Isotropic imaging in ct in detail
Reading File
Finding Sources
Finding Sources
Searching the Web
isotropic imaging CT scan radiology multiplanar reconstruction voxel
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Searching Images
isotropic CT multiplanar reconstruction voxel axial coronal sagittal
Finding Sources
Loading Image
I have all the material needed. Here is a comprehensive, detailed explanation of isotropic imaging in CT.
Isotropic Imaging in CT
1. Definition and Core Concept
Isotropic imaging in CT refers to the acquisition of a volumetric dataset in which the spatial resolution is equal in all three dimensions — the x-axis, y-axis, and z-axis (the long axis of the patient). This means each unit of data (a voxel) is a perfect or near-perfect cube, as opposed to the conventional rectangular cuboid ("anisotropic") voxel where the z-dimension (slice thickness) is larger than the in-plane x–y dimensions.
| Anisotropic (conventional) | Isotropic (modern MDCT) | |
|---|---|---|
| Voxel shape | Rectangular cuboid | Cube |
| In-plane (x–y) resolution | High (e.g., 0.5 mm) | High (e.g., 0.5 mm) |
| Z-axis resolution | Poor (e.g., 5–10 mm slice) | Equal to x–y (e.g., 0.5 mm) |
| MPR quality | Degraded ("staircase" artifact) | Equivalent in all planes |
2. Historical Context and Technical Prerequisites
Before multi-detector CT (MDCT), single-slice helical scanners produced thick slices (typically 5–10 mm). The x–y in-plane pixel size might be 0.5–0.7 mm, but the z-dimension of each slice was 10–20× larger. Reformatted images in the coronal or sagittal plane therefore had coarse, "blocky" resolution — effectively useless for detailed diagnosis.
The introduction of multidetector CT (MDCT) — first 4-slice, then 16-, 64-, and now 320+ detector row systems — allowed:
- Sub-millimetre collimation throughout the entire body in a single breath-hold
- Overlapping reconstruction (using a low pitch, e.g., pitch < 1) to further improve z-resolution
- Generation of isotropic or near-isotropic voxels as small as 0.4–0.6 mm in all dimensions
"Current CT systems are sophisticated scanners, allowing the whole body to be imaged in seconds with sub-millimetre isotropic spatial resolution. High-quality multiplanar reformats and volume rendering are now standard." — Grainger & Allison's Diagnostic Radiology
3. Technical Requirements for Isotropic Acquisition
3.1 Thin-Slice Acquisition
The detector must collect data in thin collimated slices (≤1 mm). Modern 64-slice scanners routinely use 0.625 mm detector rows; 256/320-slice systems use 0.5 mm rows.
3.2 Low Pitch / Overlapping Reconstruction
Reconstruction with a pitch ≤1 allows overlapping of the helical data, improving z-axis sensitivity. This reduces partial-volume averaging (the averaging of CT numbers within a thick voxel that obscures small structures or blurs tissue boundaries).
3.3 Reconstruction Kernel
A suitable reconstruction kernel (filter) must be applied. Sharp ("bone") kernels resolve fine detail (e.g., temporal bone, lung parenchyma) but amplify noise; smooth ("soft tissue") kernels reduce noise.
3.4 Post-processing Workstation
Isotropic datasets require a workstation capable of:
- Multiplanar reformatting (MPR)
- Maximum intensity projection (MIP)
- Volume rendering (VR)
- Curved planar reformatting (CPR)
4. Voxel Size and Partial Volume Effect
Partial volume effect occurs when a voxel straddles two different tissue types; the CT number assigned to that voxel is an average of both, reducing contrast resolution. In thick-slice (anisotropic) imaging, every coronal or sagittal pixel spans the full slice thickness, severely degrading resolution.
With isotropic voxels:
- The partial volume effect is minimised equally in all planes
- Small structures (e.g., small airways, fine fracture lines, coronary arteries) are better delineated
- No plane is preferentially degraded
5. Multiplanar Reformatting (MPR) — The Primary Clinical Benefit
The most immediate clinical value of isotropic imaging is the ability to generate high-quality reformats in any plane from a single acquisition:
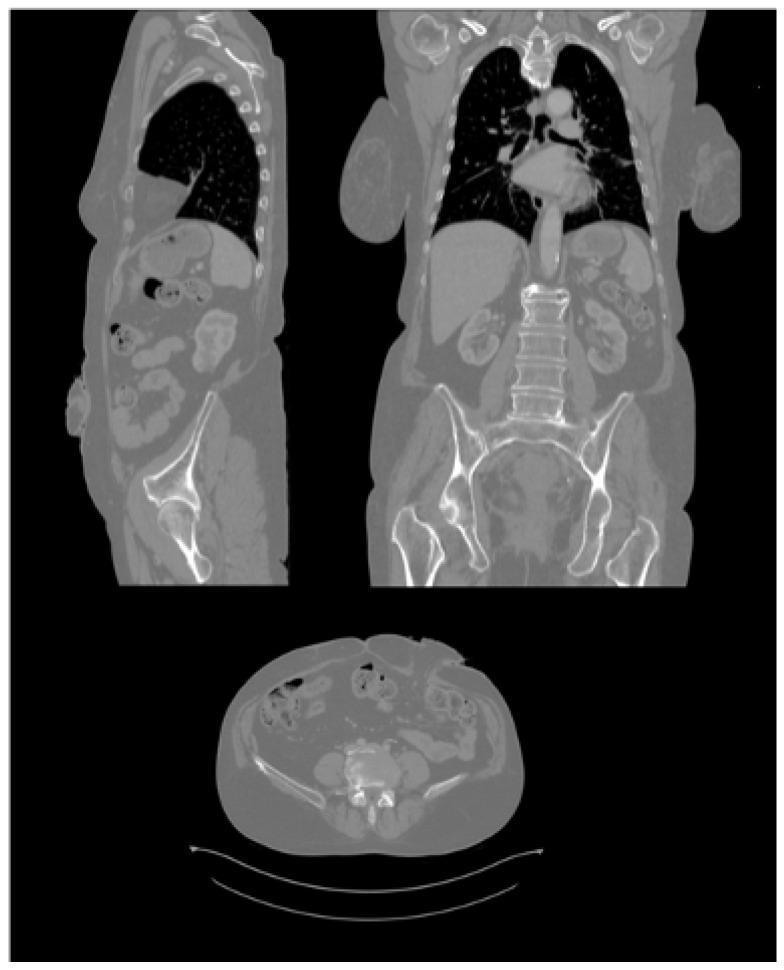
Multiplanar reconstruction from an isotropic CT dataset showing sagittal (left), coronal (right), and axial (bottom) planes — all with equivalent image quality.
