Can you teach me respiratory drugs from basic as i sm i
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have everything I need from Katzung's textbook. Let me compile a thorough, beginner-friendly lesson on all respiratory drugs.
Respiratory Drugs - A Complete Beginner's Guide
Based on Katzung's Basic & Clinical Pharmacology, 16th Edition
Why Do We Need Respiratory Drugs?
The airways can become too narrow (bronchoconstriction) due to:
- Muscle spasm (smooth muscle contracts)
- Inflammation and swelling (mucosal edema)
- Excess mucus production
The drugs we use either open the airways (bronchodilators) or reduce inflammation (controllers). Think of it like a pipe - you either widen it or stop it from getting clogged.
The Big Picture - How Bronchial Tone Is Controlled
This is the most important concept. Look at this diagram:
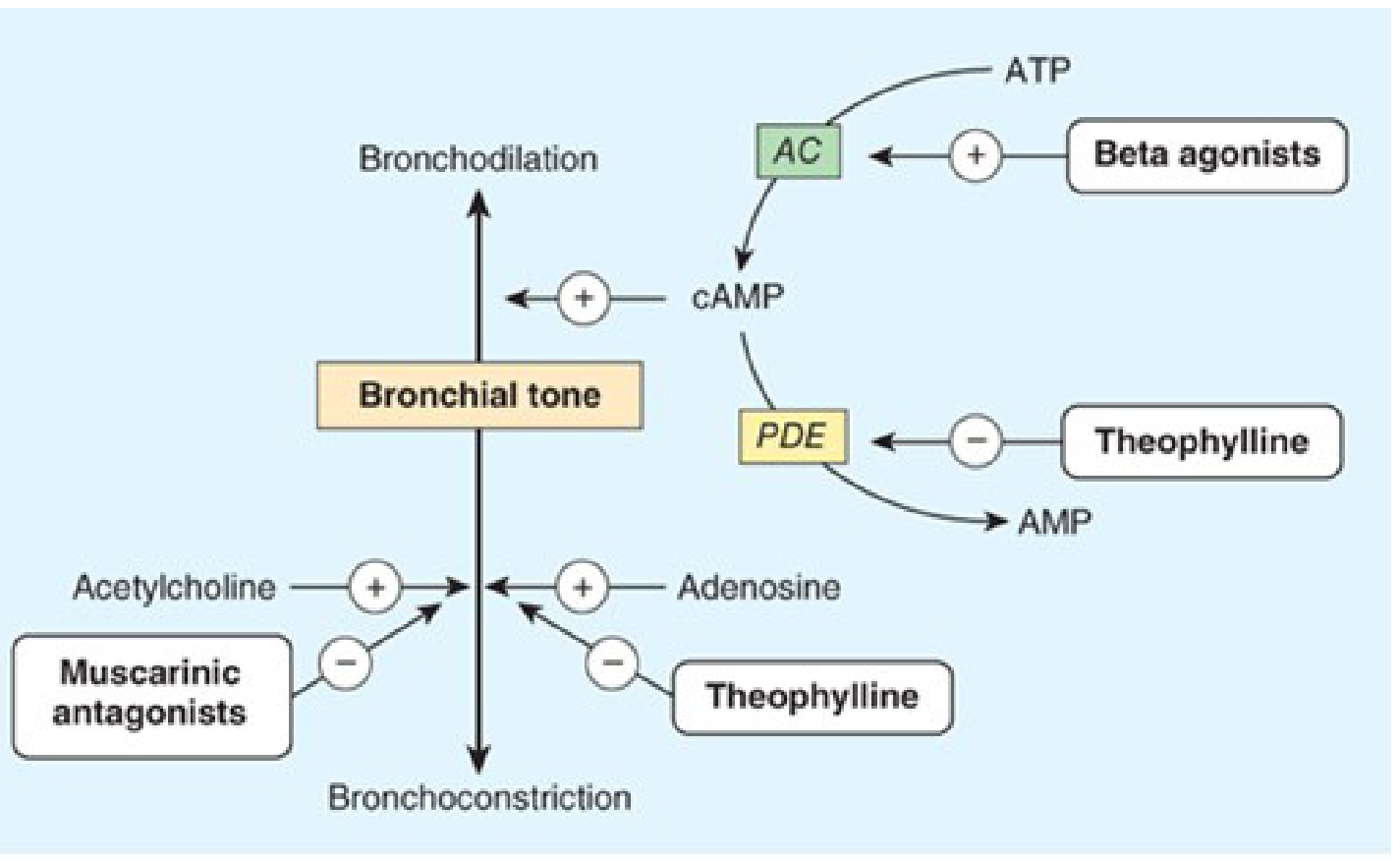
Key concept:
- cAMP = bronchodilation (high cAMP = open airways)
- Acetylcholine (via muscarinic receptors) = bronchoconstriction
- Adenosine = bronchoconstriction
So drugs work by either:
- Increasing cAMP (Beta agonists - activate adenylyl cyclase AC)
- Preventing cAMP breakdown (Theophylline - blocks PDE enzyme)
- Blocking acetylcholine (Muscarinic antagonists like ipratropium)
CLASS 1: Beta-2 Agonists (Bronchodilators / "Relievers")
How they work
Beta agonists bind to beta-2 (β2) receptors on airway smooth muscle → activate adenylyl cyclase (AC) → increase cAMP → smooth muscle relaxes → airways open.
