Thoracotomy 20 marks university exam surgery subject
THORACOTOMY
Definition
Indications
- Lung resections (pneumonectomy, lobectomy, segmentectomy) - most frequent indication
- Oesophageal surgery (oesophagectomy, hiatus hernia repair)
- Mediastinal tumour resection (thymoma, lymphoma)
- Thoracic aortic aneurysm repair
- Cardiac procedures (valvular surgery, pericardectomy)
- Sympathectomy
- Correction of chest wall deformities
- Massive haemothorax unresponsive to chest drain
- Cardiac tamponade (penetrating trauma)
- Aortic cross-clamping in haemorrhagic shock
- Traumatic cardiac arrest with penetrating injury (resuscitative thoracotomy)
- Air embolism
- Bronchial disruption
Types of Thoracotomy Incisions
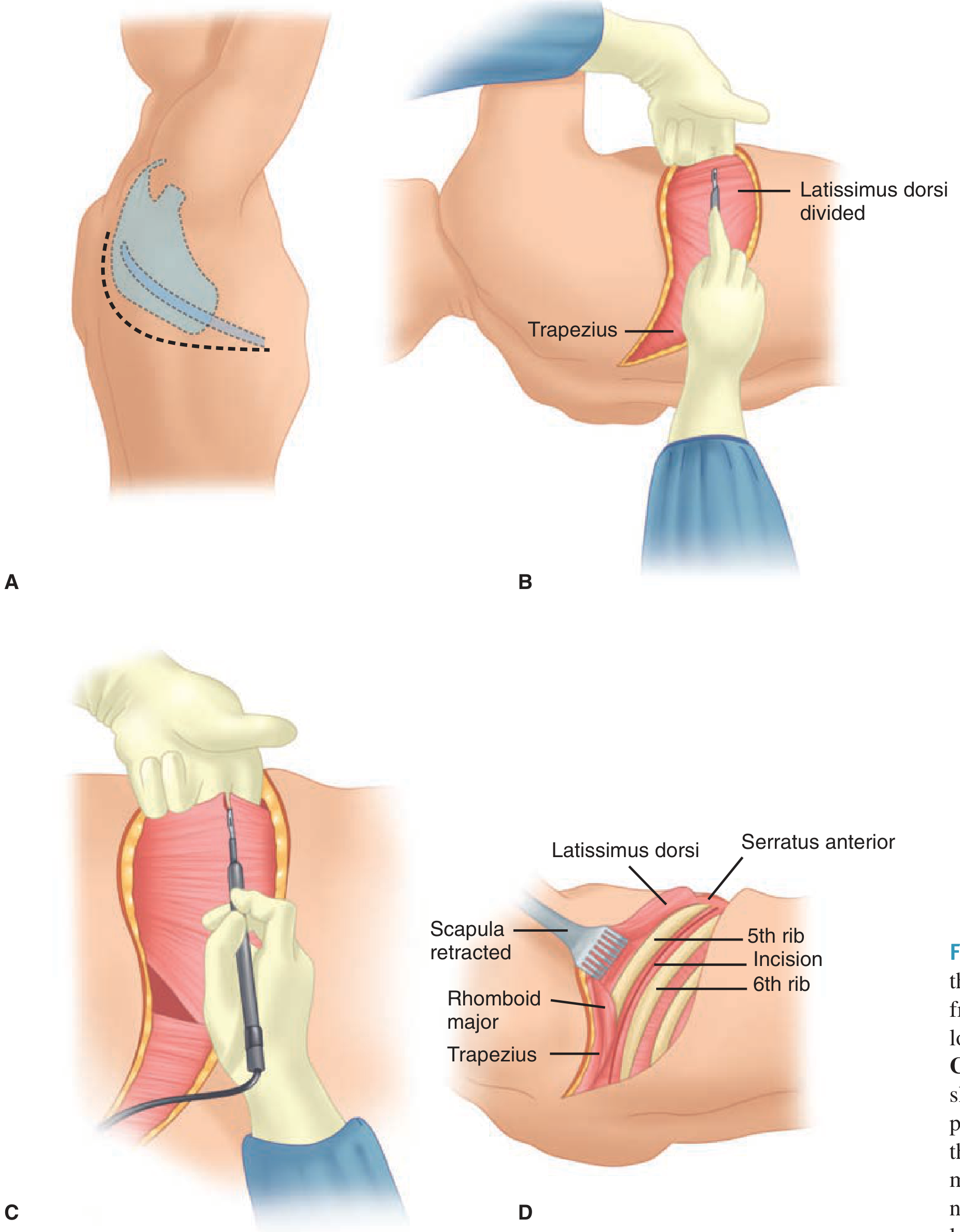
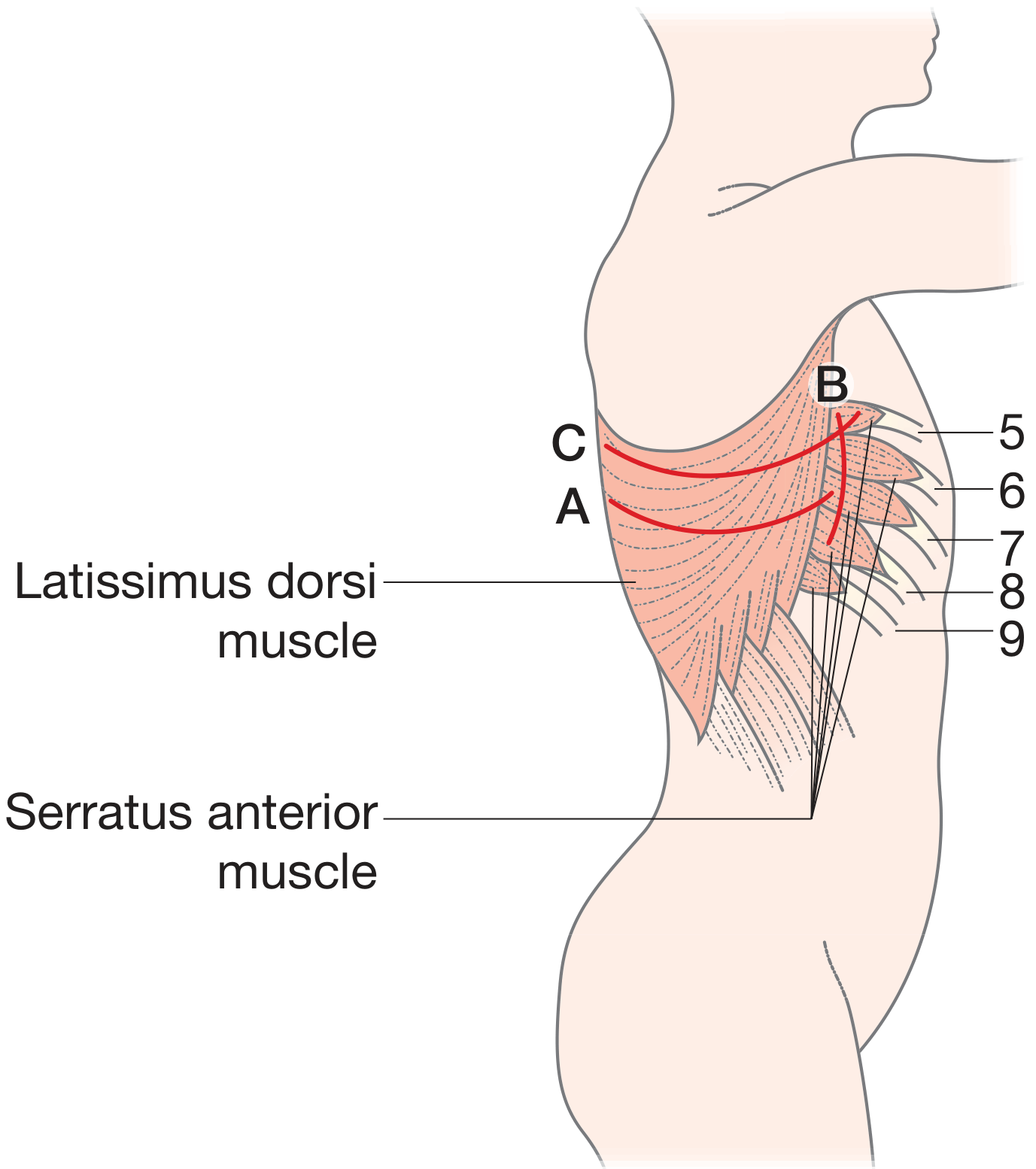
1. Posterolateral Thoracotomy (Standard / Most Common)
- Skin incision passes 1-2 cm below the tip of the scapula, extending posteriorly and superiorly between the medial border of the scapula and the spine - forming a curved line connecting three points: (i) 4th/5th intercostal space at midclavicular line, (ii) one fingerbreadth below scapula tip, (iii) midpoint between spine and scapula medial border.