Key MPR planes and their clinical uses:
| Plane | Clinical Application |
|---|---|
| Coronal | Delineates superior-inferior lesion extent, renal/adrenal anatomy, craniofacial fractures, lung apices to bases |
| Sagittal | Spine alignment, aortic arch anatomy, anterior-posterior lesion extent |
| Oblique | Tailored to organ of interest (e.g., oblique coronal for inner ear ossicles) |
| Curved planar | Vessel lumen along its full length (e.g., carotid, coronary arteries, aorta) |
"With isotropic CT, acquired imaging can be reformatted in any plane to fully evaluate the anatomy and extent of disease. The coronal plane is excellent for delineating the superior-inferior extent of a lesion." — Cummings Otolaryngology, Head and Neck Surgery
"The ability to produce isotropic voxels allows multiplanar reformatting to be undertaken as a routine, either by the radiographic staff or at the time of reporting by the radiologist." — Grainger & Allison's Diagnostic Radiology
6. Advanced 3D Post-Processing Techniques
Isotropic datasets are the foundation for all advanced 3D visualisation:
6.1 Volume Rendering (VR)
Each voxel is assigned a unique colour and transparency based on its Hounsfield Unit (HU) value and relationship to adjacent voxels. Clinician-controlled opacity transfer functions allow selective display of bone, vessels, or soft tissue. Applications: CT angiography, orthopaedic surgery planning, craniofacial reconstruction.
6.2 Maximum Intensity Projection (MIP)
The brightest voxel along a projection ray is displayed, making high-attenuation structures (contrast-enhanced vessels, calcifications) stand out. Used extensively in CT angiography and pulmonary nodule detection.
6.3 Minimum Intensity Projection (MinIP)
The lowest HU voxel along a ray is displayed — used for airway imaging (bronchiectasis, tracheal stenosis).
6.4 Virtual Endoscopy / CT Colonography
Isotropic data allows fly-through simulations of hollow organs (colon, trachea, bronchi). Clinically validated for colorectal polyp detection.
6.5 Curved Planar Reformation (CPR)
A curved slab through a tubular structure (e.g., artery, ureter) is "unrolled" into a single flat image displaying the entire lumen and wall.
7. Clinical Applications
Isotropic imaging has transformed the following specialties in particular:
| Specialty | Application |
|---|---|
| CT Angiography | Aortic dissection, pulmonary embolism, coronary CTA, peripheral vascular disease |
| Trauma | Facial fracture classification (Le Fort, nasoethmoidal, tripod), occult spinal fractures |
| Skull base / ENT | Temporal bone, ossicles, petrous apex, craniofacial pathology |
| Uro-radiology | CT urography: urothelial imaging, renal mass characterisation, calculi |
| Thoracic | Airway stenosis, bronchiectasis, lung nodule characterisation |
| Oncology | Staging, treatment response, multiplanar lesion measurement |
| Musculoskeletal | Trabecular architecture, cartilage surface mapping (extremity CT ~<80 µm voxels) |
| Virtual colonoscopy | Polyp detection, computer-aided detection (CAD) |
8. Dose Implications
An important practical point: generating MPR images from an isotropic dataset does not increase radiation dose because the reformats are computed post-hoc from the original acquisition.
"With modern isotropic CT scanners, obtaining multi-planar reformats does not increase the dose because these are generated from existing images, rather than an additional acquisition." — Yamada's Textbook of Gastroenterology
Additional acquisitions (e.g., separate arterial + portal venous + delayed phases) still each add dose. Dose reduction techniques (iterative reconstruction, tube current modulation, low-kV protocols) can reduce dose by 50–75% without sacrificing the isotropic resolution necessary for high-quality MPR.
9. Noise Trade-off
Thinner slices = better z-resolution → isotropic voxels, but smaller voxels contain fewer X-ray photons → more image noise.
