How to manage hypernatremia in pediatrics
Reading File
Finding Sources
Finding Sources
Searching PubMed
hypernatremia management children
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to provide a detailed answer on pediatric hypernatremia management. Let me compile the response.
Management of Hypernatremia in Pediatrics
Definition and Overview
Hypernatremia is defined as a serum sodium >145 mEq/L. In children, it is most commonly caused by diarrheal illness (leading cause), improper formula preparation, inadequate free water intake, or pathological water loss. Serum Na+ >160 mEq/L requires immediate attention due to risk of permanent neurologic sequelae, and levels >180 mEq/L may require dialysis.
Infants are particularly vulnerable because they cannot access free water independently and have a higher body surface area-to-volume ratio, leading to greater insensible losses.
Diagnostic Approach
The diagnostic flowchart below helps classify the cause based on ECF volume and urine findings:
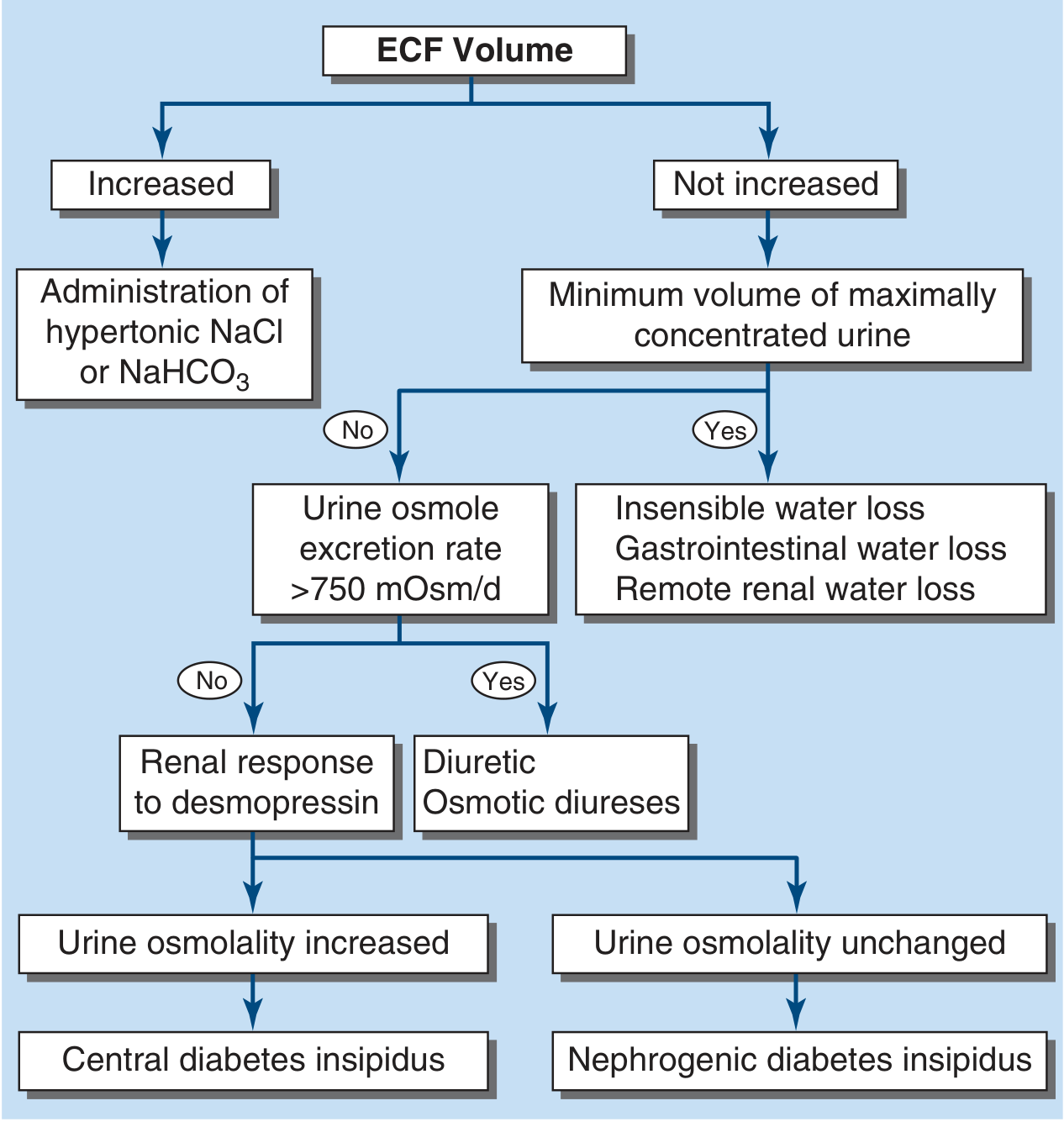
Figure: Diagnostic approach to hypernatremia - Harrison's Principles of Internal Medicine 22E
Key categories:
| Type | Cause | Example |
|---|---|---|
| Hypovolemic | Water loss > Na loss | Diarrhea, vomiting, burns, osmotic diuresis |
| Euvolemic | Pure water loss | Diabetes insipidus (central or nephrogenic), insensible losses |
| Hypervolemic | Excess Na+ gain | Hypertonic saline/NaHCO3 administration, hyperaldosteronism |
Clinical Features
Symptoms result from cellular dehydration as free water shifts from intracellular to extracellular space:
- Irritability, high-pitched cry (infants)
- Mental status changes, lethargy
- Muscular weakness, hyper- or hyporeflexia
- Tremors, myoclonus, asterixis, chorea
- Nuchal rigidity, increased peripheral tone
- Seizures, intracerebral hemorrhage
- Death (in severe untreated cases)
In chronic hypernatremia, brain cells generate idiogenic osmoles (organic osmolytes) to resist cellular shrinkage. This adaptation is why rapid correction is particularly dangerous in children - it causes water to rush into brain cells, causing cerebral edema.