They also:
- Inhibit mast cell mediator release
- Reduce microvascular leakage
- Increase mucociliary transport (helps clear mucus)
The Drug Structures
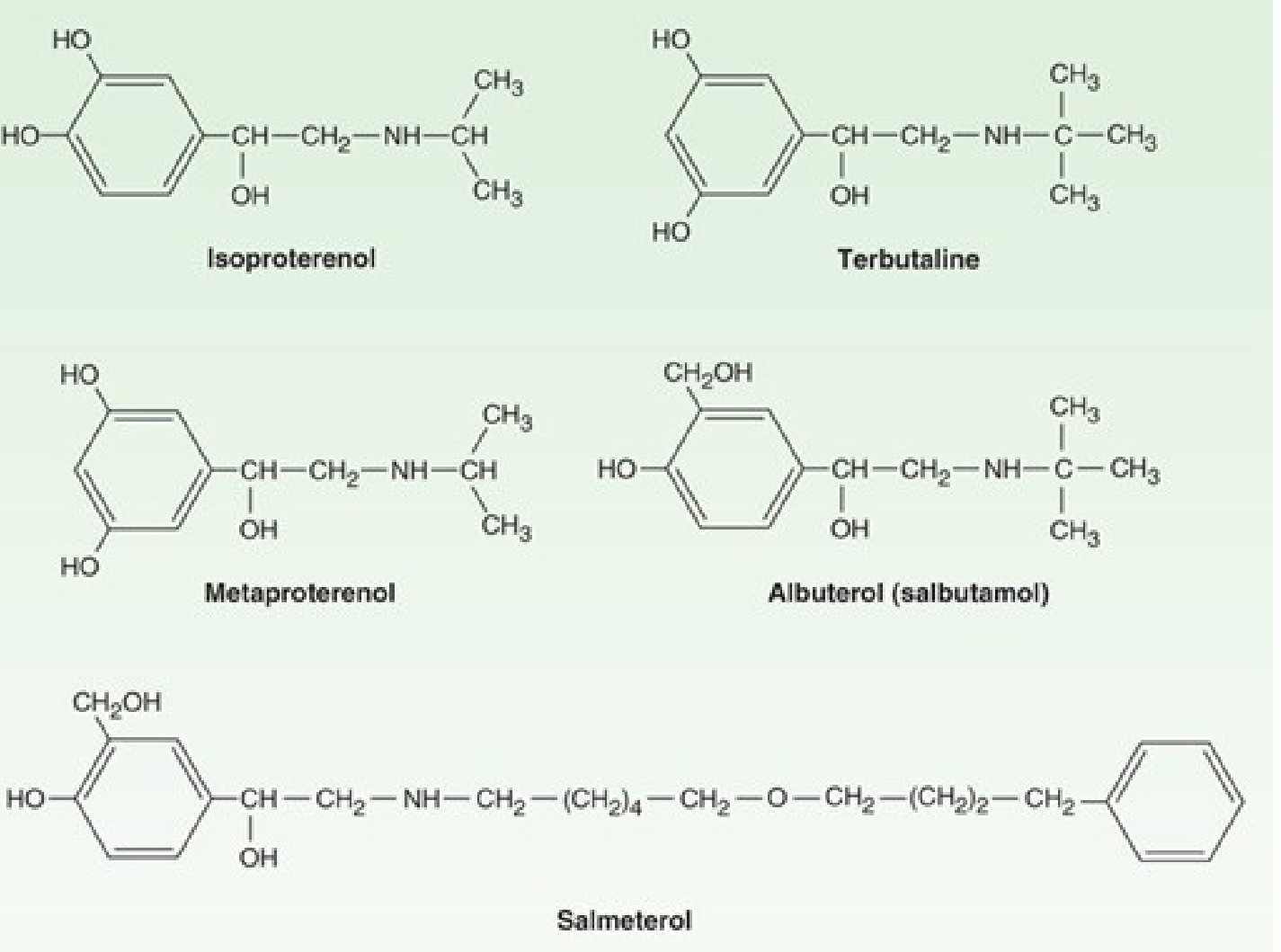
Short-Acting Beta-2 Agonists (SABAs) - "Rescue Inhalers"
| Drug | Key Points |
|---|---|
| Albuterol (Salbutamol) | Most widely used SABA; onset 5-15 min; lasts 4-6 hrs |
| Terbutaline | Also available SC (subcutaneous) injection for severe attacks |
| Metaproterenol | Older, less selective than albuterol |
Use: Acute bronchospasm relief. Using >2 canisters/month = danger sign of poorly controlled asthma.
Long-Acting Beta-2 Agonists (LABAs) - "Controllers"
| Drug | Key Points |
|---|---|
| Salmeterol | Onset ~20 min; duration 12+ hrs; note the very long tail in the chemical structure above! |
| Formoterol | Faster onset than salmeterol; also 12 hr duration |
Important rule: LABAs are NEVER used alone in asthma - always combined with an inhaled corticosteroid (ICS) because using a LABA alone without ICS increases the risk of fatal asthma attacks.
Adverse Effects of Beta Agonists
- Tachycardia (from β1 receptor activation)
- Skeletal muscle tremor (very common, especially with systemic use)
- Hypokalemia (decreased serum potassium - can worsen with high doses)
Route: Why Inhaled?
Inhalation delivers drug directly to airways, giving the greatest local effect with least systemic toxicity. However, even with the optimal particle size (2-5 µm), 80-90% of the aerosol is deposited in the mouth/pharynx - this is why rinsing the mouth after using inhalers matters (especially with corticosteroids).