Strategies to mitigate:
- Iterative reconstruction algorithms (ASIR, SAFIRE, AIDR, deep-learning reconstruction) — allow dose reduction while maintaining SNR
- Post-processing noise filters at the workstation
- Image averaging / slab MIP in specific applications (e.g., 3–5 mm MIP slabs for nodule detection)
10. Comparison: Isotropic CT vs. Isotropic MRI
Both CT and MRI now employ isotropic acquisition strategies, but the mechanisms differ:
| Feature | CT | MRI |
|---|---|---|
| Mechanism | X-ray attenuation | Radiofrequency absorption by H nuclei |
| Isotropic basis | Thin-slice multidetector acquisition | 3D gradient-echo/spin-echo sequences |
| Typical isotropic resolution | 0.4–0.6 mm | 0.9–1.2 mm (routine); < 0.5 mm (research) |
| Radiation | Yes | No |
| Bone detail | Excellent | Limited |
| Soft tissue contrast | Moderate | Superior |
MRI 3D isotropic techniques (e.g., SPACE, CUBE, VISTA sequences) are specifically used for skull base, spine, and knee imaging.
Summary
| Key Point | Detail |
|---|---|
| Definition | Equal spatial resolution in x, y, and z; cubic voxel |
| Enabled by | MDCT with ≥64 detector rows, sub-mm collimation |
| Core benefit | High-quality MPR in any plane from a single acquisition |
| Eliminates | Preferential in-plane degradation; staircase artifact in reformats |
| Reduces | Partial volume effect |
| Dose | MPR itself adds no dose; thin-slice acquisition managed with iterative reconstruction |
| Clinical revolution | CTA, trauma imaging, virtual endoscopy, skull base CT, CT urography |
Sources: Grainger & Allison's Diagnostic Radiology; Cummings Otolaryngology Head and Neck Surgery; Yamada's Textbook of Gastroenterology, 7th ed.; Radiology Cafe FRCR Physics Notes.
4d ct in detail
Finding Sources
Finding Sources
Searching the Web
4D CT four dimensional CT radiology applications radiation therapy cardiac perfusion
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Searching Images
4D CT scan parathyroid adenoma four phase contrast
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
I now have comprehensive material from multiple authoritative sources. Let me compose the full answer.
4D CT (Four-Dimensional Computed Tomography) — In Detail
1. What is 4D CT?
In conventional CT, the three spatial dimensions are x, y, and z. 4D CT adds time as the fourth dimension, producing a series of 3D volumetric datasets acquired at multiple time points. This enables imaging of dynamic processes — whether physiological motion (breathing, cardiac contraction) or pharmacokinetic events (contrast enhancement and washout over time).
The term "4D CT" is used in two distinct clinical contexts with different meanings for the "fourth dimension":
| Context | "4th Dimension" | Primary Use |
|---|---|---|
| Radiotherapy planning | Respiratory phase (time-resolved breathing cycle) | Tumor motion mapping |
| Parathyroid / functional imaging | Contrast enhancement over time (temporal perfusion) | Gland localization and characterisation |
| Cardiac / cerebrovascular | Cardiac cycle / temporal blood flow | Perfusion, flow dynamics |
2. Context A — 4D CT in Radiotherapy Planning (Respiratory Gating)
2.1 The Problem: Respiratory Motion
Lung and upper abdominal tumours move with breathing — sometimes by 10–20 mm in the superior-inferior direction. A standard 3D CT is a temporal snapshot: it may catch the tumour in any phase of the respiratory cycle, leading to:
- Motion blurring — averaging the tumour's position over time
- Inaccurate target delineation — the gross tumour volume (GTV) may be misrepresented
- Large safety margins — needed to ensure the tumour is always within the treatment field, but these irradiate healthy tissue unnecessarily
"Because lung tumors move significantly with respiratory motion, large margins were needed to ensure that a tumor was being appropriately treated." — Fishman's Pulmonary Diseases and Disorders
2.2 How 4D CT Solves This
4D CT acquires CT data continuously while simultaneously recording a respiratory surrogate signal (external bellows, spirometry, optical tracking of chest wall, or internal fiducial markers). After acquisition, the raw CT data is retrospectively sorted ("binned") into typically 8–10 phase bins representing stages of the respiratory cycle:
- 0% = end-expiration (or end-inspiration, depending on convention)
- 10%, 20% ... 90%, 100% = intermediate phases
Each bin contains a complete 3D volumetric CT dataset. The result is a cine loop of 3D volumes cycling through a full respiratory cycle — a "movie" of the tumour and surrounding anatomy.
Acquisition modes:
- Cine mode (axial): The table remains stationary at each position for one or more respiratory cycles while multiple axial images are acquired, then the table advances. Data are binned by phase retrospectively. This is the most common approach.
- Helical mode: Slow helical acquisition with low pitch, so that each anatomical location is sampled across multiple respiratory phases. Phase sorting is then applied.
2.3 Outputs and Their Uses
| Output | Description | Clinical Use |
|---|---|---|
| Phase images | Individual 3D volumes at each respiratory phase | Visualise tumour at each breathing stage |
| Average CT | Temporal average of all phases | Used as planning CT (reduces streaks) |
| Maximum Intensity Projection (MIP) | Max HU at each voxel across all phases | Maps full excursion of solid tumour/vessels |
| Minimum Intensity Projection (MinIP) | Min HU across all phases | Maps full excursion of lung air regions |
| Internal Target Volume (ITV) | Union of GTVs across all phases | Planning margin that encompasses full motion |
"Four-dimensional computed tomography (4D-CT) is now routinely used when performing CT simulation near the thorax and allows for visualization and accounting of a tumor's movement throughout a normal respiratory cycle." — Fishman's Pulmonary Diseases and Disorders
2.4 Respiratory Gating and Breath-Hold Techniques
4D CT enables:
- Respiratory gated radiotherapy (RGRT): The linear accelerator beam is triggered only when the tumour is within a defined gating window (e.g., end-expiration). This reduces treatment margins.
