Teach me like neonatologist/paeditrcian in depth topic - feral Circulation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the complete, in-depth teaching session.
Fetal Circulation - A Neonatologist's / Paediatrician's Deep Dive
(Sources: The Developing Human - Moore, Langman's Medical Embryology, Guyton & Hall Medical Physiology, Ganong's Review, Harriet Lane Handbook 23e)
1. The Core Concept: Why Fetal Circulation is Different
The fetus cannot use its own lungs for gas exchange - they are filled with fluid and the placenta does all the work of a "fetal lung." Therefore the cardiovascular system is specifically engineered to:
- Deliver the most oxygenated blood to the brain and myocardium (the organs that matter most)
- Bypass the non-functional lungs (high pulmonary vascular resistance diverts flow)
- Bypass most of the liver (it receives a large volume of blood from the placenta that does not need hepatic processing)
- Return deoxygenated blood back to the placenta for reoxygenation
This is achieved through three obligate fetal shunts and a unique parallel-circuit arrangement (rather than the series circuit of adult life).
2. The Fetal Circulation: Step-by-Step Blood Flow
Here is the full fetal circulation diagram:
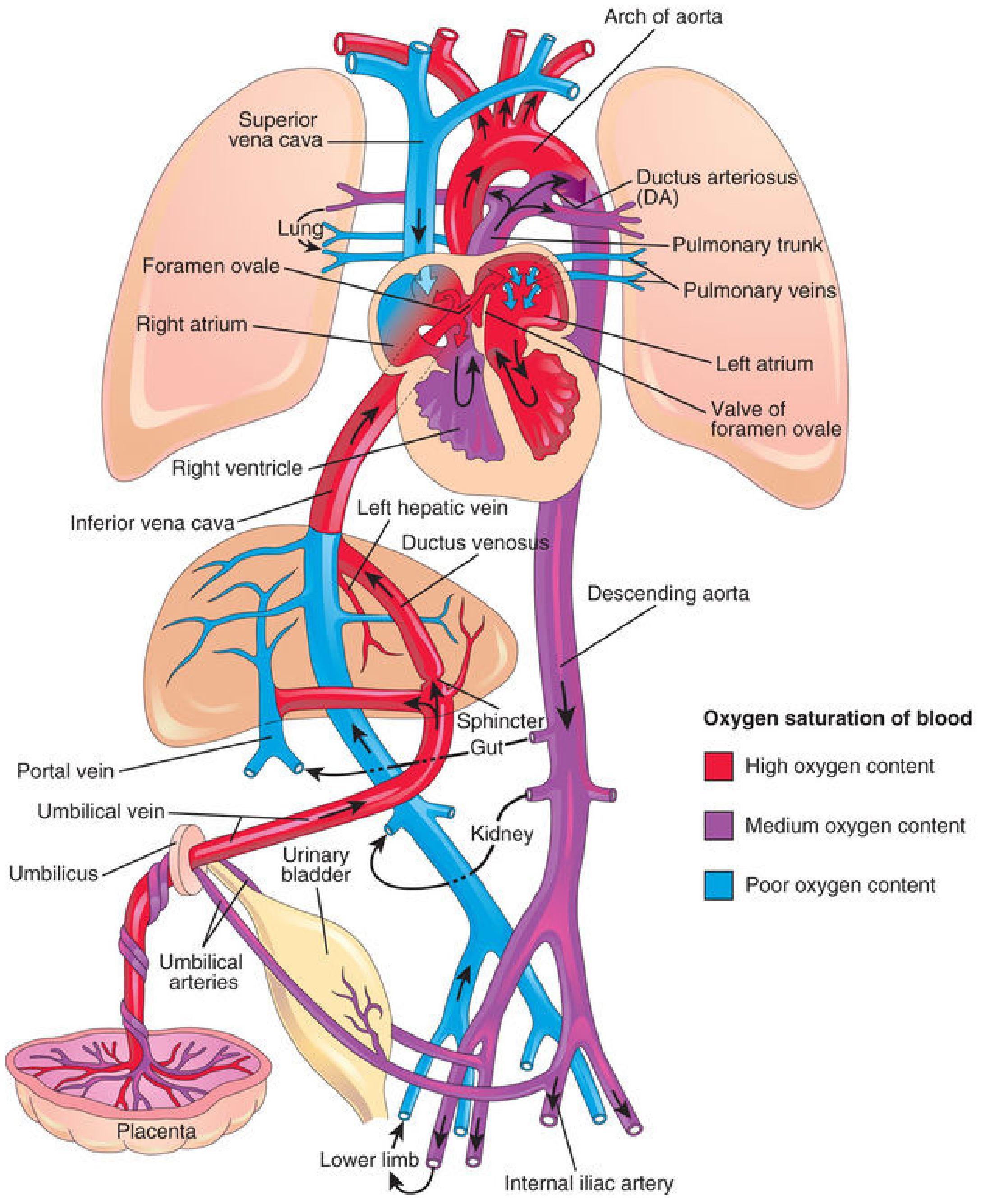
Fig. 13.46 from The Developing Human (Moore) - Color-coded oxygen saturations and the three shunts
Step 1: Blood leaving the placenta (Umbilical Vein)
- Blood in the umbilical vein is ~80% saturated with O2 - this is the most oxygenated blood in the entire fetal circuit
- It enters the fetus at the umbilicus and travels toward the liver
- Key point for exam/ward: The umbilical vein carries oxygenated blood - the opposite of adult veins. This trips up many students and trainees.