- Incision deepened through subcutaneous tissue to the latissimus dorsi - divided with diathermy (careful haemostasis).
- A plane is developed deep to the scapula and serratus anterior.
- Ribs counted from the 2nd rib (highest palpable); 6th rib periosteum is scored at its upper border.
- Periosteal elevator lifts periosteum, or intercostal muscle is cut with diathermy just above the rib, to avoid the neurovascular bundle running below each rib.
- Pleura entered by blunt dissection; rib spreader inserted gently to avoid rib fracture.
- Chest entered through the 5th or 6th interspace for most pulmonary work.
2. Anterolateral Thoracotomy
- Patient supine - anaesthesiologist has full access for resuscitation
- Incision in 4th or 5th interspace from sternum to anterior axillary line
- Used traditionally in trauma victims and haemodynamically unstable patients
- Quicker entry; avoids repositioning
- Can be extended to bilateral (clamshell) thoracotomy
3. Median Sternotomy
- Midline sternal split
- Access: Anterior mediastinum, ascending aorta and arch, pulmonary arteries, carina, anterior heart, both pleural spaces
- Standard approach for cardiac surgery
4. Clamshell (Bilateral Anterior) Thoracotomy
- Left + right anterolateral thoracotomies joined by transverse sternotomy
- Excellent bimanual access to both pleural cavities and heart
- Used in: bilateral lung transplantation, major mediastinal injury, surgeons unfamiliar with routine chest entry
- Not the approach of choice for posterolateral structures
5. Trap-Door (Hemiclamshell) Thoracotomy
- Anterolateral thoracotomy + partial median sternotomy
- For access to mediastinal structures and subclavian vessels on one side
Approach Selection by Structure (Emergency Context)
| Structure | Best Approach |
|---|---|
| Left lung, thoracic aorta, left subclavian origin, left heart, lower oesophagus | Left anterolateral thoracotomy |
| Right lung, azygos vein, SVC, upper oesophagus, thoracic trachea | Right anterolateral thoracotomy |
| Anterior heart, ascending aorta and arch, pulmonary arteries, carina | Median sternotomy |
Resuscitative / Emergency Department Thoracotomy (EDT)
- Trauma victims with severe refractory haemodynamic instability or cardiac arrest
- Penetrating trauma with witnessed cardiac arrest
- Non-traumatic hypothermic cardiac arrest
- Blunt trauma cardiac arrest without signs of life
- Obvious non-survivable injuries
- Asystole without signs of life
- Signs of prolonged arrest (lividity, rigor mortis)
- Open cardiac massage
- Release of cardiac tamponade
- Aortic cross-clamping to redistribute perfusion to heart and brain
- Control of haemorrhage
- Treatment of air embolism
Anaesthetic Considerations
- Double-lumen endotracheal tube - allows separate ventilation; operated lung deflated to facilitate surgery and protect the contralateral lung