- Deep Inspiration Breath-Hold (DIBH): Patient breath-holds at maximum inspiration; the lung fills with air, displacing the heart away from chest wall tumours and reducing cardiac dose (especially in left-sided breast cancer and mediastinal lymphoma).
- Tumour tracking: Real-time tumour position fed back to the linac to continuously redirect the beam, even as the tumour moves.
2.5 Limitations in Radiotherapy
- Assumes periodic, reproducible breathing — arrhythmic or irregular breathing leads to artefacts (double-image artefacts, missing data)
- The 4D CT samples only ~5 seconds of breathing per anatomical level — a small sample of inter-fraction variability over a multi-week course of radiotherapy
- Higher radiation dose than a single 3D CT (proportional to number of phases acquired)
- 4D CBCT (cone-beam CT) extends this to on-treatment verification — the patient is imaged immediately before each radiotherapy fraction to confirm tumour position and motion
3. Context B — 4D CT in Parathyroid Imaging
This is the most common use of 4D CT outside of radiotherapy and has a very different technical basis.
3.1 Concept
Here, "4D" refers to three spatial dimensions + time (contrast enhancement kinetics). A multi-phase CT of the neck and upper chest is acquired at serial time points after intravenous contrast injection, capturing the differential contrast enhancement and washout pattern of parathyroid tissue relative to thyroid and lymph nodes.
"In 4D CT, the 'fourth dimension' reflects differential enhancement over time after contrast administration." — Sabiston Textbook of Surgery, 21st ed.
3.2 Protocol
A standard 4D CT parathyroid protocol includes:
| Phase | Timing | Finding |
|---|---|---|
| Non-contrast | Before injection | Parathyroid adenoma: hypodense vs thyroid (high iodine baseline) |
| Arterial phase | ~25–30 sec post-injection | Parathyroid adenoma: avid early enhancement (hypervascular) |
| Venous phase | ~50–60 sec | Adenoma begins to wash out |
| Delayed/washout phase | 60–80 sec | Adenoma: rapid washout (hypodense again); lymph nodes: minimal early uptake |
Coverage: axial, coronal, and sagittal reformats of the neck and upper chest (to capture ectopic mediastinal glands).
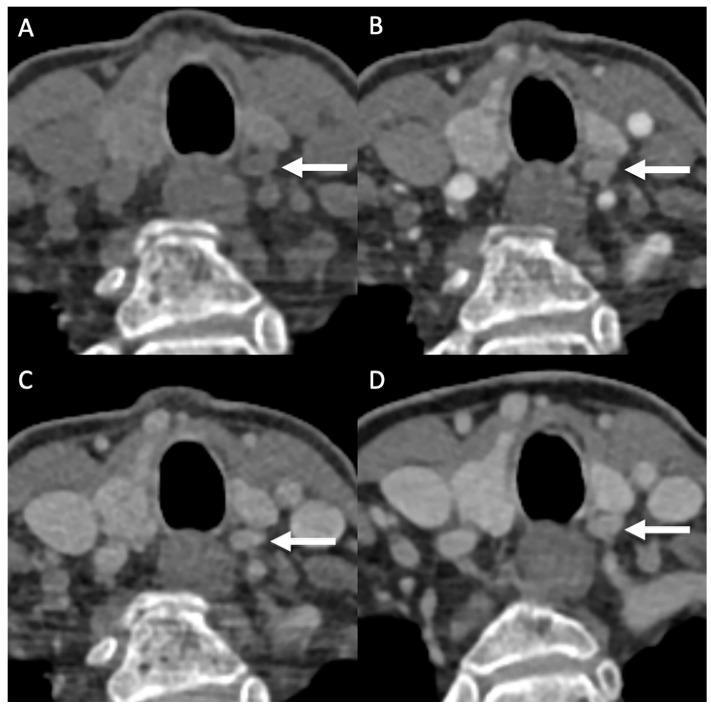
4D CT of a parathyroid adenoma (arrows): (A) non-contrast — hypodense nodule posterior to left thyroid, (B) arterial phase — intense rapid enhancement, (C) venous and (D) delayed phases — rapid washout. This kinetic pattern distinguishes parathyroid adenoma from thyroid tissue and lymph nodes.
3.3 Differential Enhancement Pattern
| Structure | Arterial phase | Washout phase |
|---|---|---|
| Parathyroid adenoma | Rapid, intense enhancement | Rapid washout (hypodense) |
| Thyroid gland | Moderate enhancement | Prolonged retention |
| Cervical lymph node | Minimal enhancement | Minimal |
This physiological "perfusion profile" is the basis for identification and localisation.
3.4 Performance
- Sensitivity: ~90% for parathyroid localisation — the most sensitive single modality
- Particularly valuable in:
- Failed prior surgical exploration
- Recurrent / persistent primary hyperparathyroidism (PHPT)
- Ectopic parathyroid glands (mediastinal, retro-oesophageal, intrathyroidal)
- Cases where ultrasound and sestamibi scintigraphy are discordant or negative
"4D CT is the most sensitive (90%) modality for parathyroid localization and is particularly useful in cases of failed prior exploration or recurrent disease." — Current Surgical Therapy, 14th ed.