Step 2: The Ductus Venosus (Shunt #1)
- At the porta hepatis, the umbilical venous blood splits:
- ~50% goes directly through the ductus venosus into the inferior vena cava (IVC), bypassing the liver entirely
- The remaining ~50% flows through the portal sinusoids and hepatic veins into the IVC
- Physiologic sphincter: There is a functional sphincter near the origin of the ductus venosus that prevents cardiac overload during high-flow states (e.g., uterine contractions). Its existence as a true anatomic sphincter is debated, but the physiologic function is well established.
- The blood entering the IVC from the DV mixes with poorly oxygenated blood from the lower limbs, abdomen, and pelvis - so by the time it reaches the right atrium, saturation has dropped somewhat
Step 3: The Foramen Ovale (Shunt #2) - The "Selective Streaming" Phenomenon
This is where fetal circulation is truly ingenious:
- IVC blood enters the right atrium
- The crista dividens (the inferior free edge of the septum secundum) acts as a flow divider:
- Most of the IVC blood (the better-oxygenated portion from the DV) is preferentially directed across the foramen ovale into the left atrium
- A smaller amount of IVC blood mixes with the desaturated SVC blood in the right atrium and passes down through the tricuspid valve into the right ventricle
- The foramen ovale has a one-way valve (the septum primum acts as a flap valve), allowing only left-to-right flow in fetal life
- From the left atrium, blood enters the left ventricle and is pumped into the ascending aorta
- Critical neonatal point: The first branches of the ascending aorta are the coronary arteries and carotid arteries - so the heart muscle and brain receive the most oxygenated blood in the fetus. This is selective oxygen delivery by design.
Step 4: Blood from the SVC through the Right Ventricle
- Desaturated blood from the head and upper limbs returns via SVC
- This mixes in the right atrium with the remaining IVC blood
- Flows through tricuspid valve → right ventricle → pulmonary trunk
- In fetal life, pulmonary vascular resistance (PVR) is very high due to:
- Hypoxic pulmonary vasoconstriction (PO2 in fetal lung ~17-19 mmHg)
- Fluid-filled, unexpanded alveoli compressing vessels
- Structurally thick-walled pulmonary arterioles
- Result: Only ~12% of combined cardiac output passes through the lungs (vs. virtually 100% after birth)
Step 5: The Ductus Arteriosus (Shunt #3)
- Most of the blood from the pulmonary trunk bypasses the lungs via the ductus arteriosus (DA) and enters the descending aorta
- The DA connects the pulmonary trunk (just after the left pulmonary artery origin) to the descending aorta (just distal to the left subclavian artery)
- Mixing points in the descending aorta: blood from the aortic arch (previously supplied to head/arms) + ductus arteriosus blood. This mix is delivered to:
- Abdominal organs (gut, kidneys)
- Lower limbs
- And crucially: via the two umbilical arteries back to the placenta
- O2 saturation in the umbilical arteries is approximately 55-58% - this is the "venous" blood heading back to be reoxygenated
O2 Saturation at Key Points (Five Mixing Zones)
| Location | Event | Saturation Change |
|---|---|---|
| I. Liver | UV mixes with portal blood | Slight drop |
| II. IVC | Mixes with deoxygenated lower body blood | Drop |
| III. Right atrium | Mixes with SVC blood | Drop |
| IV. Left atrium | Mixes with small amount of pulmonary venous return | Slight drop |
| V. Descending aorta | DA blood mixes with aortic arch blood | Drop |
(Langman's Medical Embryology, p.237)
3. Quantitative Distribution of Fetal Cardiac Output
(Guyton & Hall, p.1052)
- ~55% of combined cardiac output flows through the placenta
- ~45% perfuses all fetal tissues
- Only ~12% goes through the lungs in fetal life
- After birth, virtually 100% goes through the lungs
This means the right ventricle dominates in fetal life - it pumps a larger volume than the left ventricle. This is why the neonatal ECG normally shows right ventricular dominance (right axis deviation, dominant R in V1) and why this pattern in an older child would be pathological.