- Arterial line for intraoperative hemodynamic and oxygenation monitoring
- Central venous access in patients with significant underlying morbidity
- Lateral decubitus position with all pressure points padded
Wound Closure
- Ribs are approximated with strong absorbable pericostal sutures (around the ribs)
- Muscles closed in layers
- One or two chest drains (intercostal tubes) placed before final closure - one apical drain for air, one basal drain for fluid/blood
- Subcutaneous and skin closure in layers
Postoperative Analgesia
- Epidural catheter (placed pre-operatively or intraoperatively) - preferred
- Paravertebral catheter (surgically sited intraoperatively)
- Intercostal nerve block with long-acting local anaesthetic
- Multimodal systemic analgesia (NSAIDs, opioids)
Complications
Intraoperative
- Haemorrhage (intercostal vessel injury, pulmonary vessel injury)
- Lung injury / air leak
- Nerve injury (phrenic nerve, recurrent laryngeal nerve, thoracic sympathetic chain)
- Coronary artery injury (in EDT)
- Oesophageal injury
- Arrhythmias
Postoperative - Early
- Haemothorax / haemorrhage - most common early complication
- Pneumothorax / tension pneumothorax (chest drain blocked or displaced)
- Respiratory failure - inadequate pain control, pre-existing lung disease
- Atelectasis and pneumonia (due to pain-related splinting)
- Air leak (prolonged alveolar air leak)
- Wound infection / empyema
- Cardiac arrhythmias
- DVT / pulmonary embolism
Postoperative - Late
- Post-thoracotomy pain syndrome - chronic pain (>2 months) due to intercostal nerve damage from rib retraction; occurs in up to 50% of patients
- Frozen shoulder / restricted shoulder movement
- Hypesthetic nipple (with hemiclamshell / anterior approach)
- Bronchopleural fistula
- Empyema
- Scoliosis (in children)
Minimally Invasive Alternative: VATS
- Avoids rib-spreading
- Reduces post-operative pain significantly
- Shortens hospital stay
- Allows faster recovery, especially in frail patients
- Achieves equivalent oncological outcomes for appropriate cases
Summary Points for Exam
| Feature | Posterolateral | Anterolateral | Clamshell | Median Sternotomy |
|---|---|---|---|---|
| Position | Lateral decubitus | Supine | Supine | Supine |
| Interspace | 5th / 6th | 4th / 5th | Bilateral 4th | Midline sternum |
| Muscles divided | Latissimus dorsi, serratus anterior | Pectoralis | Bilateral pectorals | Nil (bone split) |
| Main use | Lung resection, oesophagus | Trauma, emergency | Bilateral lung Tx, heart | Cardiac, mediastinum |
| Drawback | Cannot use in emergency easily | Limited posterior access | Morbid, unstable chest wall | Limited posterior access |
Jand drawn diagrams of sternotomies
