I want 10 common condition to find in ECG and with images for each condition
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the content and ECG image URLs I need for all 10 conditions. Let me compile the comprehensive answer.
Here are 10 common ECG conditions with descriptions and textbook images for each:
1. Atrial Fibrillation (AF)
Key ECG features:
- Absence of discernible P waves (flat or chaotic baseline)
- Irregularly irregular ventricular rhythm
- Narrow QRS complexes (unless aberrant conduction)
- Ventricular rate typically 120-170 beats/min (AV node unaffected)
AF occurs due to multiple small areas of atrial myocardium continuously discharging, producing chaotic atrial activity with no effective atrial contraction. Common causes include ischemic or valvular heart disease, thyrotoxicosis, and cardiomyopathy.
2. Atrial Flutter
Key ECG features:
- "Sawtooth" flutter waves (negative deflections), best seen in inferior leads (II, III, aVF) and V1
- Regular atrial rate ~300 beats/min (range 250-350)
- AV block ratio commonly 2:1, giving ventricular rate ~150 beats/min
- Narrow QRS complexes (unless bundle branch block)
Atrial flutter is a re-entrant rhythm. A regular narrow-complex tachycardia at ~150 beats/min should strongly suggest atrial flutter with 2:1 conduction.
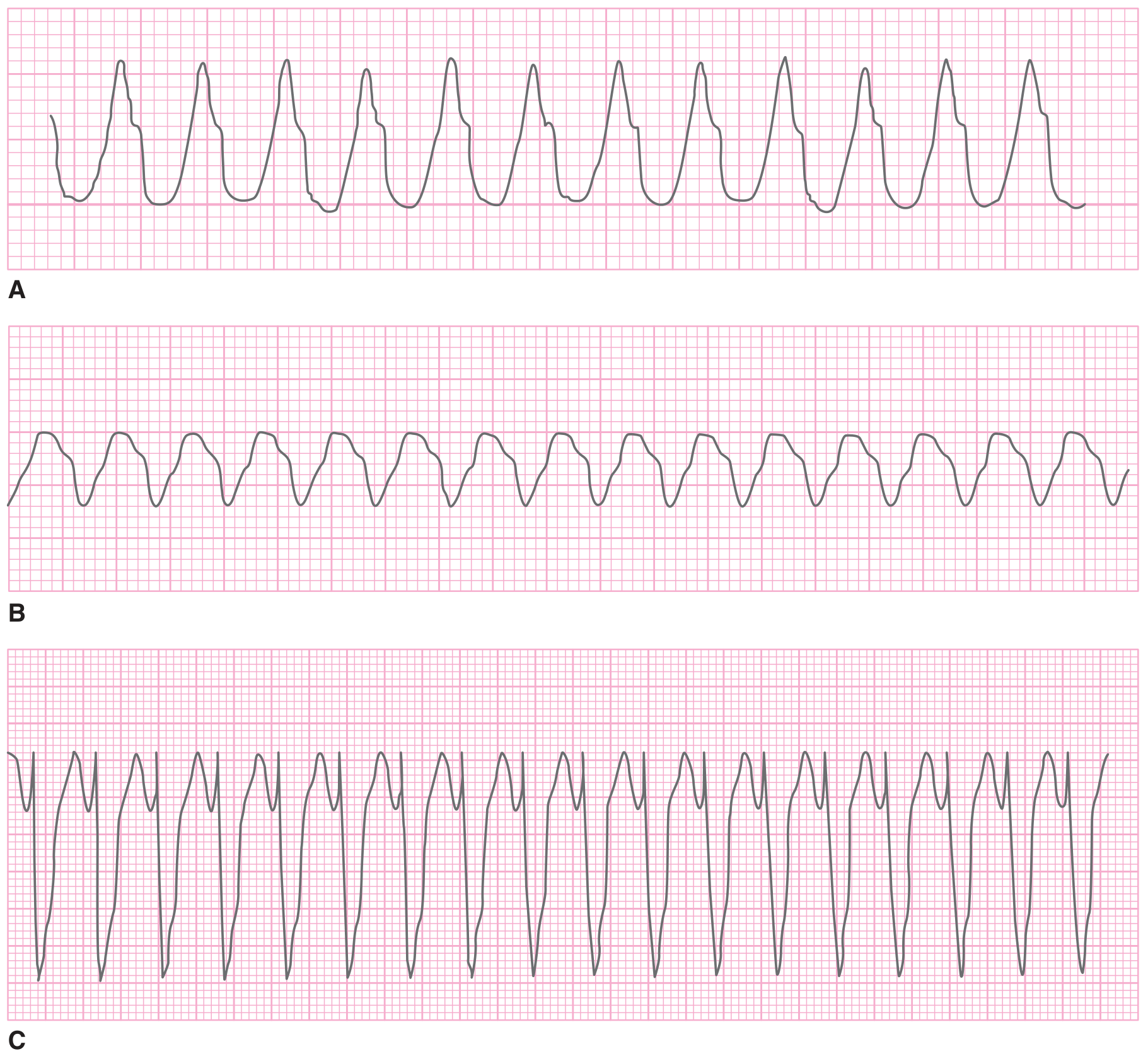
3. Ventricular Tachycardia (VT)
Key ECG features:
- Wide QRS complex (>100-120 ms)
- Rate 140-180 beats/min (range 120-300)
- No P waves associated with QRS (may see occasional dissociated P waves)
- Monomorphic: consistent beat-to-beat QRS morphology
- Polymorphic: varying QRS morphology (Torsades de Pointes is a subtype)
VT is defined as 3 or more consecutive ventricular depolarizations at >100 beats/min. Most cases are caused by chronic ischemic heart disease or acute MI. Torsades de Pointes is a polymorphic subtype seen with prolonged QT interval.