4. Parallel vs. Series Circulation
| Feature | Fetal | Adult (Postnatal) |
|---|---|---|
| Circuit arrangement | Parallel (both ventricles pump to systemic circuit via shunts) | Series (RV → lungs → LV → body) |
| Dominant ventricle | Right ventricle | Left ventricle |
| Pulmonary blood flow | ~12% of CO | ~100% of CO |
| PVR | High | Low |
| SVR | Low | High |
| Gas exchange organ | Placenta | Lungs |
5. Transitional Circulation at Birth - The Most Critical Period
This is when things can go catastrophically wrong. The transition involves massive, rapid, and sequential hemodynamic changes within seconds to minutes.
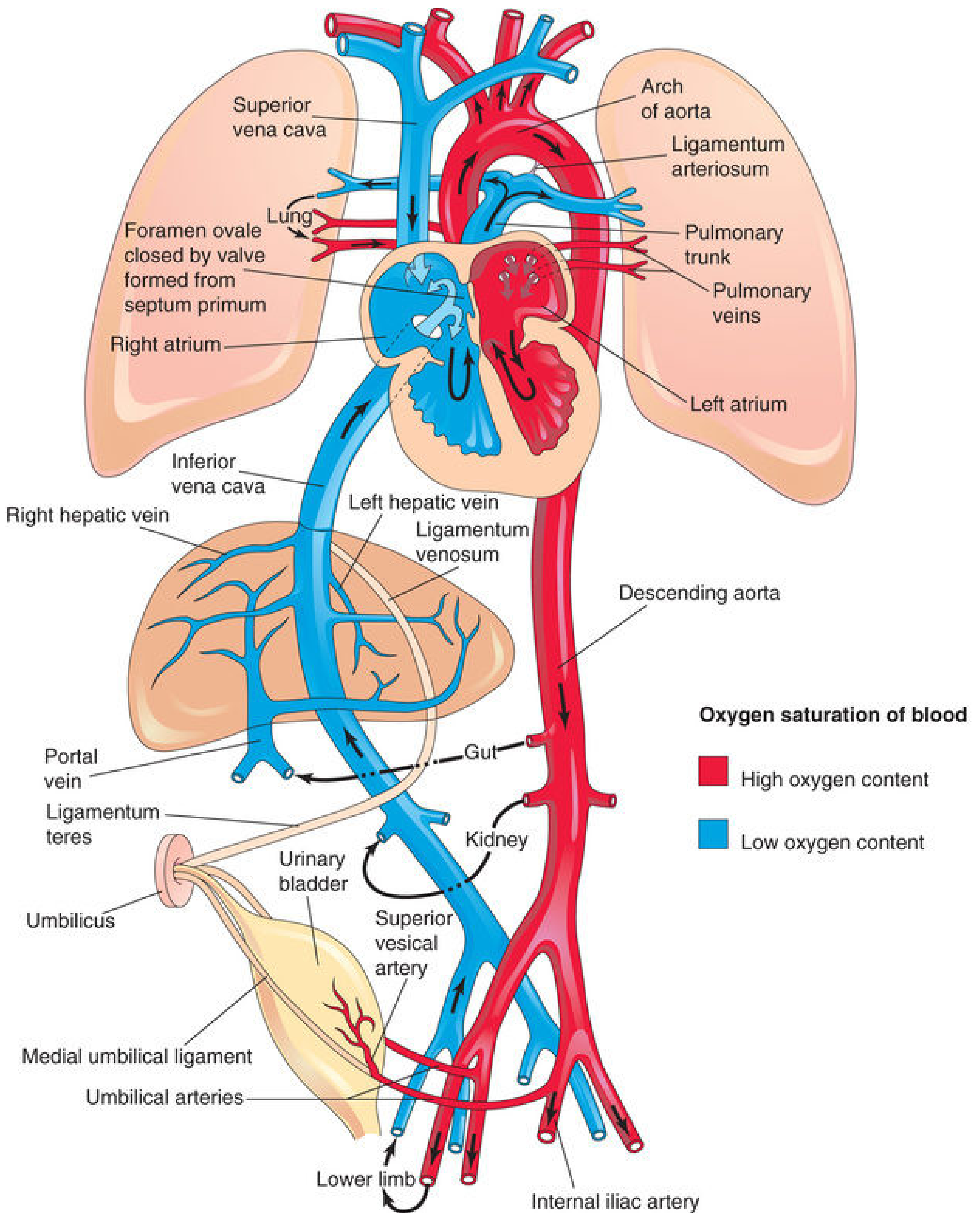
Neonatal circulation - adult derivatives of fetal vessels
Trigger Events at Birth
Two simultaneous events initiate the transition:
- Umbilical cord clamping → loss of low-resistance placental circuit → SVR doubles
- First breath/lung expansion → lungs expand, hypoxic vasoconstriction reverses → PVR drops ~5-fold
Sequential Closure of the Three Shunts
Closure of Umbilical Arteries
- Occur within minutes of birth
- Mechanism: thermal and mechanical stimuli + rise in O2 tension → smooth muscle contraction
- Functional closure: minutes; anatomical obliteration: 2-3 months
- Adult derivatives: Medial umbilical ligaments (distal parts); proximal parts remain open as the superior vesical arteries
Closure of Umbilical Vein and Ductus Venosus
- Follows shortly after umbilical artery closure
- (Blood from placenta can still enter newborn briefly after birth if cord is unclamped)
- Adult derivatives:
- Umbilical vein → Ligamentum teres hepatis (in lower margin of falciform ligament)
- Ductus venosus → Ligamentum venosum
Closure of the Foramen Ovale
- After birth: SVR rises → LA pressure rises; PVR falls → RA pressure falls
- Net result: LA pressure now exceeds RA pressure → the flap valve (septum primum) is pressed against septum secundum and closes
- Functional closure: immediate after first breath (septum primum apposed to septum secundum)
- Important: In the first days of life, this closure is reversible - crying creates increased right-sided pressure, reopening the shunt temporarily → transient cyanosis during crying in neonate is normal!