3.5 Advantages Over Other Modalities
| Modality | Sensitivity | Notes |
|---|---|---|
| Ultrasound | 74–90% | Operator-dependent; cannot image ectopic mediastinal glands |
| Tc-99m sestamibi + SPECT | 90–97% | Poor anatomic detail; thyroid nodules cause false positives |
| 4D CT | ~90% | Superior anatomic detail; identifies ectopic glands; multiplanar reformats |
| MRI | Moderate | No radiation; poor sensitivity; reserved for reoperative cases |
| 11C-methionine PET/CT | High | Reserved for refractory cases |
3.6 Radiation Dose Consideration
- Overall radiation dose similar to sestamibi MIBI
- However, thyroid radiation dose ~50× higher with 4D CT than with MIBI (due to proximity of the thyroid to the neck CT field)
- Translates to estimated 0.1% lifetime absolute increase in thyroid cancer risk in a 20-year-old female — debatable clinical significance
"Preferential radiation to the thyroid is roughly fiftyfold higher with 4D CT than with MIBI. The clinical significance of this is debatable, however, because it translates to a lifetime absolute increase in thyroid cancer risk of 0.1% for a 20-year-old female." — Sabiston Textbook of Surgery
4. Context C — 4D CTA (Cerebrovascular / Neurovascular)
320-row detector CT systems (whole-brain coverage in one rotation) enable 4D CT angiography (4D CTA): repeated whole-volume acquisitions over time after a single contrast bolus, producing a temporal sequence of vascular fill images.
"CT with 320 detector rows enables dynamic scanning, providing both high spatial and temporal resolution of the entire cerebrovasculature (four-dimensional [4D] CTA)." — Bradley and Daroff's Neurology in Clinical Practice
Applications:
- Collateral circulation assessment in acute ischaemic stroke: identifies which patients benefit from thrombectomy even beyond standard time windows
- AVM nidus and draining vein mapping: temporal flow sequence shows arteriovenous shunting
- Dural arteriovenous fistula (dAVF): demonstrates early venous filling
- Aneurysm flow dynamics: pulsatility, flow direction within the sac
5. Context D — 4D CT Cardiac Perfusion
Dynamic (4D) CT myocardial perfusion imaging involves repeated CT acquisitions over the first pass of contrast through the myocardium to generate time-attenuation curves and quantify myocardial blood flow (MBF).
- Requires ≥256/320-row CT for whole-heart coverage in one rotation
- Static CT perfusion: single-phase acquisition with/without vasodilator stress
- Dynamic (4D) CT perfusion: full temporal sampling of contrast kinetics → quantitative MBF
Meta-analysis data: dynamic CT perfusion has higher sensitivity (0.85) but lower specificity (0.81) compared to static perfusion imaging (sensitivity 0.72, specificity 0.90). Its greatest limitation remains increased radiation dose and susceptibility to motion artefact.
6. Technical Considerations Common to All 4D CT
| Parameter | Consideration |
|---|---|
| Detector rows | ≥64 rows for most applications; 256/320 for cardiac/cerebrovascular whole-organ coverage |
| Temporal resolution | Determined by gantry rotation speed and acquisition interval between phases |
| Radiation dose | Higher than single 3D CT (multiple phase acquisitions); mitigated by dose modulation and iterative reconstruction |
| Data volume | Very large datasets; requires dedicated post-processing workstations |
| Artefacts | Motion artefacts at phase transitions; respiratory irregularity artefacts in respiratory-gated CT |
| Contrast timing | Precise injection rate and timing critical for arterial/venous/washout phases |
7. Summary Table
| Application | "4th Dimension" | Key Technology | Primary Output | Main Clinical Indication |
|---|---|---|---|---|
| Radiotherapy 4D CT | Respiratory phase | Cine/helical + phase binning | ITV, motion maps, gated plans | Thoracic/upper abdominal tumour RT planning |
| Parathyroid 4D CT | Contrast kinetics | Multi-phase neck CT | Enhancement/washout maps | PHPT localisation pre-surgery |
| 4D CTA (brain) | Blood flow over time | 320-row CT + repeated scans | Temporal angiographic sequence | Stroke collaterals, AVM, aneurysm |
| 4D cardiac CT | Cardiac cycle + perfusion | High-temporal-res CT | MBF quantification | Myocardial ischaemia assessment |
Sources: Fishman's Pulmonary Diseases and Disorders, 5th ed.; Current Surgical Therapy, 14th ed.; Sabiston Textbook of Surgery, 21st ed.; Bradley & Daroff's Neurology in Clinical Practice; Grainger & Allison's Diagnostic Radiology; Bailey & Love's Short Practice of Surgery, 28th ed.
Protocols for adult whole body ct
Finding Sources
Finding Sources
Searching the Web
adult whole body CT scan protocol parameters contrast phases radiology technique
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
MDCT whole body CT protocol scan parameters kVp mAs pitch slice thickness reconstruction kernel 2024
Finding Sources
Finding Sources
Reading Web Page
https://radiologyassistant.nl/more/ct-protocols/ct-contrast-…
Reading File
Reading File
Finding Sources
Reading File
Searching the Web
whole body CT polytrauma trauma protocol non-contrast arterial portal venous phases indications site coverage
I now have comprehensive information from textbooks, protocol PDFs, and clinical guidelines. Let me compile the full answer.
