pharyngeal tissue, increased neck circumference, difficult mask ventilation |
| Diabetes + obesity (BMI 36) | Increased neck adipose tissue; "stiff joint syndrome" in diabetics can restrict atlanto-occipital extension |
| Dysphagia | Suggests significant mass effect on the hypopharynx or oesophageal inlet |
Teaching point: Past anaesthetic records should always be reviewed. Patients may relay verbal or written warnings from a previous anaesthetist. Difficulty may also be inferred from a history of displaced front teeth, bruised lips, excessive post-operative sore throat, or an unexpected stay in ITU. (Scott-Brown's, Vol. 1)
Step 2: Physical Examination - The Bedside Battery
A pre-anaesthetic airway assessment is mandatory before every anaesthetic procedure. Multiple anatomical and functional manoeuvres estimate the difficulty of tracheal intubation. (Morgan & Mikhail's Clinical Anesthesiology, 7e)
2a. Mouth Opening
- Measure the inter-incisor gap. A distance of ≥3 cm (approximately 3 fingerbreadths) is desirable in an adult.
- Less than 3 cm suggests difficult laryngoscope blade insertion.
- In Mr. Ahmed: reduced mouth opening is possible given prior neck radiotherapy causing progressive fibrosis/trismus.
2b. Mallampati Classification
The most widely used test - it examines the size of the tongue relative to the oral cavity. The patient sits upright, opens the mouth maximally, and protrudes the tongue without phonation.
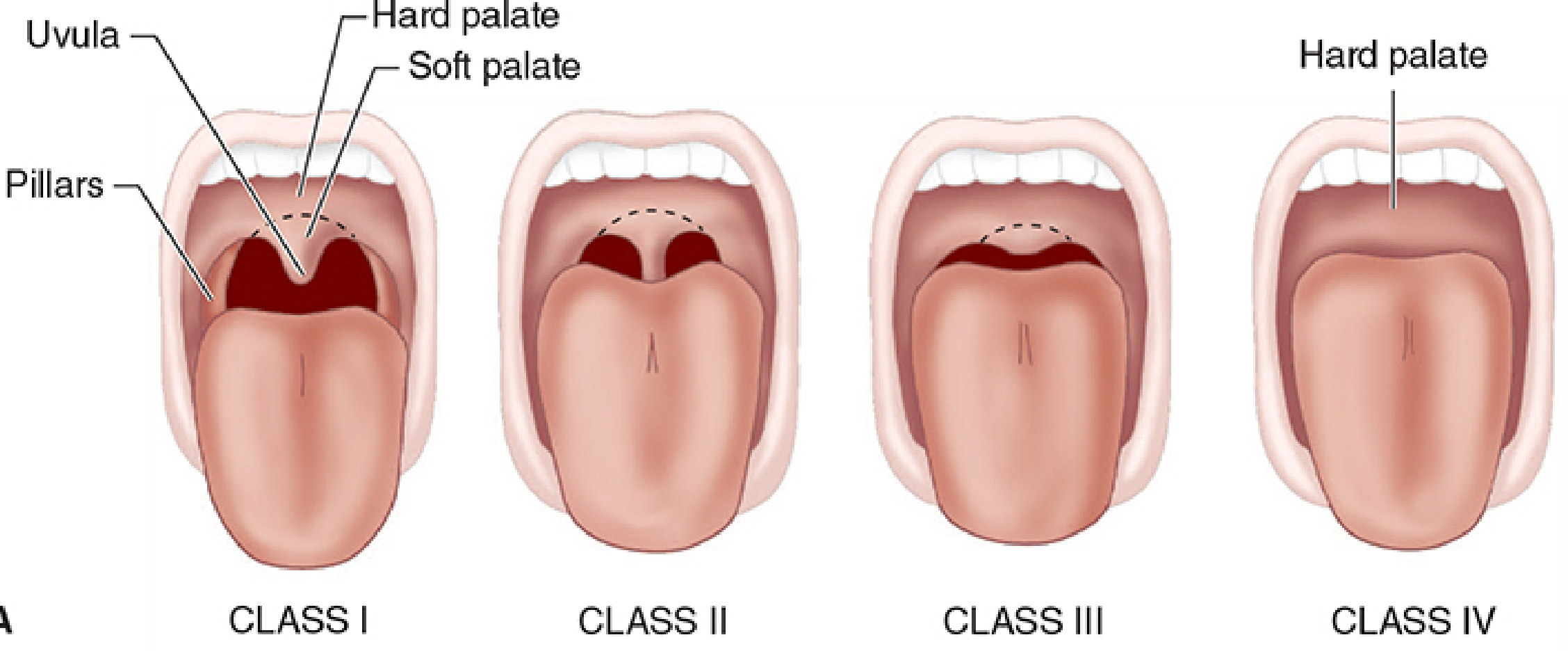
| Class | What is visible | Laryngoscopic view |
|---|---|---|
| I | Entire palatal arch, bilateral faucial pillars, uvula visible to base | Easy - Grade I/II |
| II | Upper faucial pillars and most of uvula visible | Usually easy |
| III | Only soft and hard palates visible | Likely difficult - Grade III |
| IV | Only hard palate visible | Very difficult - Grade IV |
- Class III or IV predicts a difficult intubation (Grade III/IV laryngoscopic view). (Morgan & Mikhail's)
- Note: Although the presence of these findings is not highly sensitive alone, the absence of all these findings is reassuring. Any patient's airway may prove surprisingly difficult despite a normal bedside assessment. (Morgan & Mikhail's)
2c. Thyromental Distance (TMD)
The distance between the mentum (chin) and the superior thyroid notch with the neck in full extension.