CLASS 2: Anticholinergics / Muscarinic Antagonists
How they work
Block muscarinic (M3) receptors in airway smooth muscle → prevent acetylcholine from causing bronchoconstriction → airways stay open.
Think of it as "removing the brake pedal" from the bronchoconstriction reflex.
Key Drugs
| Drug | Type | Duration | Use |
|---|---|---|---|
| Ipratropium | Short-acting (SAMA) | 4-6 hrs | Acute COPD exacerbations; added to albuterol in severe asthma attacks |
| Tiotropium | Long-acting (LAMA) | 24 hrs (once daily) | Maintenance therapy for COPD; also used in difficult asthma |
| Glycopyrronium, Umeclidinium, Aclidinium | LAMAs | 12-24 hrs | COPD maintenance |
Adverse Effects (classic anticholinergic: "dry as a bone, blind as a bat")
- Dry mouth (most common)
- Urinary retention (caution in BPH)
- Blurred vision if accidentally sprayed in eyes
- Constipation
- No significant cardiac effects at inhaled doses (unlike systemic atropine)
CLASS 3: Methylxanthines (Theophylline)
How they work (two mechanisms - look at the diagram again)
- Inhibit phosphodiesterase (PDE) → cAMP is NOT broken down → stays high → bronchodilation
- Adenosine receptor antagonism → blocks adenosine-mediated bronchoconstriction
Also has anti-inflammatory effects and stimulates respiratory drive (useful in apnea of prematurity).