Clean medical surgical diagram showing types of sternotomy incisions on a human chest (anterior view). Label each type clearly: 1) Full Median Sternotomy - complete vertical midline split from jugular notch to xiphoid process, 2) Upper Partial Sternotomy (Inverted T or J) - upper half split only, 3) Lower Partial Sternotomy - lower half split only, 4) Mini-Sternotomy - small upper midline split to 3rd rib level. Show the sternum, clavicles, ribs, jugular notch, manubrium, sternal body, xiphoid process. Use dashed red lines for incision paths. White background, clean anatomical illustration style, clearly labeled.
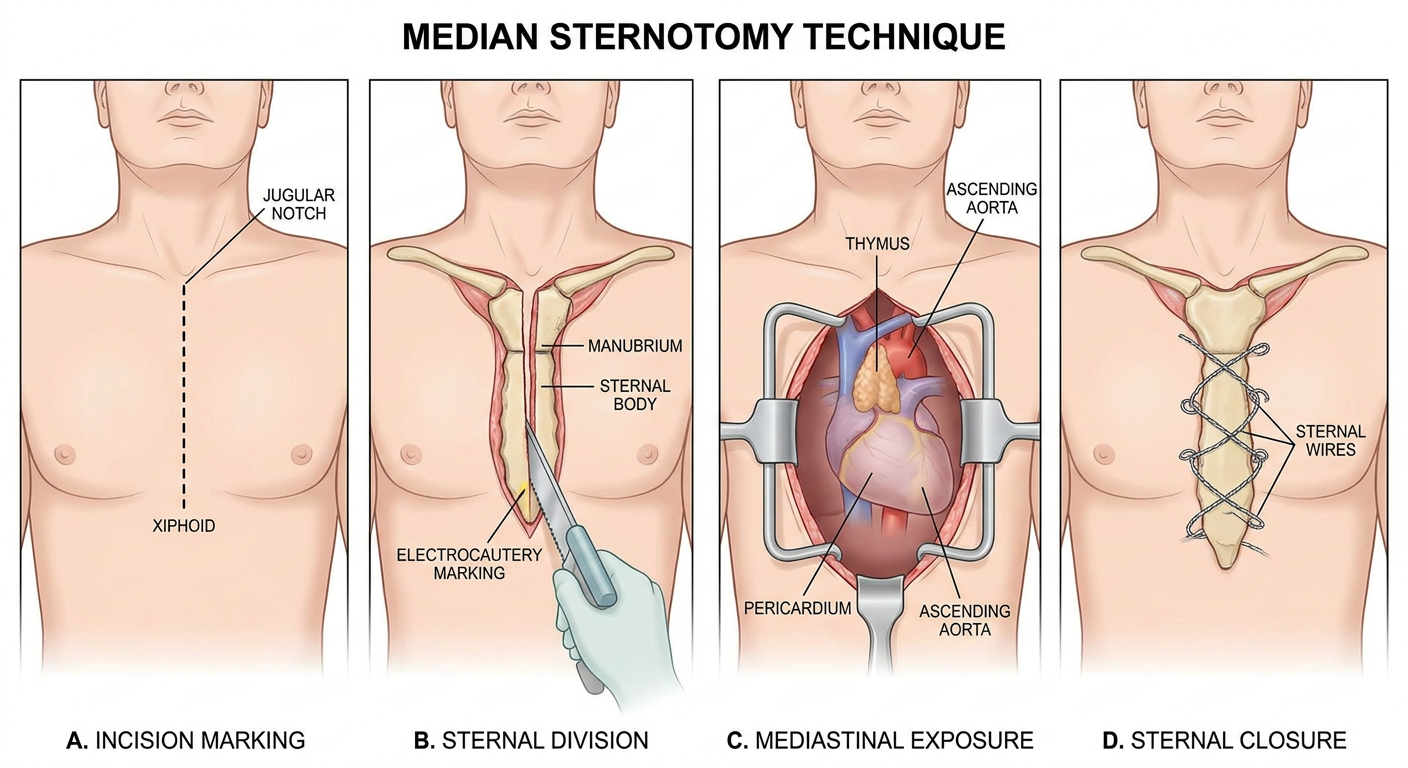
Medical surgical diagram showing step-by-step technique of median sternotomy. Panel A: patient supine position, skin incision line from jugular notch to xiphoid marked with dashed line. Panel B: sternum exposed, midline electrocautery marking, sternal saw dividing sternum. Panel C: sternal retractor inserted and opened, showing the mediastinum, pericardium, aortic arch, and thymus visible. Panel D: closure with sternal wires (figure-of-8 or simple interrupted stainless steel wires around sternum). Labeled anatomical structures: jugular notch, manubrium, sternal body, xiphoid, pericardium, thymus, ascending aorta. Clean medical illustration style, white background.
STERNOTOMY - Complete Notes with Diagrams
Definition
Types of Sternotomy
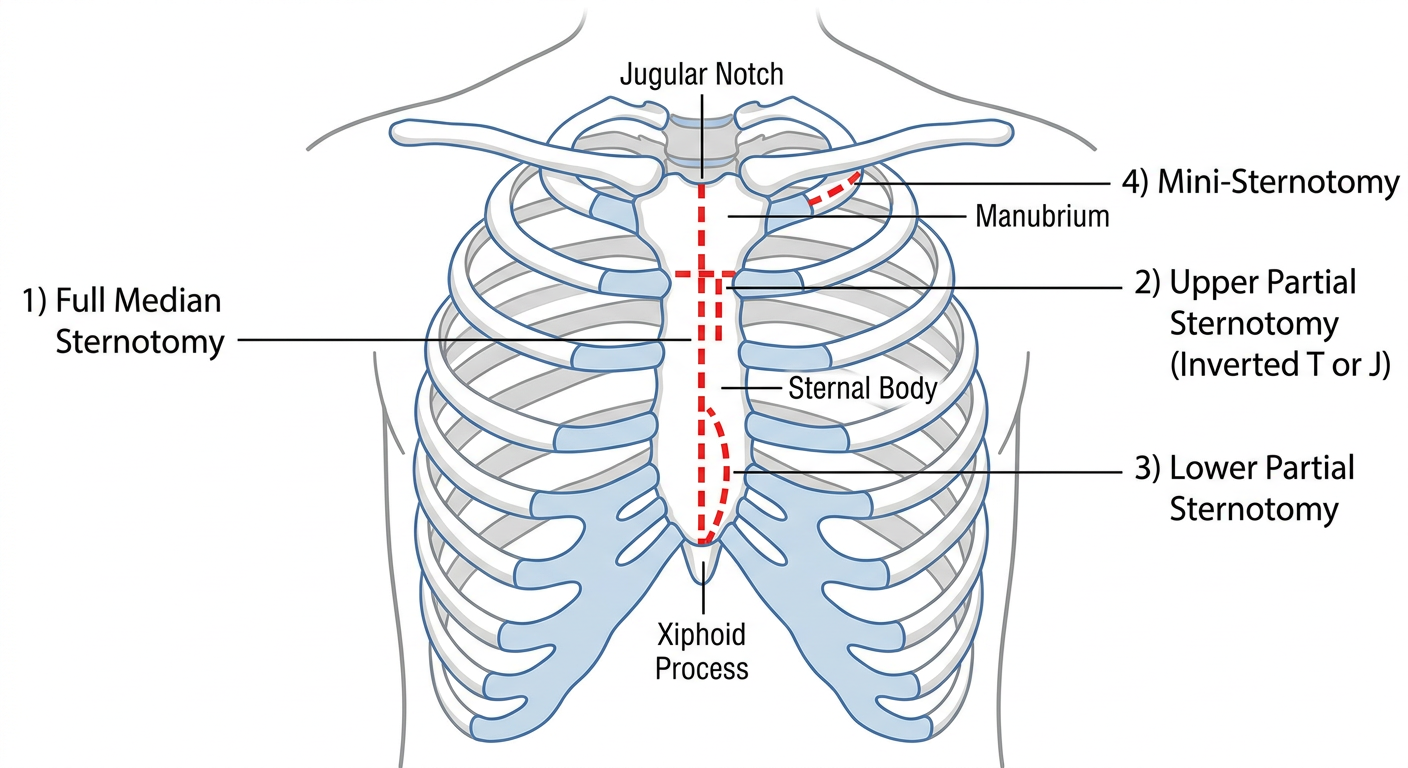
1. Full Median Sternotomy (Standard)
- Skin incision from sternal notch to xiphisternal junction with a scalpel
- Subcutaneous tissue and suprasternal attachments divided with electrocautery
- Blunt finger dissection creates a retrosternal plane (between sternum and venous structures beneath)
- Electrocautery marks a target line in the centre of the sternum (confirmed by palpating anterior rib insertions)
- Xiphoid attachments taken down and bluntly dissected
- Anaesthesia deflates the lungs momentarily
- Sternum divided in midline with sternal saw (oscillating saw or Gigli saw)
- Bone-edge bleeding controlled with electrocautery + bone wax
- Sternal retractor inserted and opened slowly (avoid fracture)
- Thymus and upper mediastinal fat divided to expose aortic arch; pericardium opened and retracted
- Pericardium loosely approximated (or left open)
- Mediastinal + pericardial drains placed
- Sternum closed with stainless steel wires (figure-of-8 or simple interrupted, typically 6-8 wires)
- Layers: pectoral fascia - subcutaneous tissue - skin
2. Upper Partial Sternotomy (Mini-Sternotomy)
- Inverted-T or J sternotomy (split continues transversely into the 3rd interspace on one side)
- Straight upper partial split
3. Lower Partial Sternotomy
4. Clamshell Sternotomy (Transverse / Bilateral Thoracosternotomy)
- Bilateral lung transplantation (standard approach at many centres)
- Major mediastinal trauma
- Bilateral pulmonary resections