- Desirable: ≥3 fingerbreadths (approximately 6-8 cm).
- A short TMD reflects reduced neck mobility, retrognathia, and predicts difficult tongue displacement during laryngoscopy.
- In this patient with prior neck radiotherapy, TMD may be reduced.
2d. Neck Circumference
A neck circumference of >17 inches (43 cm) is associated with difficulties in glottic visualisation - relevant given this patient's BMI of 36. (Morgan & Mikhail's)
2e. Upper Lip Bite Test (ULBT)
The patient is asked to bite their upper lip with their lower incisors:
- Class I: Lower incisors bite above the vermilion border of the upper lip - easy intubation likely
- Class II: Lower incisors bite below the vermilion border - moderately difficult
- Class III: Lower incisors cannot bite the upper lip at all - difficult intubation predicted
2f. Neck Mobility / Atlanto-occipital Extension
Full neck extension is needed to align the oral, pharyngeal, and laryngeal axes for direct laryngoscopy.
- Previous radiotherapy and diabetes both reduce this.
- Assess by asking the patient to maximally extend the neck and estimating the angle of excursion.
2g. Dentition
- Prominent central incisors obstruct the laryngoscopic view.
- Poor or restored dentition increases risk of dental trauma.
- Edentulous patients are harder to mask-ventilate. (Barash's Clinical Anesthesia, 9e)
Summary Physical Examination Table
(Adapted from Barash's Clinical Anesthesia, 9e - Table 28-2)
| Feature | Finding in Mr. Ahmed | Implication |
|---|---|---|
| Mouth opening | Likely reduced (prior XRT) | Difficult blade insertion |
| Jaw protrusion (ULBT) | May be impaired | Difficult tongue displacement |
| Mallampati | Likely III-IV (supraglottic mass) | Difficult laryngoscopy predicted |
| Thyromental distance | Possibly reduced | Retrognathia / reduced neck mobility |
| Neck circumference | Increased (BMI 36, OSA) | Difficult mask ventilation and laryngoscopy |
| Airway pathology | Supraglottic mass + stridor | Friable tissue, absent/altered landmarks |
| Neck mobility | Reduced (prior XRT + fibrosis) | Difficult axis alignment |
Step 3: Imaging and Indirect Laryngoscopy
For patients with a suspected difficult airway - especially those with head and neck pathology - pre-operative imaging review and indirect laryngoscopy are essential additions to the bedside examination.
-
CT scan of the neck/larynx: Defines the size, location, and degree of luminal narrowing caused by the mass. Reviews whether the mass is supraglottic, glottic, or subglottic, and whether there is tracheal deviation or subglottic extension."Reviewing the results of a preoperative computed tomography (CT) scan or an indirect laryngoscopy in selected patients can be particularly helpful." (Miller's Anesthesia, 10e)
-
Indirect/flexible laryngoscopy (nasendoscopy): Often performed by the ENT surgeon in clinic pre-operatively. Directly visualises the mass, vocal cord mobility, and the degree of supraglottic obstruction. This is arguably the most important single investigation before proceeding to intubation.
-
Nasendoscopy findings in Mr. Ahmed: A 2 cm supraglottic mass on the right aryepiglottic fold with partial vocal cord fixation and approximately 50% reduction in glottic lumen on inspiration.
This has major implications for anaesthetic planning - the patient has a partially obstructed airway and vocal cord immobility.