Management: Step-by-Step Approach
Step 1 - Assess Volume Status (Priority #1)
Volume status must be assessed FIRST. Hemodynamic instability always takes precedence over correcting sodium.
If hypovolemic and hemodynamically unstable:
- Give isotonic NS 20 mL/kg IV boluses, reassessing after each bolus until stable
- Do NOT give hypotonic fluids while the patient is in shock
- Once euvolemia is achieved, then address the free water deficit
Step 2 - Calculate Free Water Deficit
Once stable, calculate the free water deficit:
Formula (Tintinalli's / pediatric formula):
Free water deficit (mL) = 4 mL × body weight (kg) × [desired change in serum Na (mEq/L)]
Alternative formula (adults/nephrology):
Water deficit (L) = TBW × ([Na+]/140 - 1) where TBW = 0.6 × weight (kg) in children
Example: A 10-kg child with Na+ = 165 mEq/L, target Na+ = 145 mEq/L:
- Free water deficit = 4 mL × 10 kg × (165-145) = 800 mL
Note: This formula does NOT account for ongoing losses (urine, stool, insensible). These must be estimated and added to replacement volumes.
Step 3 - Determine Rate of Correction (Critical in Pediatrics)
This is the most important and controversial aspect of pediatric hypernatremia management.
| Duration | Target Correction Rate |
|---|---|
| Acute hypernatremia (<48h) | No faster than 1 mEq/L/hr, no more than 10-12 mEq/L/day |
| Chronic hypernatremia (>48h) | More conservative: 5-8 mEq/L/day |
| General pediatric rule | Never exceed 0.5 mEq/L/hr - case series show seizures at faster rates |
| Maximum in first 24h | No more than 15 mEq/L in the first 24 hours |
Animal studies and pediatric case series specifically suggest that correction >0.5 mEq/L/hr can provoke seizures due to cerebral edema from the osmolyte-loaded brain cells drawing in water. - Comprehensive Clinical Nephrology, 7th Edition
Complete correction may take >48 hours. Monitor serum Na+ every 1-2 hours initially.