Protocols for Adult Whole-Body CT
"Whole-body CT" (WBCT) is not a single fixed protocol — it refers to any CT examination covering head to pelvis (or skull vertex to proximal femora). The protocol design depends entirely on the clinical indication. The major categories are:
- Polytrauma / Pan-scan — emergency
- Oncology staging / restaging — Chest-Abdomen-Pelvis (CAP) ± head
- CT Angiography (WBCTA) — vascular mapping
- Low-dose screening — general health check
1. Patient Preparation
| Item | Details |
|---|---|
| Fasting | Nil by mouth 4 hours before for elective contrast studies (minimises aspiration risk and nausea); not applicable in trauma |
| Oral contrast | Positive (dilute iodine/barium): delineates bowel; given 60–90 min before scan. Negative (water, ~500 ml): used in CT enterography, rectal cancer staging. Often omitted in modern oncology protocols for speed |
| IV access | 18–20 gauge antecubital vein minimum; 16–18G preferred for high-rate injections (CT angiography) |
| Creatinine / eGFR | Check before elective contrast: avoid IV contrast if eGFR <30 mL/min/1.73 m² (relative) or <15 mL/min (absolute) without dialysis cover |
| Allergy history | Previous contrast reactions, asthma, seafood allergy: pre-medicate (steroids + antihistamine) or use alternative modality |
| Metformin | Withhold 48 hours after IV contrast in patients with renal impairment |
| Positioning | Supine, arms elevated (reduces beam-hardening artefact through thorax/abdomen); feet-first orientation |
| Breath-hold instruction | Verbal coaching for inspiration hold during thoracic acquisition; suspended respiration for abdominal series |
2. Core Technical Parameters
2.1 Scanner Requirements
Modern WBCT requires at minimum a 64-detector row MDCT scanner to cover the entire body in a single breath-hold with sub-millimetre collimation. 128-, 256- and 320-row systems offer faster coverage and better temporal resolution for multiphasic and vascular studies.
2.2 Acquisition Parameters
| Parameter | Typical Value | Rationale |
|---|---|---|
| Tube voltage (kVp) | 120 kVp standard adult; 100 kVp in thin patients (<60 kg); 80 kVp for CTA with contrast | Lower kVp increases contrast-to-noise ratio for iodine (enhances vessels/organs), reduces dose in lean patients |
| Tube current (mA) | Automatic (AEC / tube current modulation) | Adjusts to patient diameter and anatomy; prevents unnecessary dose in thin sections |
| Effective mAs | 100–300 mAs depending on region and body habitus | |
| Rotation time | 0.5–0.8 sec | Faster reduces cardiac/pulsation artefact |
| Detector collimation | 0.5–0.625 mm (64 × 0.625 mm or 128 × 0.6 mm) | Enables isotropic sub-millimetre voxels |
| Pitch | 0.6–1.5 | Lower pitch = more overlap = better z-resolution but higher dose; higher pitch = faster scan, lower dose |
| Reconstruction slice thickness | Axial display: 3–5 mm; thin series for MPR/3D: 0.75–1.5 mm | Thin slices stored for post-processing; thicker displayed for reading |
| Reconstruction kernel/filter | Soft tissue (e.g., B30f, B/C/D series): abdomen/mediastinum; Lung (e.g., B60f): pulmonary parenchyma; Bone (e.g., B70f): skeletal detail | |
| Iterative reconstruction | ASIR-V, SAFIRE, AIDR 3D, DLIR (deep learning) at 40–60% blend | Reduces noise by 30–50%, allowing 30–50% dose reduction |
| Display FOV | Set to patient body size (not table FOV) to maximise resolution |
2.3 Dose Reduction Strategies
"There are many available strategies to reduce radiation exposure; these include the use of size-dependent protocols, automated tube current modulation, reduction of the number of passes, reduction in duplicate coverage, reduction of mAs and kVp where possible, optimisation of IV contrast medium administration and the possible use of external shielding." — Grainger & Allison's Diagnostic Radiology
| Strategy | Effect |
|---|---|
| Automatic exposure control (AEC) | Adjusts mA to patient size and anatomy in real time |
| Low kVp (80–100 kV) | Reduces dose; increases contrast enhancement of iodine |
| Iterative / deep-learning reconstruction | 30–50% dose reduction for equivalent image quality |
| Limit phases scanned | Each additional phase multiplies dose proportionately |
| Eliminate duplicate coverage | Coordinate field overlap between thoracic and abdominal acquisitions |
| Higher pitch where compatible | Reduces scan time and dose if effective mAs is not pitch-compensated |
| Organ-based tube current modulation | Reduces dose to breast, thyroid, lens |
Typical effective doses:
- Chest CT: ~5–7 mSv
- Abdomen-pelvis CT: ~8–12 mSv
- Full WBCT (head to pelvis, single phase): ~15–25 mSv
- Multiphasic WBCT (e.g., non-contrast + arterial + portal venous): ~25–40 mSv
3. Contrast Medium Administration
3.1 Contrast Types
- Non-ionic iodinated contrast (e.g., ioversol 350, iohexol 300/350, iomeprol 400): standard for CT
- Concentration: higher concentration (350–400 mg I/mL) preferred for angiography; 300 mg I/mL adequate for most body CT
- Volume: weight-based dosing: 1.5–2 mL/kg (max 150 mL); or fixed 100–150 mL for CTA; 80–100 mL for standard CAP
3.2 Injection Rate and Access
| Indication | IV Gauge | Rate | Volume |
|---|---|---|---|
| Standard CAP (oncology) | 18–20G | 2–3 mL/sec | 80–100 mL |
| CTA chest/aorta | 18G | 4–5 mL/sec | 100–150 mL |
| Liver lesion characterisation | 18G | 4–5 mL/sec | 100–150 mL |
| Trauma WBCT | 18G min | 3–4 mL/sec | 100–150 mL |
- Always followed by 50 mL saline flush at the same rate to push contrast bolus through the dead space of tubing and arm veins, improving arterial peak enhancement
3.3 Bolus Timing Methods
| Method | Description | Use |
|---|---|---|
| Fixed delay | Scan starts at predetermined time post-injection | Simple; less accurate for vascular phases |
| Bolus tracking (SmartPrep / CARE Bolus) | ROI placed on aorta/vessel; scan triggered when HU exceeds threshold (100–150 HU) | Standard for CTA and arterial phase |
| Test bolus | 15–20 mL test injection with serial monitoring of ROI attenuation to time peak enhancement | Used when precise arterial timing is critical |
4. Enhancement Phases and Timing
This is the most clinically important element of whole-body CT protocol design.