Theophylline - Key Drug
- Given orally (sustained-release) or IV (aminophylline = theophylline + ethylenediamine)
- Narrow therapeutic index - requires blood level monitoring (target: 5-15 mg/L)
- Half-life is variable - affected by smoking, liver disease, drugs
Adverse Effects (dose-dependent, watch levels!)
- Mild: Nausea, vomiting, headache, insomnia, tremor
- Moderate: Tachycardia, arrhythmias
- Severe/Toxic: Seizures (can be life-threatening), ventricular arrhythmias
Drug interactions that raise theophylline levels (risk of toxicity)
- Ciprofloxacin, erythromycin (CYP1A2 inhibitors)
- Cimetidine
Theophylline levels decreased by
- Smoking (induces CYP1A2)
- Phenytoin, rifampin
Clinical note: Theophylline is now a third-line agent for asthma due to its toxicity profile. Still used in some COPD patients for bronchodilation + respiratory muscle stimulation.
CLASS 4: Inhaled Corticosteroids (ICS) - "Controllers"
How they work
Bind to glucocorticoid receptors → enter the nucleus → inhibit transcription of inflammatory cytokines (IL-4, IL-5, IL-13, TNF-α) → reduce eosinophilic inflammation → decrease airway hyperresponsiveness and mucus production.
They do NOT cause immediate bronchodilation - they treat the underlying inflammation.
Key Drugs
| Drug | Notes |
|---|---|
| Beclomethasone | Older ICS, first widely used |
| Fluticasone | High potency, low systemic bioavailability |
| Budesonide | Can also be nebulized; safe in pregnancy |
| Mometasone | Once-daily dosing; also used for T2-high asthma |
| Ciclesonide | Pro-drug, activated in the lung; lower oral candidiasis risk |
Adverse Effects
- Local: Oral candidiasis (thrush), dysphonia (hoarse voice) - both prevented by rinsing mouth/using a spacer
- Systemic (at high doses): Adrenal suppression, osteoporosis, growth retardation in children, cataracts
Combination Products (ICS + LABA)
These are the most commonly prescribed inhalers for moderate-severe asthma and COPD:
- Fluticasone + Salmeterol (Advair/Seretide)
- Budesonide + Formoterol (Symbicort)
- Fluticasone furoate + Vilanterol (Breo Ellipta)
CLASS 5: Leukotriene Modifiers
Background
Leukotrienes (LTC4, LTD4, LTE4) are inflammatory mediators released from mast cells and eosinophils. They cause:
- Bronchoconstriction
- Increased mucus secretion
- Airway edema
Two Types of Drugs
a) Leukotriene Receptor Antagonists (LTRAs)
- Montelukast (most widely used) - oral, once daily
- Zafirlukast - oral, twice daily
Mechanism: Block CysLT1 receptors → block leukotriene effects
Use: Mild persistent asthma, aspirin-exacerbated asthma (excellent!), allergic rhinitis + asthma
Adverse effects: Generally well tolerated; rare: Churg-Strauss syndrome (systemic vasculitis); Montelukast now has an FDA black box warning for neuropsychiatric effects (mood changes, suicidality - especially in children)
b) 5-Lipoxygenase Inhibitor
- Zileuton - blocks the enzyme that makes leukotrienes
Adverse effects: Hepatotoxicity (requires LFT monitoring)
CLASS 6: Cromones (Mast Cell Stabilizers)
Key Drugs
- Cromolyn sodium (sodium cromoglycate)
- Nedocromil
How they work
Stabilize mast cell membranes → prevent degranulation → no release of histamine, leukotrienes, or other mediators.