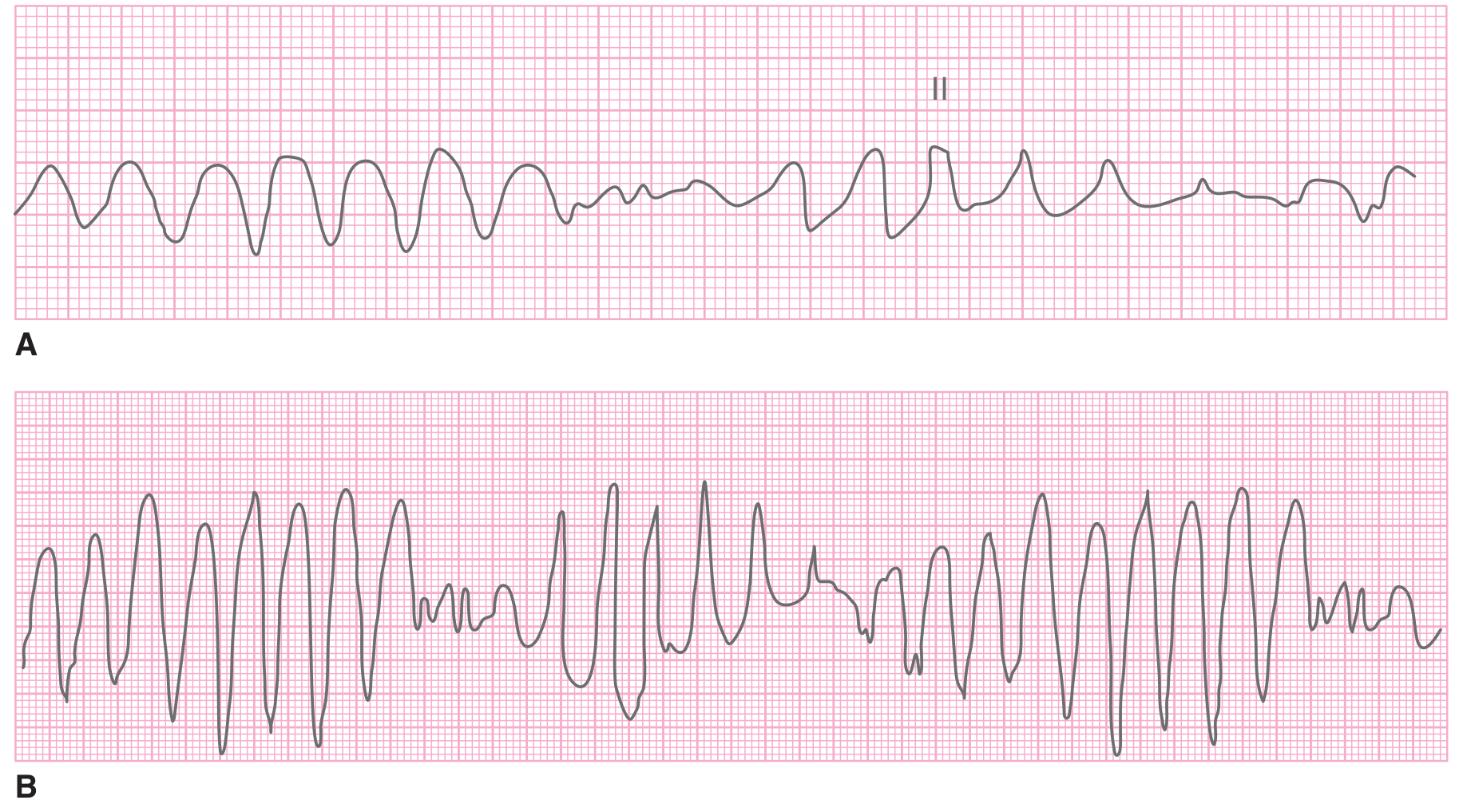
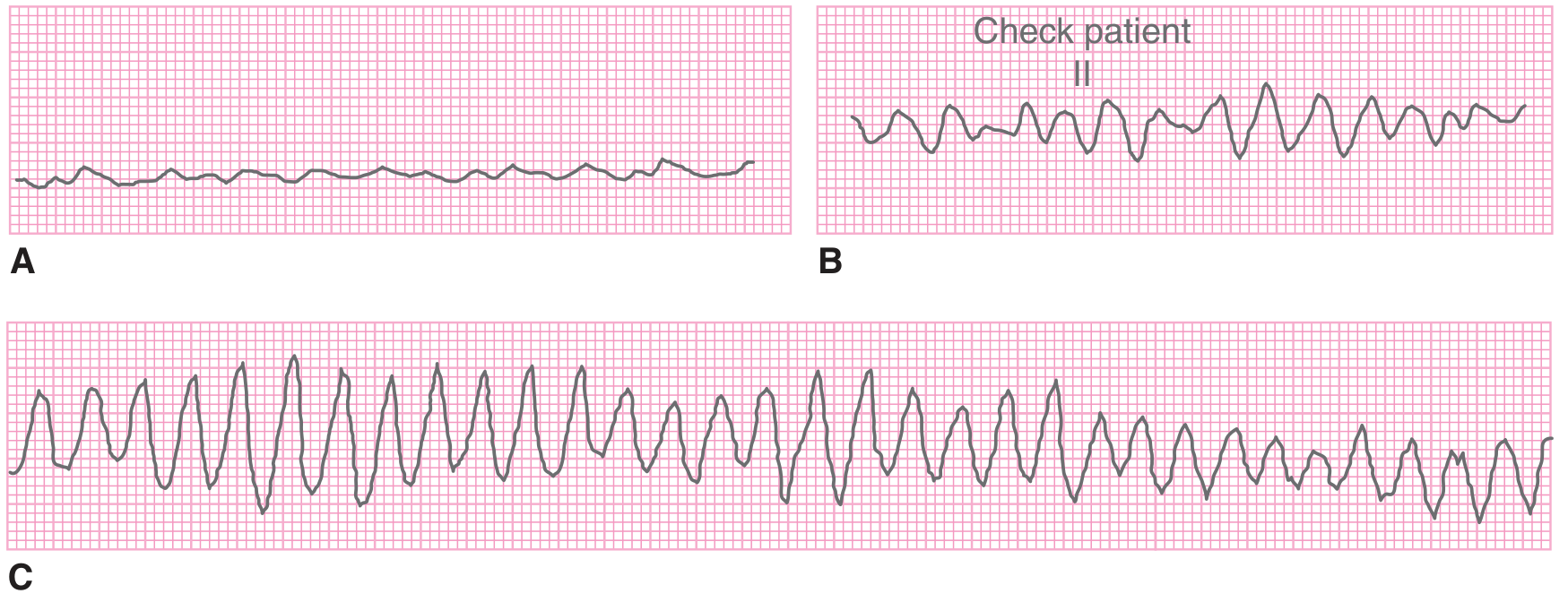
4. Ventricular Fibrillation (VF)
Key ECG features:
- Disorganized, chaotic waveform
- No discernible P waves or QRS complexes
- Irregular pattern that can be fine, intermediate, or coarse in amplitude
- No cardiac output - always a cardiac arrest rhythm
VF is disorganized depolarization of small ventricular areas with no effective mechanical activity. Most common in