Give me a full notes on liver cirrhosis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"liver cirrhosis"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content across all key domains. Let me compile the full, well-structured notes on liver cirrhosis.
Liver Cirrhosis — Comprehensive Notes
1. Definition
Cirrhosis is the diffuse transformation of the entire liver into regenerative parenchymal nodules surrounded by fibrous bands, representing the final common pathway of a wide variety of chronic liver diseases. It is a pathologic entity defined by:
- Diffuse hepatic fibrosis
- Replacement of normal liver architecture by nodules (both regenerative and fibrotic)
- Disruption of vascular relationships
Cirrhosis is not a specific diagnosis — it has variable prognostic implications depending on etiology, stage, and response to therapy. Regression of fibrosis (and even of established cirrhosis) may occur with disease remission or cure.
Gross appearance: The liver surface is covered with bulging regenerative nodules separated by broad scars.

2. Etiology / Causes
| Category | Specific Causes |
|---|---|
| Alcohol | Alcohol-associated liver disease (~48% of cirrhosis deaths in USA) |
| Viral | Chronic Hepatitis B, Chronic Hepatitis C |
| Metabolic | MASLD/NAFLD/NASH (metabolic dysfunction-associated steatotic liver disease) |
| Biliary | Primary biliary cholangitis (PBC), Primary sclerosing cholangitis (PSC), biliary obstruction |
| Autoimmune | Autoimmune hepatitis |
| Vascular | Cardiac cirrhosis (right heart failure), Budd-Chiari syndrome |
| Metabolic/Genetic | Hemochromatosis, Wilson's disease, α1-antitrypsin deficiency |
| Drugs/Toxins | High-dose vitamin A, methotrexate |
| Cryptogenic | No clear cause identified (~5–10% of cases) |
Alcohol-associated cirrhosis = micronodular (<3 mm). With cessation of alcohol, larger nodules may form → mixed micro- and macronodular.
3. Pathogenesis
Key Cellular Players
Hepatic stellate cell (HSC) is the principal cell responsible for fibrosis:
- Normally a pericyte in the Space of Dissé (abluminal to sinusoidal endothelium)
- Upon activation → transforms into myofibroblast
- Characterized by: ↑ smooth muscle actin expression, ↑ motility/contractility, collagen type 1 production
- Earliest matrix product = fibronectin, then collagen type 1
- Activating pathways: PDGF, TGF-β, integrin signaling
Other contributing cells:
- Portal fibroblasts → implicated in biliary forms of injury (PBC, PSC)
- Kupffer cells (macrophages) → release profibrogenic cytokines → activate stellate cells; some subclasses promote fibrosis, others resolve it
- Hepatocytes → epithelial cell injury (apoptosis, necrosis, inflammation) is the initiating event
Fibrosis Cascade (simplified)
Hepatocyte injury → Kupffer cell activation → cytokine release (TGF-β, PDGF)
→ Stellate cell activation → myofibroblast transformation
→ Collagen/ECM deposition → progressive fibrosis → nodule formation
→ Disruption of vascular architecture → CIRRHOSIS
Alcohol-Specific Mechanism
- Ethanol → ADH → acetaldehyde (highly reactive)
- Also via CYP2E1 (MEOS) → reactive oxygen species (ROS)
- Acetaldehyde adducts interfere with microtubule formation and protein trafficking
- ROS → Kupffer cell activation → stellate cell activation → collagen production
- Fatty acid oxidation ↓, lipoprotein secretion ↓ → steatosis
- Fibrosis: centrilobular, pericellular, or periportal → connects portal triads to central veins
4. Morphology