Step 4 - Choose Replacement Fluid
| Situation | Fluid Choice |
|---|---|
| Hemodynamic instability | Normal saline (0.9% NaCl) boluses first |
| Mild-moderate hypernatremia, volume stable | 0.45% NaCl (half-normal saline) |
| Moderate-severe once stable | D5W or 0.2% NaCl (quarter NS) |
| Oral/NG route available | Oral water or dilute feeds - preferred when possible |
- The preferred route is oral or nasogastric water/feeds when the child is not vomiting and is hemodynamically stable
- IV D5W or quarter NS are alternatives
- For hypovolemia, 0.45% NS corrects both volume and partially addresses the free water deficit simultaneously
Fluid administration schedule (Tintinalli's pediatric protocol):
- Subtract bolus fluids already given from the calculated deficit
- Give half the remaining deficit over the first 8 hours
- Give the remaining half over the next 16 hours
- Add maintenance fluids and estimated ongoing losses on top of this
Step 5 - Treat the Underlying Cause
Central Diabetes Insipidus (CDI):
- Treat with DDAVP (desmopressin) - a vasopressin analog
- Intranasal: 5-30 mcg once or twice daily
- Oral: 0.05-0.8 mg/day in divided doses
Nephrogenic Diabetes Insipidus (NDI):
- Low-sodium diet + thiazide diuretics (induces mild volume depletion, enhancing proximal water reabsorption)
- NSAIDs (indomethacin) can be added in select cases
- Remove offending drugs (lithium, ifosfamide) if applicable
Hypervolemic hypernatremia (iatrogenic Na+ excess):
- Discontinue hypertonic infusions
- Diuretics to eliminate excess sodium (furosemide)
- Dialysis if sodium cannot be reduced without causing volume overload, or if Na+ >180 mEq/L
Hypernatremic dehydration from diarrhea/gastroenteritis:
- Oral rehydration solution (ORS) is preferred when tolerated
- Use low-osmolarity ORS (the 2024 systematic review, PMID 39641334 confirms low-osmolarity ORS is effective for childhood diarrhea-related dehydration)
Step 6 - Monitor Closely
- Check serum Na+ every 1-2 hours initially
- Adjust infusion rate based on trending results
- Monitor urine output - risk of acute tubular necrosis in severe cases
- A single calculation is never enough - the dynamic balance of ongoing losses requires frequent reassessment
- Watch for signs of cerebral edema during correction: worsening headache, vomiting, seizures, altered consciousness
Special Considerations in Neonates/Infants
- Neonatal hypernatremic dehydration is frequently linked to breastfeeding failure/inadequate intake. A 2024 systematic review (PMID 39111773) identified maternal risk factors including primiparous mothers, flat/inverted nipples, and delayed lactogenesis.
- Use TBW = 0.7 × weight (kg) in neonates (higher body water content)
- Oral rehydration is preferred over IV when possible
- Formula preparation errors (concentrated formula) are a preventable cause
Maintenance Fluid Choice After Correction
The 2024 meta-analysis (PMID 37365423) confirms isotonic (0.9% NaCl) maintenance fluids are safer than hypotonic fluids for hospitalized children to prevent iatrogenic hyponatremia - but this is for maintenance, not for correction of established hypernatremia.
Summary Algorithm
Hypernatremia (Na+ >145 mEq/L)
|
Hemodynamically unstable?
YES → NS boluses 20 mL/kg until stable
|
Now stable → Calculate free water deficit
(4 mL × kg × desired ΔNa+)
|
Choose fluid (½NS, ¼NS, D5W, or oral)
|
Correct at ≤0.5 mEq/L/hr
(max 10-12 mEq/L/day, 15 mEq/L in first 24h)
|
Monitor Na+ q1-2h, adjust rate
|
Identify & treat underlying cause
(DI → DDAVP or thiazide; excess Na+ → stop source/diurese)
Sources: Tintinalli's Emergency Medicine (Comprehensive Study), p. 763-781 | Washington Manual of Medical Therapeutics, p. 2583-2615 | National Kidney Foundation Primer on Kidney Diseases 8e, p. 3721-3754 | Comprehensive Clinical Nephrology 7th Ed., p. 1068-1080 | Harrison's Principles of Internal Medicine 22E, p. 2845-2865
This is a shared conversation. Sign in to Orris to start your own chat.