| Phase | Timing Post-Injection | What Is Enhanced | Primary Indications |
|---|---|---|---|
| Non-contrast (NECT) | Before injection | Calcification, haemorrhage, iodine-based lesion baseline | Calculi, haematoma, adrenal adenoma, liver steatosis |
| Early arterial | 18–25 sec | Arteries (pure vascular fill) | CT angiography (aorta, pulmonary arteries, carotids) |
| Late arterial / hepatic arterial | 30–40 sec | Hypervascular lesions, arteries + early liver enhancement | HCC, carcinoid, pancreatic neuroendocrine tumours |
| Portal venous (PV) | 60–75 sec | Liver parenchyma, portal veins, spleen, bowel wall | Standard abdominal oncology; metastases; bowel pathology |
| Nephrographic | 80–120 sec | Renal parenchyma uniform enhancement | Renal masses, papillary RCC |
| Delayed / equilibrium | 3–10 min | Fibrotic/desmoplastic lesions retain contrast | Cholangiocarcinoma, peritoneal disease, bladder |
| Urographic / excretory | 5–15 min | Collecting systems, ureters, bladder opacified | CT urography, urothelial malignancy |
"Hypovascular lesions like metastases, cysts and abscesses will not enhance and are best seen in the hepatic phase at 70 sec; fibrotic lesions like cholangiocarcinoma hold contrast longer and are best seen in the delayed phase at 600 sec." — Radiology Assistant (CT Contrast Injection and Protocols)
5. Region-Specific Protocols Within Whole-Body CT
5.1 Head
| Setting | Phase | Slice/Recon |
|---|---|---|
| Trauma, screen | Non-contrast | 5 mm axial brain; 2 mm bone |
| Ischaemic stroke | NECT + CTP + CTA | NECT first, then CTP (whole brain), then CTA skull base to vertex |
| Oncology staging (brain mets) | Post-contrast T1-equivalent CECT | 3 mm with MPR; or MRI preferred |
5.2 Neck
- Post-contrast, 3 mm slices from skull base to sternal notch
- Soft tissue + bone reconstructions
- Arterial phase if CTA carotids requested (bolus-tracked off common carotid)
5.3 Chest (Thorax)
| Indication | Phase | kVp | Notes |
|---|---|---|---|
| Oncology staging | Portal venous (60–70 sec) | 120 | Arms up; inspiration breath-hold |
| PE (CTPA) | Arterial (15–20 sec from trigger at pulmonary artery) | 100–120 | Bolus-tracked at main pulmonary artery |
| Aortic dissection | Arterial (aortic arch trigger) + delayed | 100–120 | Non-contrast useful to show intramural haematoma |
| Lung nodule / LDCT screen | Single-pass NECT | 100–120 kVp, very low mAs (20–40 mAs) | No contrast; lung kernel; deep inspiration |
| Empyema/mediastinitis | Post-contrast PV phase | 120 | Pleural enhancement assessed |
Reconstructions — chest:
- 3–5 mm axial (soft tissue + mediastinum)
- 1.25 mm thin axial stored
- Coronal and sagittal 3 mm MPR
- 1.5 mm axial MIP (7 mm slab) for pulmonary nodules
- Lung window: 1.5 mm axial for parenchyma
5.4 Abdomen and Pelvis
Standard oncology CAP (most common whole-body CT):
- Portal venous phase (65–75 sec)
- Arms raised; 3 mm axial, 3 mm coronal and sagittal
- Includes liver, spleen, pancreas, kidneys, adrenals, bowel, pelvic organs
Liver protocol (2- or 3-phase):
- NECT — baseline
- Late arterial (35 sec) — hypervascular lesions
- Portal venous (70 sec) — background liver enhancement, hypovascular mets
Pancreatic protocol:
- NECT
- Late arterial (40–45 sec, pancreatic phase) — pancreatic parenchyma maximally enhances; ductal adenocarcinoma is hypovascular
- Portal venous (70 sec)
Renal / CT urography (3-phase):
- NECT — calculi, adrenal, baseline
- Nephrographic (90–120 sec) — renal masses
- Excretory/urographic (5–10 min) — urothelial filling; can use split-bolus technique to combine phases 2 and 3 in a single acquisition (dose reduction)
6. Whole-Body CT in Polytrauma (Pan-Scan)
The "pan-scan" (WBCT from skull vertex to proximal femora with IV contrast) has become standard in major trauma centres for haemodynamically stable or transiently stabilised severely injured patients.