- Emergency access for surgeons unfamiliar with routine chest entry
5. Trap-Door (Hemiclamshell) Sternotomy
Summary Table
| Type | Extent of Sternal Division | Main Use |
|---|---|---|
| Full Median Sternotomy | Jugular notch → xiphoid, midline full split | Cardiac surgery, mediastinal masses, great vessel repair |
| Upper Partial (Mini-sternotomy) | Jugular notch → 3rd rib, upper split only | Aortic valve, thymoma, superior mediastinum |
| Lower Partial | Xiphoid → body, lower split only | Lower mediastinum access |
| Clamshell | Bilateral 4th space + transverse sternal cut | Bilateral lung Tx, major mediastinal trauma |
| Trap-door / Hemiclamshell | Anterolateral thoracotomy + partial sternotomy ± collar | Tracheal tumours, subclavian vessel injury |
Anaesthetic Considerations
- Supine position, arms tucked
- Standard endotracheal tube (single lumen - no lung isolation required for most cardiac cases)
- Cardiopulmonary bypass (CPB) with cannulation of ascending aorta + right atrium / venae cavae
- Lungs deflated momentarily during sternal saw division to protect the pleura
- Arterial line, central venous access, transoesophageal echocardiography (TEE) standard
Complications
Early
- Haemorrhage - from sternal edges, internal mammary artery branches, or mediastinal vessels
- Pneumothorax / haemopneumothorax (if pleural space inadvertently entered)
- Cardiac injury during saw division (rare; risk higher in re-do sternotomy)
- Arrhythmias
- Air embolism
Late / Specific to Sternotomy
| Complication | Detail |
|---|---|
| Deep Sternal Wound Infection / Mediastinitis | Occurs in 0.5-2% of patients; sternal dehiscence results; mortality up to 40%; requires debridement and rewiring. Risk factors: diabetes, obesity, smoking, dialysis, high transfusion requirements |
| Sternal Non-union / Dehiscence | Wires cut through osteoporotic bone; sternal instability ("clicking sternum") |
| Chronic sternal pain | Wire-related pain or costochondral disruption |
| Keloid / hypertrophic scar | Long midline scar |
| Post-pericardiotomy syndrome | Fever, pleuritis, pericarditis weeks post-surgery |
| Neurological deficit | Stroke from air/particulate emboli during CPB |
Key Anatomical Relations During Median Sternotomy
| Structure | Relation |
|---|---|
| Left brachiocephalic vein | Crosses the top of the mediastinum - mobilised and looped, rarely divided |
| Thymus / mediastinal fat | Divided to expose aortic arch and great vessel origins |
| Phrenic nerves | Run laterally on the pericardium - must be avoided |
| Right vagus nerve | Lateral to right carotid, passes anterior to right subclavian origin |
| Recurrent laryngeal nerve (right) | Wraps around right subclavian origin - vulnerable during brachiocephalic vessel exposure |
| Internal mammary (thoracic) arteries | Run 1 cm lateral to sternal edge - preserved during saw division; used as CABG conduits |