severe ischemic heart disease. Fine VF must be distinguished from asystole; coarse VF can mimic VT.
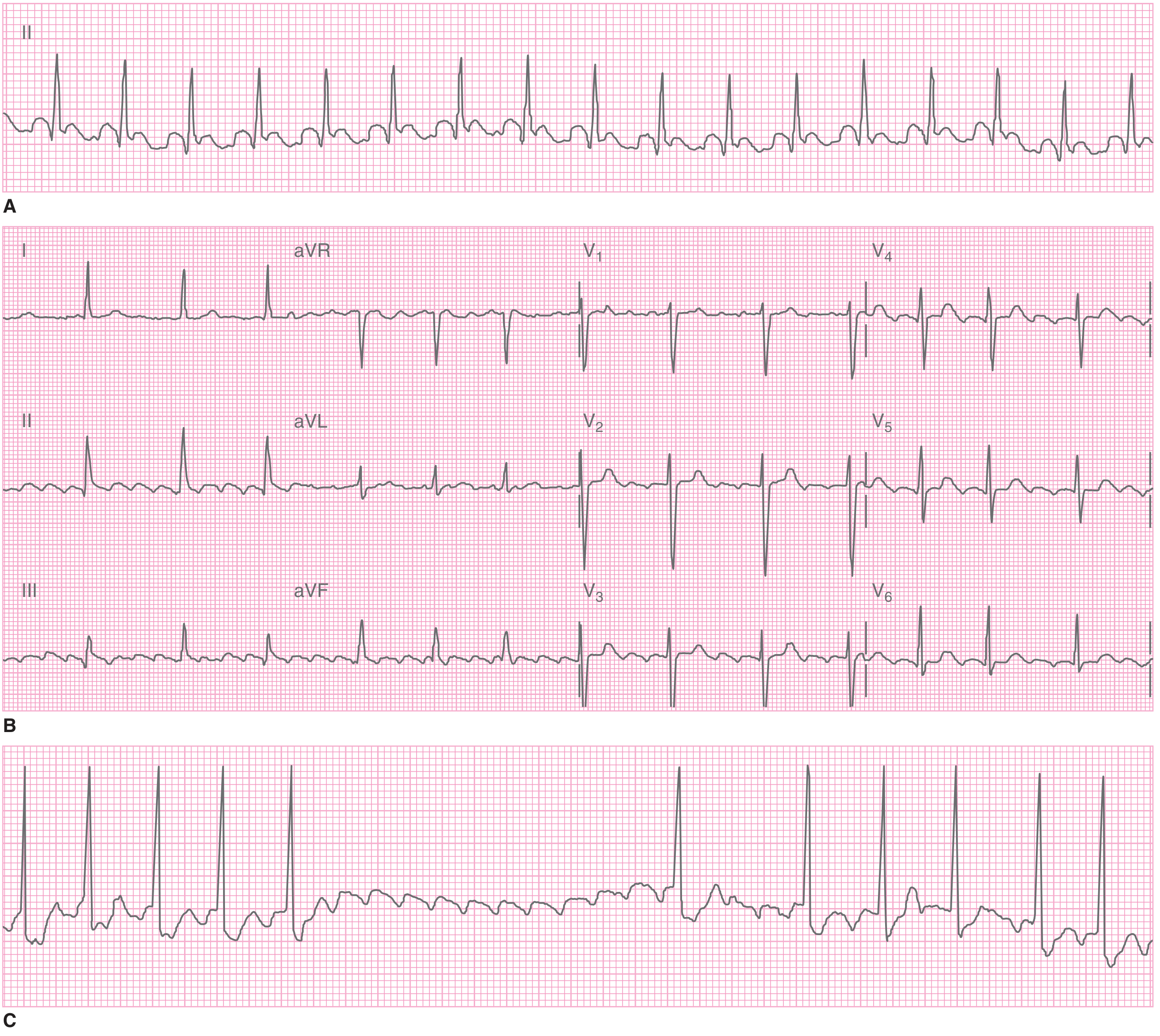
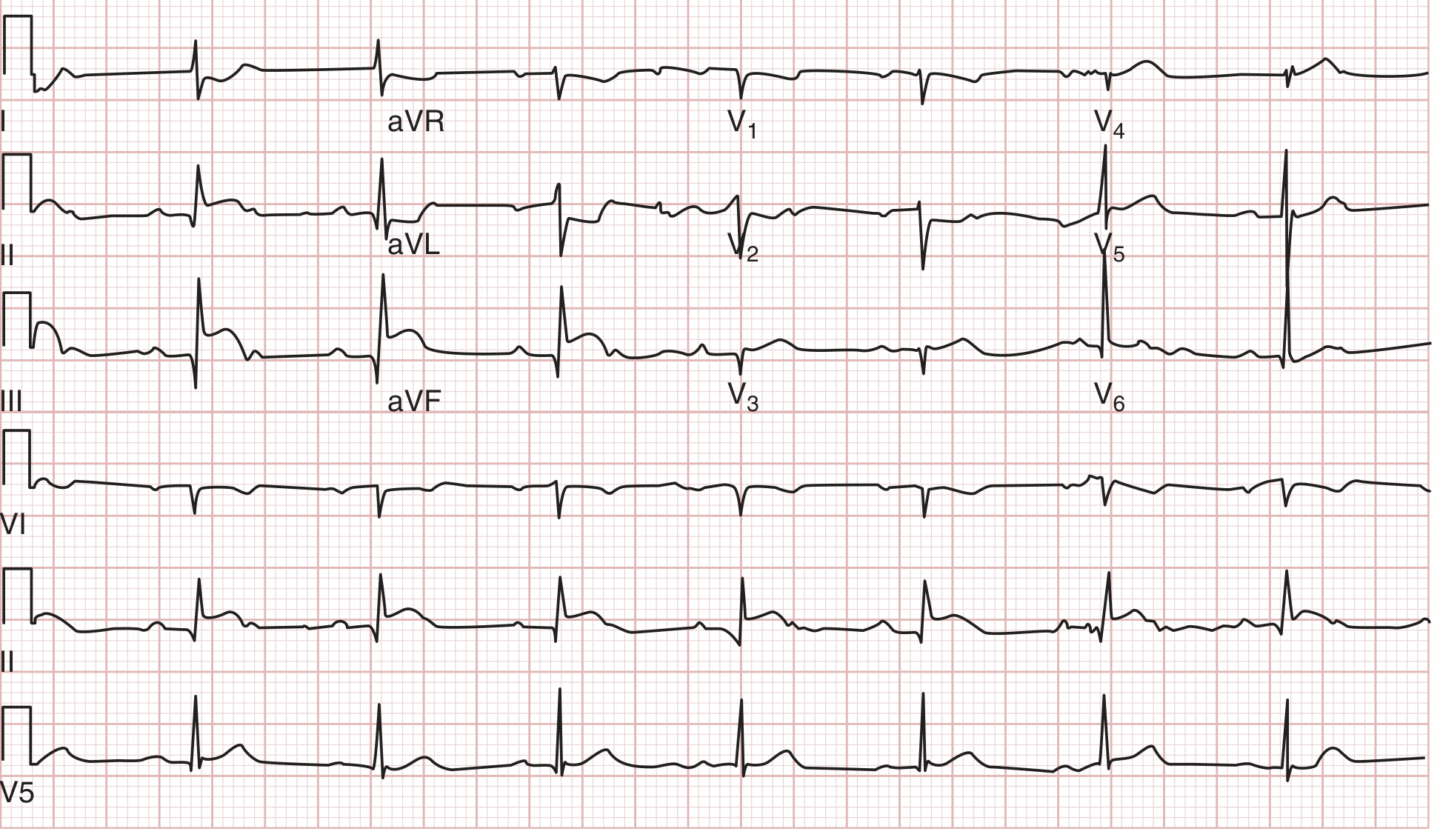
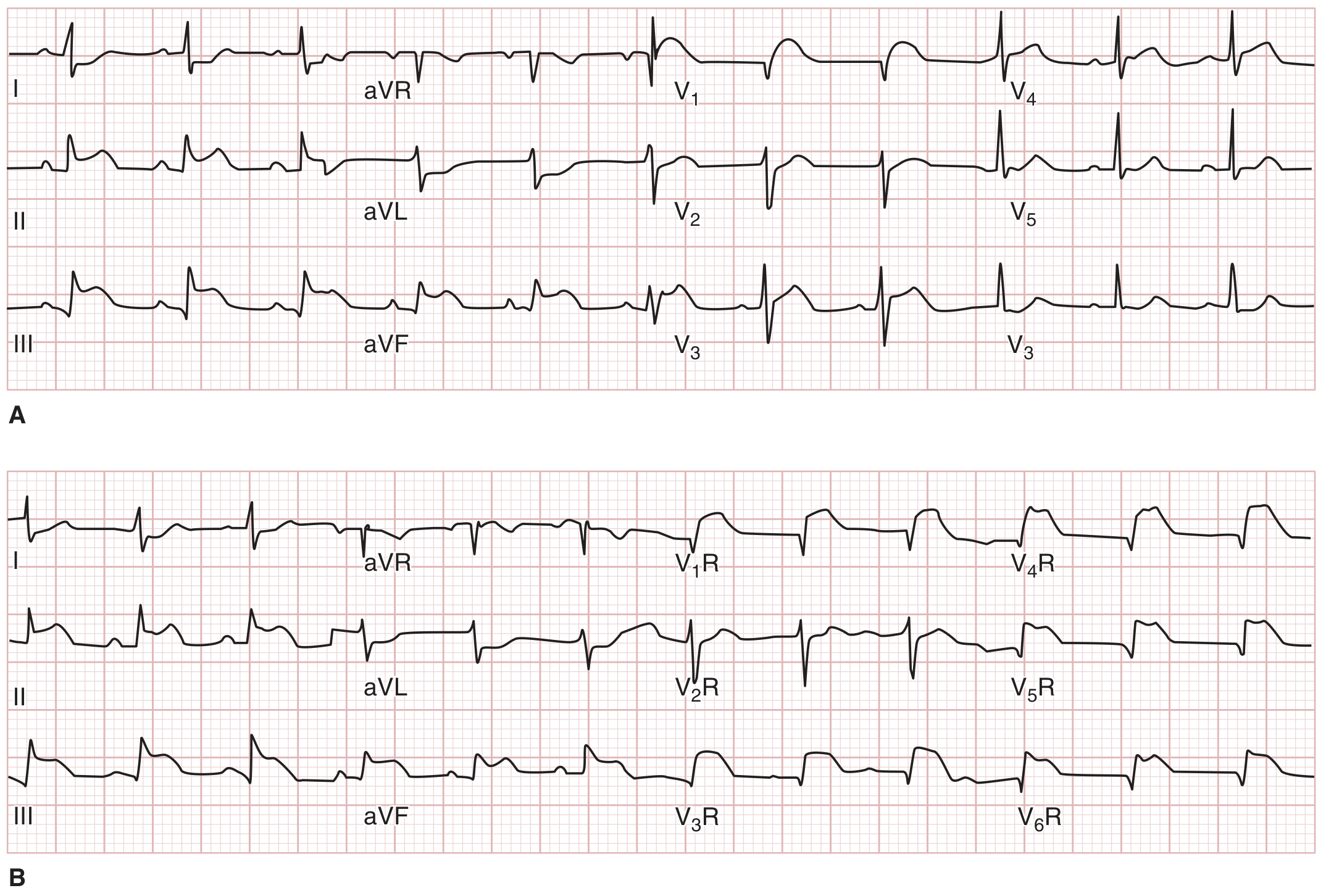
5. ST-Elevation Myocardial Infarction (STEMI)
Key ECG features:
- ST-segment elevation in regional lead groups (indicating culprit vessel territory)
- Inferior STEMI: ST elevation in II, III, aVF (usually RCA)