Gross
- Entire liver replaced by regenerative nodules separated by fibrous septa
- Surface nodularity easily visible
- Liver may be enlarged (early) or shrunken/small (late)
- Nodule size varies: micronodular (<3 mm, e.g., alcoholic) vs. macronodular (>3 mm, e.g., viral)
Microscopic
- Fibrous bands linking portal tracts to each other OR portal tracts to central veins
- Regenerative nodules surrounded by fibrosis
- Ductular reactions (stem cell-derived ductlike structures) increase with disease progression, most prominent in cirrhosis
- Variable degrees of parenchymal loss and vascular thrombosis (especially portal vein)
Reversibility
- Regression of fibrosis may follow disease remission/cure
- Scars become thinner, compact, then fragment
- Adjacent nodules coalesce into larger parenchymal islands
- All cirrhotic livers show elements of both progression and regression
5. Clinical Features
Compensated Cirrhosis (~40% asymptomatic)
- Often discovered incidentally on imaging, labs, or endoscopy
- Nonspecific: fatigue, weight loss, ↓ muscle mass, ↓ libido, sleep disturbances
- ~40% have esophageal varices (asymptomatic if not bleeding)
- Normal/near-normal liver synthetic function
Decompensated Cirrhosis (signs of organ failure)
- Ascites (most frequent sign of decompensation — present in 80%)
- Variceal hemorrhage
- Hepatic encephalopathy
- Jaundice
Physical Examination Findings
| Sign | Mechanism |
|---|---|
| Jaundice | ↓ bilirubin conjugation/excretion |
| Spider angiomata | ↑ estrogen, arteriovenous shunting |
| Palmar erythema | ↑ estrogen |
| Gynecomastia, testicular atrophy | ↑ estrogen (impaired hepatic metabolism) |
| Leukonychia (white nails) | Hypoalbuminemia |
| Clubbing | Hypoxia (hepatopulmonary syndrome) |
| Caput medusae | Portosystemic collaterals |
| Splenomegaly | Portal hypertension → hypersplenism |
| Dupuytren's contracture | Associated with alcohol use |
| Pruritus | Cholestasis — bile salt accumulation |
| Asterixis (flap) | Hepatic encephalopathy |
| Muscle wasting / sarcopenia | Malnutrition, hyperammonemia |
| Fetor hepaticus | Exhaled mercaptans |
6. Complications
Framework
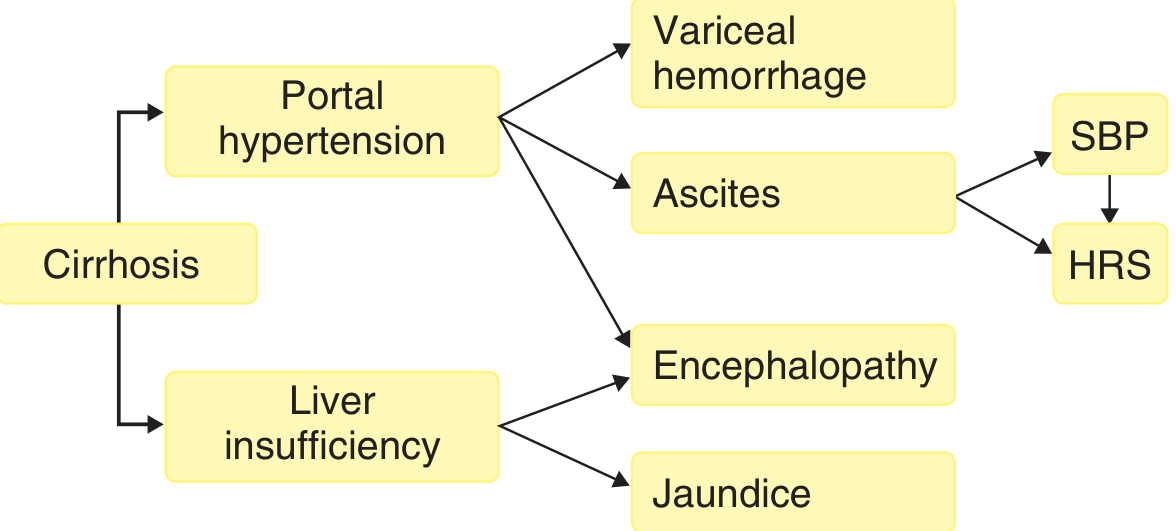
A. Portal Hypertension
- HVPG (Hepatic Venous Pressure Gradient) >10–12 mmHg → varices develop
- HVPG >12 mmHg → risk of variceal bleeding
- Mechanisms:
- Fixed component: fibrous tissue + nodule compression of sinusoids
- Functional component: intrahepatic NO deficiency → vasoconstriction
- Paradox: intrahepatic NO ↓ (vasoconstriction) but extrahepatic NO ↑ (splanchnic vasodilation)
- Splanchnic vasodilation → ↑ portal inflow → maintains portal hypertension
- Systemic vasodilation → ↓ effective arterial volume → RAAS activation → Na/water retention → hyperdynamic circulation
B. Varices and Variceal Hemorrhage
- Present in ~50% of newly diagnosed cirrhosis
- Prevalence: Child A 40% → Child C 85%
- Growth rate: 7–8%/year; small varices bleed ~5%/year; large varices ~15%/year
- Predictors of hemorrhage: large varices, severe liver disease (Child C), red wale markings
- Manifestation: hematemesis, melena, or both
- Diagnosis: upper GI endoscopy (active bleed, white nipple sign, clot on varix, or varices as only source)
C. Ascites
- Most common cause of decompensation; 80% of decompensated patients
- Rate of development: 7–10%/year in compensated cirrhosis
- Pathophysiology: Sinusoidal portal hypertension → splanchnic vasodilation → ↓ effective arterial volume → RAAS activation → Na/water retention