Step 4: Recognising Conditions with Heightened Risk
Barash's Clinical Anesthesia (Table 28-3) lists conditions that substantially increase risk of difficult laryngoscopy, mask ventilation, or supraglottic airway (SGA) placement:
- History of failed or traumatic airway management
- History of head/neck surgery or radiation therapy ✓
- Supraglottic pathology: airway cyst or tumour ✓
- Stridor ✓
- Obstructive sleep apnoea ✓
- BMI >35 ✓
- Cervical spine disease or limited range of motion ✓
- Temporomandibular joint disease
Mr. Ahmed meets six of these criteria simultaneously - this is a very high-risk airway.
Step 5: Anaesthetic Decision - Awake Intubation vs Intubation After Induction
This is the most consequential decision flowing from the pre-operative assessment.
From the ASA Difficult Airway Algorithm (reproduced in Morgan & Mikhail's Clinical Anesthesiology, 7e), the clinician must consider:
- The likelihood and clinical impact of basic management problems (difficult mask ventilation, difficult SGA placement, difficult laryngoscopy, difficult intubation, difficult surgical airway)
- The feasibility of awake intubation vs intubation after induction of general anaesthesia
- Non-invasive vs invasive techniques
- Preservation vs ablation of spontaneous ventilation
- Video-assisted laryngoscopy as an initial approach
"Awake intubation vs. intubation after induction of general anesthesia" is a core decision node in the ASA algorithm. (Morgan & Mikhail's, 7e)
In Mr. Ahmed's case:
Awake Tracheal Intubation (ATI) using a flexible bronchoscope/videolaryngoscope is the correct first choice because:
- A supraglottic mass with stridor and partial vocal cord fixation means that induction of general anaesthesia may cause complete airway obstruction - loss of spontaneous ventilation removes the safety net.
- ATI with a flexible bronchoscope is well-tolerated, gentle on the airway, and does not require force to obtain glottic exposure. (Miller's Anesthesia, 10e)
- The patient can be topicalised and sedated with dexmedetomidine or low-dose remifentanil while maintaining spontaneous breathing.
"Endotracheal intubation in an awake patient (awake tracheal intubation [ATI]) with a flexible bronchoscope is commonly used when intubation following induction of general anesthesia is predicted to be difficult or impossible." (Miller's Anesthesia, 10e)
"When an airway disorder is so extensive that awake endotracheal intubation is too risky or impractical, tracheostomy performed using local anesthesia (with or without judicious intravenous sedation) is usually the best alternative." (Miller's Anesthesia, 10e)
Step 6: Planning for Equipment and Contingencies
Before bringing Mr. Ahmed to the operating theatre, the anaesthetist must have a primary plan, a backup plan, and an emergency plan (the "Plan A / Plan B / Plan C / Plan D" framework from the Difficult Airway Society guidelines):
| Plan | Technique | Rationale |
|---|---|---|
| Plan A | Awake flexible bronchoscopic intubation with topical anaesthesia and judicious sedation | Gold standard for anticipated difficult airway with mass/obstruction |
| Plan B | Awake videolaryngoscopy (e.g. GlideScope) if bronchoscope fails | Alternative non-invasive technique |
| Plan C | SGA insertion for oxygenation (if Plans A/B fail) | Temporary bridge - likely difficult given supraglottic mass |
| Plan D (Emergency) | Front-of-neck access (surgical cricothyrotomy or tracheostomy under LA) | "Can't intubate, can't oxygenate" scenario |
Various specialty organisations produce algorithms that discourage repeated performance of the same failed technique to secure the airway. Rather, they suggest continually attempting new approaches and proceeding to front-of-neck airway access once a "can't intubate, can't oxygenate" event is recognised. (Morgan & Mikhail's, 7e)
ENT-Specific Tube Considerations (Miller's Anesthesia, 10e):
- A microlaryngeal tube (MLT) will be used - smaller diameter allows better surgical access to the larynx.
- If a laser is involved: a laser-safe ETT must be selected matched to the laser type; cuff can be filled with saline dyed with methylene blue to detect cuff leaks immediately.
- Wire-reinforced (armoured) tubes prevent kinking during head manipulation in ENT procedures.
- Cuff pressure must be kept <25 mm Hg to prevent ischaemic tracheal mucosal damage - especially important in long cases.
- If nitrous oxide is used, diffusion into the cuff will gradually increase cuff pressure and requires monitoring.