- Anatomical closure: fusion of septa takes ~1 year
- ~20% of adults never achieve complete anatomical closure = patent foramen ovale (PFO) - usually clinically silent unless there is elevated RA pressure
- (Langman's, p.238)
Closure of the Ductus Arteriosus
- Most clinically relevant shunt from a neonatal perspective
- Mechanism has two components:
- Increased PO2: After birth, PO2 in DA rises from 15-20 mmHg (fetal) to ~100 mmHg. Oxygen directly causes smooth muscle constriction in the DA wall.
- Loss of PGE2: In fetal life, PGE2 (produced by placenta) keeps the DA dilated. With placental separation, PGE2 levels fall rapidly.
- Bradykinin: Released from lungs during initial inflation also mediates constriction
- Functional closure: within hours to 1-8 days
- Anatomical/permanent closure: 1-4 months → becomes the Ligamentum arteriosum
- (Guyton & Hall, p.1052; Langman's, p.238)
Summary Table - Fetal Vessel Adult Derivatives
| Fetal Vessel | Adult Derivative |
|---|---|
| Umbilical vein | Ligamentum teres hepatis |
| Ductus venosus | Ligamentum venosum |
| Foramen ovale | Fossa ovalis (closed) |
| Ductus arteriosus | Ligamentum arteriosum |
| Umbilical arteries (distal) | Medial umbilical ligaments |
| Umbilical arteries (proximal) | Superior vesical arteries |
6. The Fetal Lung - Why It Has Such High PVR
Understanding fetal pulmonary vasoconstriction is essential for PPHN and respiratory management:
- Fetal pulmonary arterioles have thick, hypertrophied smooth muscle layers
- PO2 in fetal lung tissue is ~17-19 mmHg (hypoxia) - which causes tonic hypoxic pulmonary vasoconstriction (HPV)
- PVR in fetus is 8-10x higher than after birth
- After the first breath: oxygen tension rises → HPV reverses → PVR falls rapidly
- Additionally, physical expansion of alveoli de-compresses the perivascular space, physically reducing resistance
7. Persistent Pulmonary Hypertension of the Newborn (PPHN) - The Failed Transition
(Harriet Lane Handbook 23e, p.651-652)
PPHN is what happens when the normal fall in PVR does not occur, causing persistent right-to-left shunting through fetal channels.