- Anterior STEMI: ST elevation in V1-V4 (usually LAD)
- Lateral STEMI: ST elevation in I, aVL, V5-V6
- Reciprocal ST depression in opposite leads
- Evolution: hyperacute T waves → ST elevation → Q waves → T-wave inversion
STEMI diagnosis requires ECG in the setting of ischemic symptoms. The initial 12-lead ECG should be obtained and interpreted within 10 minutes of presentation.
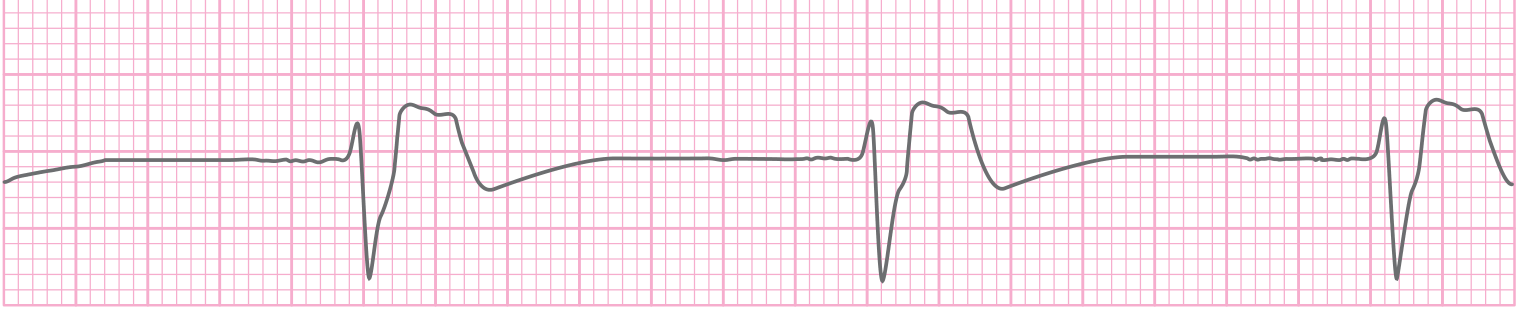
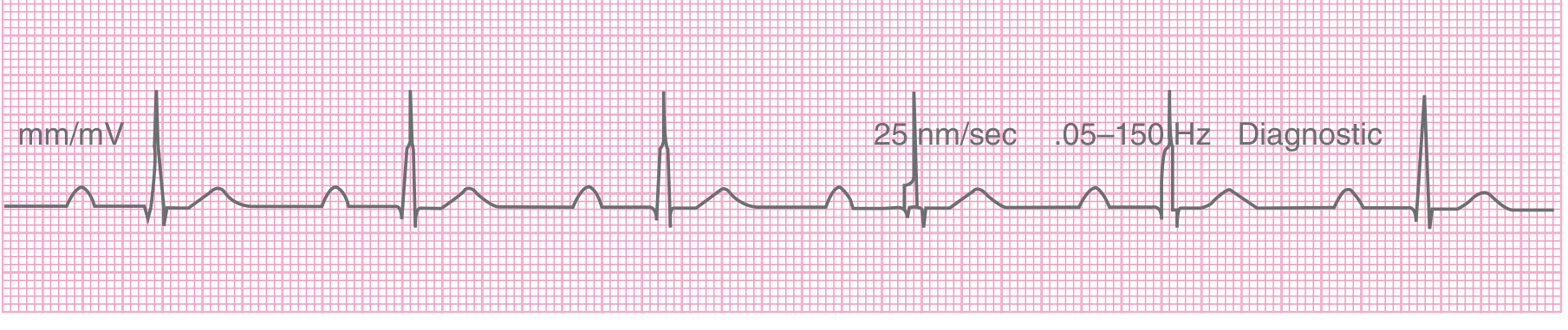
6. First-Degree AV Block
Key ECG features:
- Consistent 1:1 P wave to QRS relationship (every P conducts)
- Prolonged PR interval >200 ms (0.2 seconds)
- Normal QRS morphology
- Regular rhythm
Conduction delay occurs at the AV node. Common causes include high vagal tone, medication toxicity (digoxin, beta-blockers), inferior MI, and myocarditis. Generally benign in isolation, but in acute coronary syndromes it may herald progression to complete heart block.