- SAAG (Serum-Ascites Albumin Gradient):
| Condition | SAAG | Ascites protein |
|---|---|---|
| Cirrhosis | High (>1.1 g/dL) | Low |
| Cardiac ascites | High | High |
| Malignant/TB ascites | Low | High |
- Paracentesis mandatory for new-onset ascites: check albumin, total protein, PMN count, culture, cytology
D. Spontaneous Bacterial Peritonitis (SBP)
- Ascites PMN count ≥250 cells/mm³ = diagnostic
- Most common organisms: E. coli, Klebsiella, Streptococcus pneumoniae
- Treatment: 3rd generation cephalosporins (e.g., cefotaxime)
- Prophylaxis: norfloxacin in high-risk patients
- Associated with 4-fold ↑ mortality
E. Hepatic Encephalopathy (HE)
- Results from portosystemic shunting + liver insufficiency → ↑ ammonia and other toxins reach brain
- Grades I–IV (West Haven criteria)
- Precipitants: GI bleed, infection, dehydration, constipation, electrolyte disturbance, sedatives
- Treatment: lactulose (reduces ammonia), rifaximin (non-absorbable antibiotic)
F. Hepatorenal Syndrome (HRS)
- Functional renal failure in advanced cirrhosis — no intrinsic kidney disease
- Type 1 (now HRS-AKI): rapid onset, sCr doubles to >2.5 mg/dL in <2 weeks
- Type 2 (now HRS-CKD): gradual, associated with refractory ascites
- Mechanism: extreme splanchnic vasodilation → renal vasoconstriction
- Treatment: terlipressin + albumin (preferred); norepinephrine + albumin; TIPS; liver transplant
G. Hepatopulmonary Syndrome
- Intrapulmonary vascular dilation → hypoxemia
- Classic: platypnea (SOB worse upright, better supine), orthodeoxia
- Diagnosis: contrast echocardiography (bubble test), 99mTc-MAA scan
H. Portopulmonary Hypertension
- Pulmonary arterial hypertension in setting of portal hypertension
- Diagnosis: right heart catheterization (mPAP ≥25 mmHg)
I. Hepatocellular Carcinoma (HCC)
- Can develop at any stage of cirrhosis; accelerates course
- Annual risk ~2–4% in cirrhotic patients
- Surveillance: liver ultrasound every 6 months ± AFP
J. Other Complications
- Hepatic hydrothorax: transdiaphragmatic movement of ascites → pleural effusion (usually right-sided)
- Cirrhotic cardiomyopathy: impaired cardiac contractile response to stress
- Coagulopathy: ↓ synthesis of clotting factors (II, V, VII, IX, X)
- Thrombocytopenia: hypersplenism, ↓ thrombopoietin
- Hyponatremia: dilutional (water retention > sodium)
- Osteoporosis: especially in cholestatic disease
- Hypogonadism, adrenal insufficiency, malnutrition
7. Diagnosis
Laboratory Tests
| Test | Finding in Cirrhosis |
|---|---|
| ALT/AST | Mildly elevated or normal (late cirrhosis — few hepatocytes left) |
| ALP, GGT | Elevated (especially biliary cirrhosis) |
| Bilirubin | Elevated (conjugated and unconjugated) |
| Albumin | ↓ (best marker of synthetic function) |
| PT/INR | Prolonged (↓ clotting factor synthesis) |
| Platelets | ↓ (hypersplenism) |
| Sodium | ↓ (dilutional hyponatremia) |
| Creatinine | ↑ in HRS |
| CBC | Pancytopenia from hypersplenism |
Imaging
- Ultrasound (US): Heterogeneous echogenicity, nodular surface, splenomegaly, ascites, collateral vessels — first-line
- CT scan: Nodular liver contour, varices, splenomegaly, HCC detection
- MRI/MRCP: Better soft tissue detail; useful for HCC characterization
- Transient Elastography (FibroScan): Liver stiffness >14 kPa suggests cirrhosis; >21 kPa associated with portal hypertension; <19.5 kPa — varices unlikely
- ARFI elastography: >2.6 m/sec suggests cirrhosis