Draw hand drawn diagrams for these
Hand drawn pencil sketch style medical diagram of a human chest (anterior view) showing full median sternotomy. Sketch shows: clavicles, ribs, sternum with manubrium, sternal body and xiphoid process labeled with handwritten text. A bold dashed vertical line runs from jugular notch all the way down to xiphoid process showing the incision. Small arrows point to: jugular notch, manubrium, sternal body, xiphoid process. Title written at top in handwriting: "FULL MEDIAN STERNOTOMY". Rough pencil sketch look, slightly uneven lines, like a medical student's notebook drawing.
Hand drawn pencil sketch style medical diagram of a human chest (anterior view) showing upper partial sternotomy (mini sternotomy). Sketch shows sternum, ribs, clavicles. A bold dashed vertical line runs from jugular notch down only to the 3rd rib level (upper half only), then stops. Handwritten label: "Upper Partial / Mini-Sternotomy". Small arrows label: jugular notch, 3rd rib, manubrium, stopped here. A second variant shows a J-shaped incision curving into the 3rd intercostal space on the right. Title: "UPPER PARTIAL STERNOTOMY (Mini / J-Sternotomy)". Rough pencil sketch notebook style.
Hand drawn pencil sketch style medical diagram of a human chest (anterior view) showing clamshell sternotomy incision. The sketch shows: both left and right anterolateral thoracotomy incisions curved across the 4th intercostal space, connected in the middle by a horizontal transverse sternotomy cut across the sternum. The whole incision looks like an open clamshell or butterfly shape. Handwritten labels: "Left anterolateral thoracotomy", "Right anterolateral thoracotomy", "Transverse sternotomy", "4th intercostal space". Arrows point to each component. Title at top: "CLAMSHELL STERNOTOMY". Rough pencil sketch notebook style like a medical student drew it.
Hand drawn pencil sketch style medical diagram of a human chest (anterior view) showing trap-door / hemiclamshell sternotomy incision. Shows: left anterolateral thoracotomy incision in 4th intercostal space on the left side, extending medially and joining a partial upper median sternotomy (upper sternal split). Optional dashed extension showing collar neck incision above. The incision outline looks like an open trap-door or hinge on one side. Handwritten labels: "Left anterolateral thoracotomy", "Partial median sternotomy", "Collar incision (optional)", "Trap-door opening". Title: "TRAP-DOOR (HEMICLAMSHELL) STERNOTOMY". Rough pencil sketch notebook drawing style.
400, message: Got more than 4194304 bytes when reading: b'data: {"candidates": [{"content": {"role": "model","parts": [{"inlineData": {"mimeType": "image/png"...'.
We encountered an error while processing your request. Please try again or reach out to us for help.