Use
- Prophylaxis of asthma (especially exercise-induced or allergen-induced)
- Must be used before exposure - no use in acute attacks
- Very safe (minimal side effects)
- Now rarely used due to availability of better alternatives
CLASS 7: Biologics / Monoclonal Antibodies
These target specific immune pathways - used for severe, refractory asthma when standard therapy fails.
| Drug | Target | Use |
|---|---|---|
| Omalizumab | Anti-IgE (binds free IgE) | Allergic asthma with high IgE |
| Mepolizumab | Anti-IL-5 | Eosinophilic asthma |
| Benralizumab | Anti-IL-5Rα (IL-5 receptor) | Eosinophilic asthma |
| Dupilumab | Anti-IL-4Rα (blocks IL-4 & IL-13) | Moderate-severe asthma + atopic dermatitis |
| Tezepelumab | Anti-TSLP | Severe asthma (all phenotypes) |
T2-high asthma = eosinophilic inflammation → responds to mepolizumab, benralizumab, dupilumab
T2-low asthma = non-eosinophilic → harder to treat; tezepelumab may help
CLASS 8: Mucolytics and Expectorants
These drugs thin and help clear mucus.
| Drug | Mechanism | Notes |
|---|---|---|
| N-acetylcysteine (NAC) | Breaks disulfide bonds in mucus glycoproteins | Also used for paracetamol overdose |
| Guaifenesin | Increases respiratory secretion hydration | Common OTC expectorant |
| Dornase alfa | DNase enzyme breaks down DNA in thick mucus | Used in cystic fibrosis |
| Hypertonic saline | Osmotic - draws water into airway lumen | Cystic fibrosis, bronchiectasis |
Quick Summary Table: Asthma Step-Up Therapy
| Severity | Treatment |
|---|---|
| Intermittent | SABA (albuterol) as needed only |
| Mild persistent | Low-dose ICS + SABA PRN |
| Moderate persistent | Low-medium ICS + LABA (or medium ICS alone) |
| Severe persistent | High-dose ICS + LABA +/- LAMA +/- biologic |
| Very severe | Add systemic corticosteroids; consider omalizumab or other biologics |
COPD vs Asthma - Drug Differences
| Feature | Asthma | COPD |
|---|---|---|
| Main problem | Reversible bronchoconstriction + inflammation | Irreversible airflow limitation + emphysema |
| First-line bronchodilator | SABA (albuterol) | LAMA (tiotropium) or LABA |
| Anti-inflammatory | ICS (essential) | ICS only in frequent exacerbators |
| Biologic use | Yes (for severe) | Not routine |
| Theophylline | Third-line | Still used adjunct |
| Phosphodiesterase-4 inhibitor | Rarely | Roflumilast (for severe COPD) |
Roflumilast (PDE-4 inhibitor, oral) - specifically for COPD with chronic bronchitis + frequent exacerbations. Reduces inflammation. Side effects: nausea, diarrhea, weight loss, psychiatric effects.
Memory Tips
- SABAs = "Save-A-Breath Acutely" = rescue inhalers
- LABAs = "Long-Acting, never Alone in Asthma"
- ICS = treat the fire (inflammation), not the smoke (symptoms)
- Theophylline = narrow index, need levels, watch for seizures
- Tiotropium = "Tio for COPD daily" (once daily LAMA)
- Montelukast = good for aspirin-sensitive asthma + allergic rhinitis
Source: Katzung's Basic & Clinical Pharmacology, 16th Edition, Chapter 20
This covers all the major respiratory drug classes from first principles. Would you like me to go deeper on any particular class - for example, more detail on inhalers/devices, specific drug doses, or drug interactions? I can also create a visual summary diagram or quiz you on the material!
This is a shared conversation. Sign in to Orris to start your own chat.