- MR Elastography (MRE): Stiffness >5.9 kPa suggests cirrhosis; liver biopsy often not required
Liver Biopsy
- Gold standard for confirming cirrhosis and assessing fibrosis stage
- Required when non-invasive tests are inconclusive
- Contraindicated with significant coagulopathy (use transjugular approach)
- Fibrosis staging: Metavir F0–F4 (F4 = cirrhosis)
Non-invasive Fibrosis Markers
- FIB-4 index = (age × AST) / (platelets × √ALT)
- APRI score
- Commercial panels (FibroTest, ELF test)
- Useful for distinguishing early from late fibrosis, but not individual stages
8. Staging / Prognostic Scoring
Child-Pugh Score (Child-Turcotte-Pugh)
| Parameter | 1 point | 2 points | 3 points |
|---|---|---|---|
| Bilirubin (mg/dL) | <2 | 2–3 | >3 |
| Albumin (g/dL) | >3.5 | 2.8–3.5 | <2.8 |
| PT prolongation (sec) / INR | <4 / <1.7 | 4–6 / 1.7–2.3 | >6 / >2.3 |
| Ascites | None | Mild | Moderate–Severe |
| Encephalopathy | None | Grade 1–2 | Grade 3–4 |
| Class | Score | 1-year survival | 2-year survival |
|---|---|---|---|
| A (compensated) | 5–6 | 100% | 85% |
| B | 7–9 | 80% | 60% |
| C (decompensated) | 10–15 | 45% | 35% |
- Class B (score ≥7) = traditional criterion for liver transplant listing
- Class A = "compensated cirrhosis"
MELD Score (Model for End-Stage Liver Disease)
Formula:
MELD = 3.78 × ln[bilirubin mg/dL] + 11.2 × ln[INR] + 9.57 × ln[creatinine mg/dL] + 6.43- Uses: INR, bilirubin, creatinine
- Modified as MELD-Na (incorporates serum sodium) for better mortality prediction
- Current standard for liver transplant organ allocation in the USA (replaced Child-Pugh)
- Higher score = higher 90-day mortality on transplant waiting list
- Online calculator: OPTN MELD calculator
PELD Score
- Used for pediatric patients (<12 years)
9. Natural History
- Compensated → Decompensated: ~5–7% per year
- Median time to decompensation: ~6 years from diagnosis
- 10-year probability of decompensation from compensated state: 58%
- Annual decompensation rate by etiology:
- HCV-related: 4%/year
- Alcohol-related: 6–10%/year (higher if actively drinking)
- HBV-related: 10%/year
Survival
- Compensated cirrhosis: median survival 9–12 years
- Decompensated cirrhosis: median survival ~2 years
- Overall 5-year survival: ~38%; 10-year: ~22% (Danish population study)
- Patients with infection: 4× ↑ mortality
- Patients with renal failure: 7–8× ↑ mortality
10. Treatment
General Principles
- Treat the underlying cause (most important to slow/reverse fibrosis):
- HCV → direct-acting antivirals (cure possible → regression of fibrosis)
- HBV → nucleos(t)ide analogs (entecavir, tenofovir)
- Alcohol → abstinence (mandatory)
- MASLD/NASH → weight loss, metabolic control
- PBC → ursodeoxycholic acid (UDCA) 13–15 mg/kg/day
- Autoimmune hepatitis → corticosteroids ± azathioprine
- Hemochromatosis → phlebotomy
- Wilson's disease → penicillamine / trientine
Compensated Cirrhosis Management
- HCC surveillance: Liver US ± AFP every 6 months
- Variceal screening: Upper endoscopy at diagnosis; repeat every 1–3 years if no varices
- Non-selective beta-blockers (propranolol, nadolol, carvedilol) for medium/large varices — reduce portal pressure
- Endoscopic band ligation (EBL): Primary prophylaxis for large varices
- Immunizations: HAV, HBV, pneumococcal, influenza, COVID-19
- Statins: Use in chronic viral hepatitis → reduced risk of decompensation and mortality
- Avoid NSAIDs, aminoglycosides
- Acetaminophen ≤2 g/day acceptable
- Alcohol abstinence
- Weight loss reduces portal pressure