Indications for Trauma WBCT
- Altered vital signs (GCS ≤13, SBP <90 mmHg, RR <10 or >29)
- High-energy mechanism: MVC >60 km/h, ejection, fall >3 m
- Penetrating injury to trunk
- Fractures of ≥2 long bones
- Clinical suspicion of multi-region injury
- Transfer from another hospital with incomplete workup
(ESER Society Guideline on Radiological Polytrauma Imaging, 2020)
Trauma WBCT Protocol
Option A — Split-bolus (time-optimised, fewer phases):
- Single IV bolus → timed so that arterial and portal venous phases of the abdomen coincide in one acquisition
- Chest in arterial phase (25–35 sec)
- Abdomen-pelvis in portal venous phase (60–75 sec)
- Total scan time: ~45–90 seconds on a 64-row scanner
Option B — Multiphasic (preferred for haemodynamically unstable, suspicion of active bleeding):
| Series | Coverage | Phase | Timing |
|---|---|---|---|
| 1. NECT | Head | Non-contrast | — |
| 2. NECT | Cervical spine | Non-contrast | — |
| 3. CTA | Chest + abdomen + pelvis | Arterial (bolus-tracked at aortic arch, trigger 100–150 HU) | ~25–35 sec |
| 4. CECT | Abdomen + pelvis | Portal venous | ~65–75 sec |
- Arterial phase: identifies active arterial haemorrhage (extravasation of contrast), vascular injuries
- Portal venous phase: delineates organ parenchymal injuries, quantifies haematoma extent, differentiates contained vs. active bleeding
"The arterial phase allows the integrity of the arterial vascular system and the arterial origin of a bleed to be assessed. The venous phase shows enhancement of organ parenchyma and the amount of bleeding — differentiating lesions with contained bleeding from those with active bleeding, which is crucial for subsequent treatment." — European Review (Optimization of CT Protocol in Polytrauma Patients)
Reconstructions — trauma WBCT:
- Head: 5 mm axial + 2 mm bone
- C-spine: 2 mm axial, 2 mm coronal, 2 mm sagittal (bone kernel)
- Chest: 3 mm axial (soft tissue), 1.5 mm axial (lung kernel), 3 mm MPR
- Abdomen/pelvis: 3 mm axial, 3 mm coronal, 3 mm sagittal
- All phases reformatted in 3 planes
7. CT Angiography (CTA) Whole-Body / Aorta
Used for aortic dissection, aortic aneurysm surveillance, peripheral arterial disease.
| Phase | Timing | Coverage |
|---|---|---|
| NECT (optional) | Before contrast | Assess intramural haematoma, calcification |
| Arterial | Bolus-tracked (trigger 150 HU at aortic arch) | Skull base to femoral bifurcation |
| Delayed (optional) | 3–5 min | Endoleak detection post-EVAR; slow bleed |
- Rate: 4–5 mL/sec, 120–150 mL, 18G
- Thin reconstructions: 1 mm axial; MIP coronal + sagittal; 3D volume rendering
- kVp: 100 or 80 (reduces dose; iodine conspicuity increases at lower kVp)
8. Whole-Body Low-Dose CT (Screening)
For lung cancer screening and general health screening programmes:
| Parameter | Value |
|---|---|
| Coverage | Skull vertex to proximal femora or chest only (lung screening) |
| kVp | 100–120 |
| mAs | Very low: 20–40 mAs (chest); 50–80 mAs (abdomen) |
| Reconstruction | Deep learning or model-based iterative (essential at low dose) |
| Contrast | None (NECT only) |
| Indications | Lung cancer: 55–80 yo, ≥20 pack-year smoking history (USPSTF/NLST criteria) |
9. Reconstruction and Post-Processing — Summary
All whole-body CT examinations should routinely produce:
| Reconstruction | Slice | Use |
|---|---|---|
| Axial soft tissue | 3–5 mm | Primary reading |
| Axial bone | 1–2 mm | Skeletal detail, C-spine |
| Axial lung | 1.5 mm (high-frequency kernel) | Pulmonary parenchyma |
| Thin axial (stored) | 0.625–1.25 mm | 3D post-processing, MPR |
| Coronal MPR | 3 mm | Standard for abdominal, chest |
| Sagittal MPR | 3 mm | Spine, mediastinum, aorta |
| Coronal/sagittal MIP | 7–10 mm slab | Vascular, nodule detection |
| 3D volume rendering | As needed | CTA, skeletal, surgical planning |
10. Summary Protocol Table
| Indication | Phases | Coverage | Rate | Timing |
|---|---|---|---|---|
| Oncology staging (CAP) | PV only | Skull base → pelvis | 2–3 mL/sec | 65–75 sec |
| Liver/pancreas characterisation | NECT + arterial + PV | Abdomen ± chest | 4–5 mL/sec | 35 sec + 70 sec |
| CT urography | NECT + nephrographic + urographic | Abdomen + pelvis | 3 mL/sec | 90 sec + 10 min |
| CTPA (pulmonary embolism) | Arterial | Chest | 4–5 mL/sec | Bolus-tracked at pulmonary trunk |
| Aortic dissection | NECT + arterial + delayed | Chest + abdomen + pelvis | 4–5 mL/sec | Bolus-tracked at aortic arch |
| Polytrauma (stable) | Arterial + PV | Head + C-spine + CAP | 3–4 mL/sec | 25–35 sec / 65–75 sec |
| Polytrauma (unstable) | Arterial + PV (multiphasic) | Head + spine + CAP | 4 mL/sec | Bolus-tracked |
| Lung cancer screening | NECT (low-dose) | Chest only | None | — |
Sources: Grainger & Allison's Diagnostic Radiology; Fishman's Pulmonary Diseases and Disorders; Radiology Assistant — CT Contrast Injection and Protocols; ESER Society Guideline on Radiological Polytrauma Imaging (2020); AAPM CT Protocol Optimization; Radiology of Indiana CT Protocols; BC Trauma Standard Imaging Protocols.
This is a shared conversation. Sign in to Orris to start your own chat.