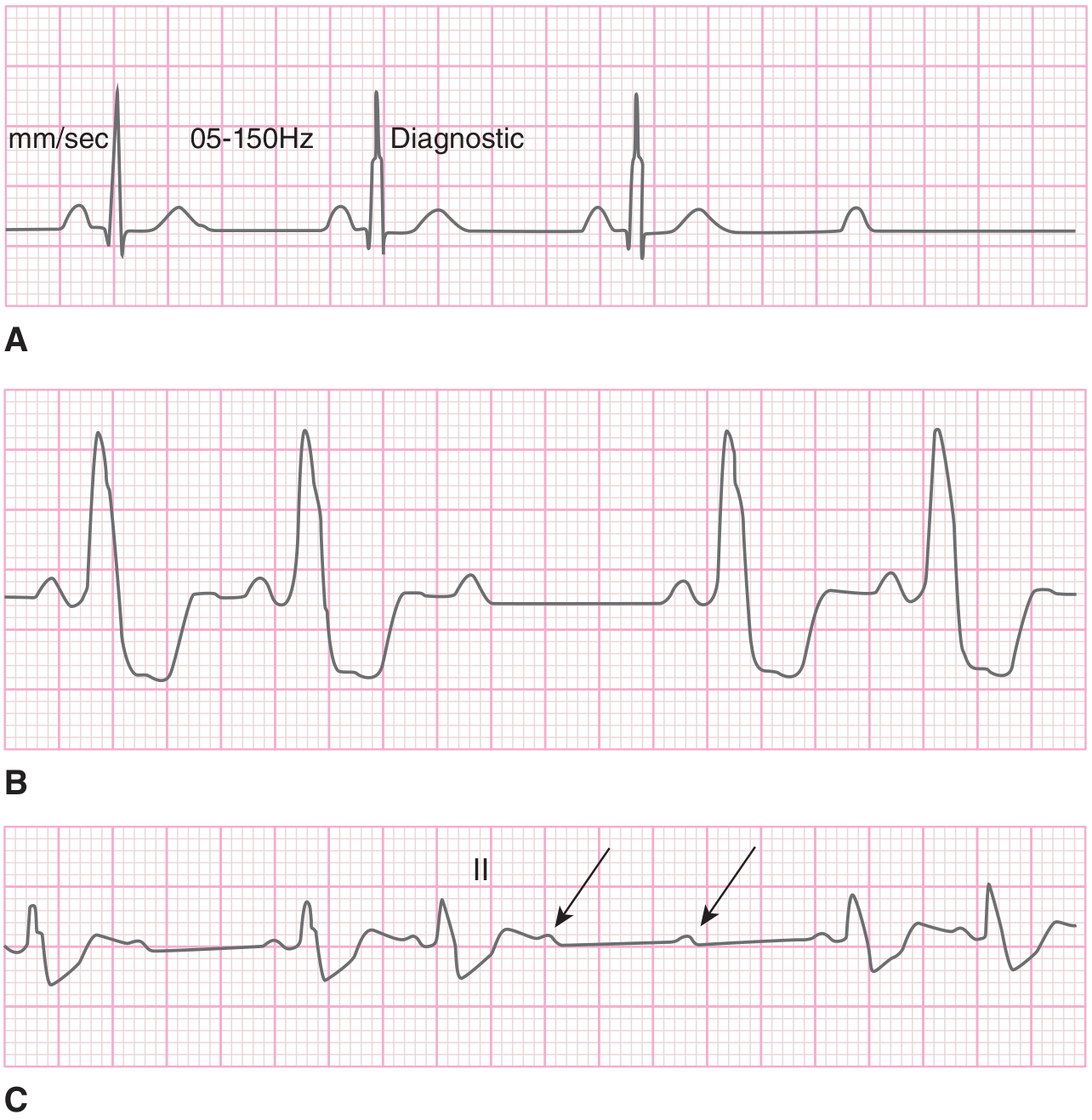
7. Second-Degree AV Block - Mobitz Type I (Wenckebach)
Key ECG features:
- Progressive prolongation of PR interval over successive beats
- Eventually a P wave is blocked (no QRS follows)
- After the dropped beat, the PR interval resets and the cycle repeats
- "Grouped beating" pattern
- Usually narrow QRS complexes
This almost always occurs at the AV node level. Frequently benign and often transient, associated with inferior MI, medication toxicity, or myocarditis. Rarely progresses to complete heart block.