Decompensated Cirrhosis Management
Ascites
- Grade 1 (mild): Sodium restriction (<2 g/day)
- Grade 2 (moderate): Spironolactone (100–400 mg/day) ± furosemide (40–160 mg/day)
- Grade 3 (large/tense): Large-volume paracentesis (LVP) + IV albumin (6–8 g per liter removed)
- Refractory ascites: TIPS (transjugular intrahepatic portosystemic shunt) or repeated LVP
Variceal Hemorrhage
- Acute bleeding:
- IV terlipressin (preferred) or octreotide/somatostatin
- Endoscopic band ligation (EBL) within 12 hours
- IV antibiotics (ceftriaxone) — reduce risk of SBP and improve survival
- Consider early TIPS (pre-emptive TIPS) in Child C patients
- Secondary prophylaxis: NSBB + EBL (combination)
- Primary prophylaxis (large varices): NSBB or EBL
Hepatic Encephalopathy
- Identify and treat precipitants
- Lactulose — titrate to 2–3 soft stools/day
- Rifaximin 550 mg BID — secondary prophylaxis; reduces recurrence by ~58%
- Adequate protein intake (1.2–1.5 g/kg/day; do NOT restrict protein)
- BCAA supplements in refractory cases
Spontaneous Bacterial Peritonitis
- IV cefotaxime 2 g q8h × 5 days
- IV albumin 1.5 g/kg on day 1, 1 g/kg on day 3 → prevents HRS
- Long-term prophylaxis: norfloxacin 400 mg/day or trimethoprim-sulfamethoxazole
Hepatorenal Syndrome
- Terlipressin + albumin (1st line where available)
- Norepinephrine + albumin (in ICU setting)
- Discontinue diuretics, nephrotoxins
- TIPS as bridge; liver transplantation = definitive treatment
Liver Transplantation
- Definitive therapy for end-stage cirrhosis
- Indications: MELD ≥15, Child-Pugh class B/C, refractory complications
- Contraindications: active alcohol/substance use (usually requires 6-month sobriety), extrahepatic malignancy, severe cardiopulmonary disease
- 5-year post-transplant survival: ~70–80%
- Milan criteria for HCC: single nodule ≤5 cm OR up to 3 nodules ≤3 cm, no vascular invasion, no extrahepatic spread
Acute-on-Chronic Liver Failure (ACLF)
- Defined as acute decompensation of cirrhosis with organ failure
- Precipitants: bacterial infection, GI bleeding, alcohol-associated hepatitis, reactivation of HBV
- Management: treat precipitant, organ support, consider LT
- G-CSF + erythropoietin combination shown to reduce mortality in some studies
- Prognosis poor with multiple organ failures
11. Fibrosis Reversal
Regression of cirrhosis is now well established:
- Hepatitis C cure with DAAs → demonstrated fibrosis regression/reversal
- HBV suppression → fibrosis regression
- Abstinence from alcohol → regression in some patients
- Mechanisms: macrophage-mediated matrix degradation, stellate cell deactivation/apoptosis, scar remodeling
- Fibrous septa become thinner, denser, then fragment; nodules coalesce
12. Summary Table
| Feature | Compensated | Decompensated |
|---|---|---|
| Symptoms | Absent or nonspecific | Ascites, jaundice, encephalopathy, GI bleed |
| Liver function | Mostly preserved | Impaired |
| Portal pressure | Mildly elevated | Markedly elevated |
| MELD | Usually <15 | Usually >15 |
| Median survival | 9–12 years | ~2 years |
| 5-year mortality | ~5× general population | ~10× general population |
Sources:
- Robbins & Kumar Basic Pathology, p. 598
- Sleisenger and Fordtran's GI and Liver Disease, Ch. 74
- Goldman-Cecil Medicine, Ch. 139
- Harrison's Principles of Internal Medicine 22e, Ch. 355 & 347
- Yamada's Textbook of Gastroenterology, 7th ed.
This is a shared conversation. Sign in to Orris to start your own chat.