Communication with the Surgeon:
Open communication between surgeon and anaesthesiologist is critical - particularly regarding:
- Whether bronchoscopy is planned pre- or post-intubation
- How the tube will be secured during head manipulation
- Whether neuromuscular blocking drugs can be used (facial nerve monitoring during some ENT procedures precludes their extended use)
- Whether tracheostomy under LA needs to be planned as a primary strategy
Step 7: Special Considerations in This Case
Post-Radiotherapy Airway
Prior radiotherapy to the head and neck causes progressive fibrosis that makes the airway increasingly difficult over time. Changes include:
- Restricted mouth opening (trismus)
- Reduced neck mobility
- Friable mucosa prone to bleeding and oedema
- Distorted anatomy with absent landmarks
- Reduced tissue compliance making mask ventilation difficult
Obesity and OSA
- Both predict difficult mask ventilation.
- Morbidly obese patients (BMI ≥35) may have redundant pharyngeal tissue and increased neck circumference.
- Not only may these patients prove difficult to intubate - routine bag-mask ventilation may also be problematic. (Morgan & Mikhail's, 7e)
- Pre-oxygenation in the 20-30° head-up (ramped) position significantly extends safe apnoea time.
Stridor
Stridor represents airway narrowing of ≥50% of the lumen and is a red flag requiring urgent pre-operative assessment. Causes include:
- Inhaled foreign bodies
- Bilateral vocal cord palsy
- Airway oedema / angioedema
- Epiglottitis
- Subglottic stenosis
- Airway tumours (as in this patient)
"Regardless of the aetiology, the initial assessment should focus on whether endotracheal intubation or a surgical approach to the airway is immediately necessary to rescue the patient from death or injury." (Miller's Anesthesia, 10e)For patients with stridor but satisfactory gas exchange, a helium:oxygen (heliox) blend via non-rebreathing mask or high-flow nasal oxygen can improve airflow temporarily while assessing and managing the cause. (Miller's Anesthesia, 10e)
Step 8: Documentation and Handover
After securing the airway, the anaesthetist must:
- Document the difficulty encountered in the medical record and add it to the problem list.
- Use a structured tool such as the Intubation Difficulty Scale (IDS) (Adnet et al.) which scores: number of supplementary attempts, additional operators, alternative techniques used, laryngoscopic grade, subjective lifting force, use of external laryngeal manipulation, and vocal cord characteristics. (Miller's Anesthesia, 10e)
- Provide the patient with a written difficult airway alert card.
- Ensure the anaesthetic record flags this for any future procedures.
Summary: The LEMON Mnemonic for Pre-operative Airway Screening in ENT
| Letter | Criterion | Finding in Mr. Ahmed |
|---|---|---|
| L - Look externally | Obvious facial/neck abnormality, stridor, neck mass, obesity | Neck fibrosis, large BMI, stridor - ABNORMAL |
| E - Evaluate 3-3-2 rule | Mouth opening ≥3F, hyoid-to-chin ≥3F, thyroid notch-to-floor of mouth ≥2F | Likely reduced across all three - ABNORMAL |
| M - Mallampati | Oropharyngeal visibility | Class III-IV predicted - ABNORMAL |
| O - Obstruction | Any condition causing obstruction (mass, haematoma, abscess, foreign body) | Supraglottic mass + 50% glottic stenosis - ABNORMAL |
| N - Neck mobility | Full range of motion for axis alignment | Restricted (prior XRT, diabetes) - ABNORMAL |
Mr. Ahmed scores LEMON positive across all five criteria - this is a predicted difficult airway requiring an awake intubation strategy.
Key Learning Points
-
ENT surgery carries the highest rates of difficult intubation of any surgical specialty - up to 12.3% in ENT cancer cases vs 2% in general surgery. Never underestimate the head and neck airway. (Scott-Brown's Otorhinolaryngology)
-
Pre-operative assessment must be multi-layered: history (prior anaesthetic records, XRT, current pathology) + physical exam (LEMON/bedside tools) + indirect laryngoscopy + imaging review.
-
Mallampati alone is insufficient - it is one component of a multivariable risk index. No single test is sensitive enough to exclude a difficult airway.
-
Stridor and supraglottic pathology demand awake intubation - inducing general anaesthesia before securing the airway in a patient with partial glottic obstruction risks total airway loss.
-
Always plan four steps ahead: Plan A (preferred technique), Plan B (alternative non-invasive), Plan C (SGA bridge), Plan D (front-of-neck access). Never repeat a failed technique without escalating.
-
Communication between anaesthetist and ENT surgeon is essential before the case, not during a crisis.
-
Document every difficult airway and alert the patient - the next anaesthetist will thank you.
Sources: Miller's Anesthesia 10e; Morgan & Mikhail's Clinical Anesthesiology 7e; Barash's Clinical Anesthesia 9e; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol.1; Cummings Otolaryngology Head and Neck Surgery.
This is a shared conversation. Sign in to Orris to start your own chat.