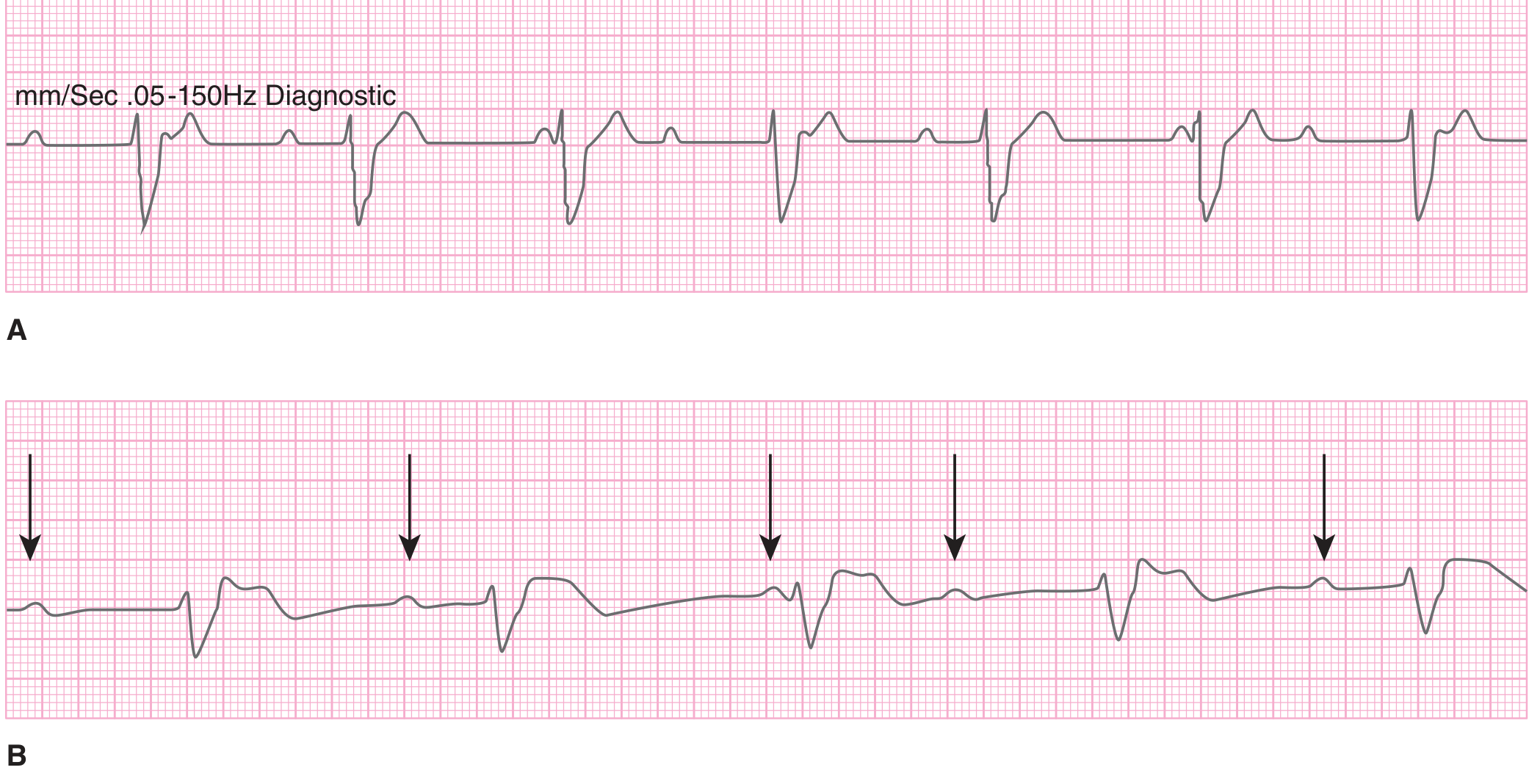
8. Second-Degree AV Block - Mobitz Type II
Key ECG features:
- Constant PR interval (no progressive lengthening)
- Sudden, unexpected non-conducted P wave (dropped QRS)
- QRS complexes are usually wide (infranodal block)
- High-grade block: two or more consecutive P waves not conducted
Mobitz II indicates structural damage to the infranodal (His-Purkinje) conducting system. It is serious because it may progress suddenly to complete heart block, especially with concomitant acute MI. Pacemaker is usually required.
9. Third-Degree (Complete) AV Block
Key ECG features:
- Complete dissociation of P waves from QRS complexes
- Atrial rate faster than ventricular rate
- Regular ventricular escape rhythm (40-60 bpm if nodal, <40 bpm if infranodal)
- QRS morphology: narrow if junctional escape pacemaker, wide if ventricular escape
- P waves "march through" QRS complexes independently
Complete absence of conduction between atria and ventricles. Nodal complete AV block (narrow QRS) complicates up to 8% of inferior MIs. Infranodal block (wide QRS) with anterior MI is ominous and usually requires urgent pacing.
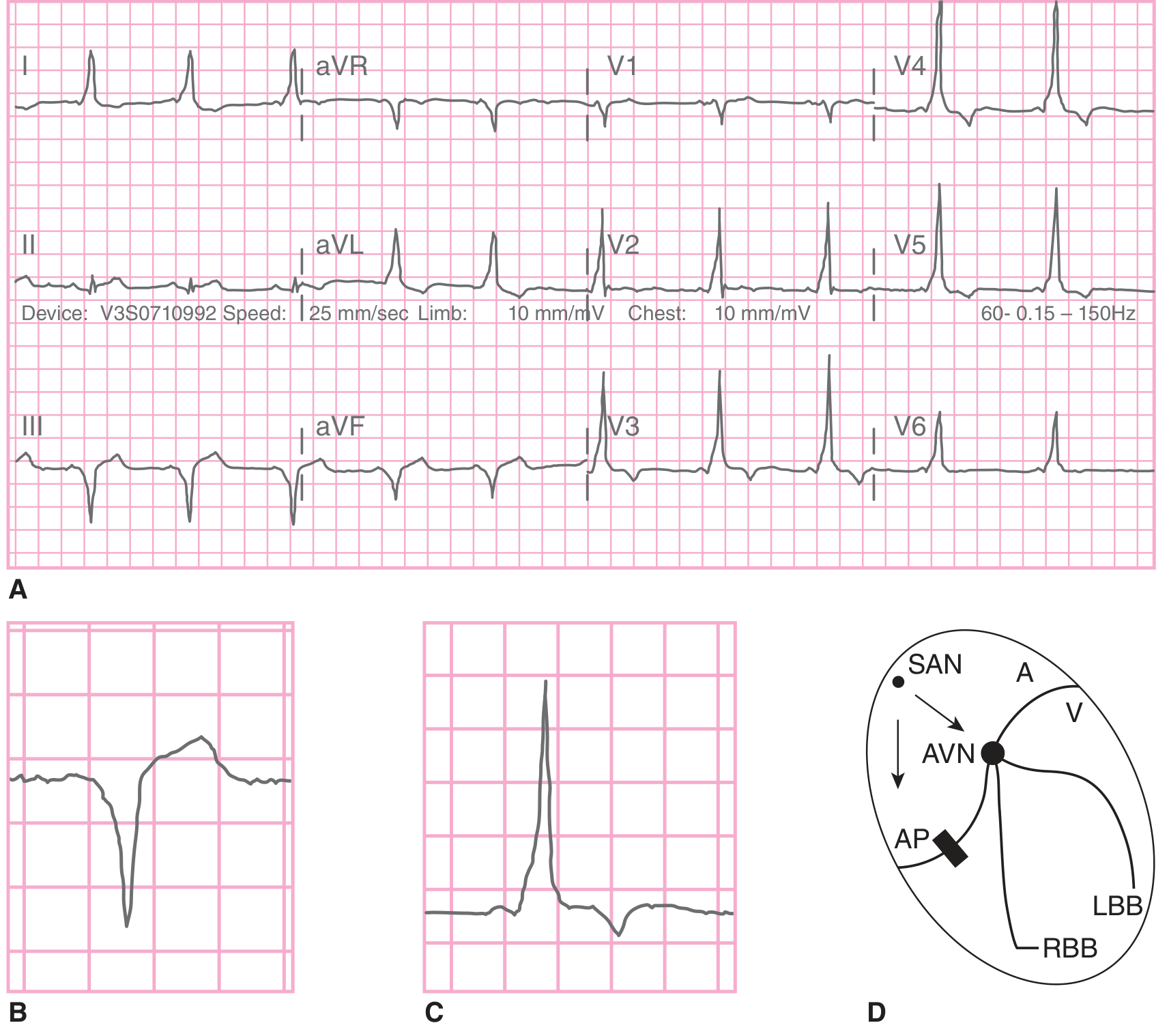
10. Wolff-Parkinson-White (WPW) Syndrome
Key ECG features (in sinus rhythm):
- Short PR interval (<120 ms)
- Delta wave (slurred upstroke of the initial QRS)
- Slightly widened QRS complex
- Secondary ST-T wave changes discordant to QRS/delta wave direction
WPW involves an accessory conduction pathway (bundle of Kent) bypassing the AV node, creating direct atrial-ventricular connection. The delta wave represents pre-excitation via the accessory pathway. Patients are prone to reentrant tachycardias (orthodromic AVRT - narrow complex; antidromic AVRT - wide complex) and atrial fibrillation with very rapid ventricular response (>200 bpm), which can degenerate into VF.
Summary Table
| # | Condition | Rate | Rhythm | P Waves | QRS |
|---|---|---|---|---|---|
| 1 | Atrial Fibrillation | 120-170 | Irregularly irregular | Absent/chaotic | Narrow |
| 2 | Atrial Flutter | ~150 (2:1) | Regular | Sawtooth ~300/min | Narrow |
| 3 | Ventricular Tachycardia | 140-300 | Regular (mono) | Dissociated | Wide |
| 4 | Ventricular Fibrillation | - | Chaotic | Absent | Absent |
| 5 | STEMI | Variable | Variable | Normal | ST elevation |
| 6 | 1st Degree AV Block | Normal | Regular | Normal | PR >200ms |
| 7 | Mobitz I (Wenckebach) | Normal | Group beats | Progressive PR↑ | Narrow |
| 8 | Mobitz II | Normal | Group beats | Fixed PR, dropped | Wide |
| 9 | Complete Heart Block | <40-60 | Regular (escape) | Dissociated | Wide/Narrow |
| 10 | WPW Syndrome | Variable | Variable | Normal | Delta wave, short PR |
Sources: Tintinalli's Emergency Medicine: A Comprehensive Study Guide; Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.