Pathophysiology
- PVR remains elevated after birth
- Right-sided pressures exceed left-sided pressures
- The foramen ovale and/or ductus arteriosus remain open with right-to-left shunting
- Deoxygenated blood bypasses the lungs → profound hypoxemia
- A vicious cycle: hypoxemia → more vasoconstriction → worse shunting
Etiology / Risk Factors
- Most commonly: term or post-term infants
- Caesarean section (no "labor squeeze" to clear lung fluid)
- Fetal distress, low Apgar scores, asphyxia
- Meconium aspiration syndrome (MAS)
- Congenital pneumonia / sepsis
- Congenital diaphragmatic hernia (CDH) - hypoplastic lungs with abnormal vasculature
- Renal agenesis / oligohydramnios - pulmonary hypoplasia
- Polycythemia / hyperviscosity
Diagnosis
- Onset: within 12-24 hours of birth
- Hallmark: Severe hypoxemia disproportionate to radiologic changes
- PaO2 <35-45 mmHg in 100% O2
- Pre-ductal vs post-ductal SpO2 gradient:
- Pre-ductal = right hand (above the DA)
- Post-ductal = either foot (below the DA)
- A difference of ≥7-15 mmHg PaO2 (or ≥3-5% SpO2) is significant - indicates right-to-left shunting at the DA
- Must distinguish from cyanotic congenital heart disease - hyperoxia test + echocardiogram
Management
- Optimize oxygenation - supplemental O2, optimize hemoglobin
- Minimize pulmonary vasoconstriction:
- Minimal handling, reduce noxious stimuli, sedation ± paralysis
- Avoid severe hypocarbia (PCO2 <30 mmHg) - causes cerebral and myocardial ischemia
- Consider high-frequency ventilation
- Maintain systemic BP to reverse the R→L shunt gradient: volume + inotropes
- Pulmonary vasodilators:
- Inhaled Nitric Oxide (iNO): First-line; 20 ppm starting dose (10 ppm in preterms); reduces PVR selectively; monitor methemoglobin (reduce dose if >4%), NO2 toxicity
- Prostacyclin analogs (e.g., epoprostenol): Pulmonary vasodilator
- Sildenafil: PDE5 inhibitor → ↑cGMP → pulmonary vasodilation; especially useful when iNO unavailable
- ECMO (Extracorporeal Membrane Oxygenation):
- Last resort for refractory cases
- Oxygenation Index (OI) >40 for >3 hours, or A-aO2 gradient ≥610 for 8 hours
- Eligibility: birth weight >2000g, gestation >34 weeks
- Must exclude reversible intracranial hemorrhage before initiation (head ultrasound)
8. Key Clinical Pearls for the Neonatologist / Paediatrician
Umbilical Vein Catheter (UVC)
- Route: UV → ductus venosus → IVC → right atrium
- Tip should ideally sit at the junction of IVC and RA (T8-T9 on XR)
- If tip is too far in: can enter RA → arrhythmias, pericardial effusion
- The ductus venosus is the pathway for rapid IV access in newborn resuscitation
Patent Ductus Arteriosus (PDA)
- DA stays open in prematurity because:
- Lower PO2 (less oxygen-mediated constriction)
- Higher circulating PGE2 (immature metabolism)
- Immature smooth muscle response to oxygen
- Clinical signs of significant PDA: bounding pulses, wide pulse pressure, hyperactive precordium, continuous "machinery" murmur at left upper sternal border
- Medical closure: Indomethacin or Ibuprofen (NSAIDs - inhibit prostaglandin synthesis → allow DA constriction)
- PGE1 (Alprostadil): Used deliberately to KEEP the DA open in duct-dependent congenital heart lesions (e.g., transposition, pulmonary atresia, hypoplastic left heart)
Fetal Heart Rate (FHR) and Oxygen Delivery
- Fetal HR is 110-160 bpm - the fetus compensates for lower O2 delivery by running a higher cardiac output
- Fetal Hb (HbF) has higher O2 affinity than adult HbF (shifts dissociation curve left) - another adaptation to extract O2 from the relatively low PO2 placental environment
- At birth, HbF begins to switch to HbA over 6 months
Why Crying Makes a Normal Newborn Transiently Blue
- Crying raises intrathoracic and right atrial pressure
- If foramen ovale is not yet anatomically fused (normal in first days-weeks), this can briefly reopen R→L shunting
- Transient acrocyanosis (blue hands and feet) in a newborn in the first 24-48 hours is normal and represents vasomotor instability, not cyanotic heart disease
Pre-ductal vs Post-ductal Saturation - How to Use It
| Clinical Scenario | Pre-ductal SpO2 | Post-ductal SpO2 | Interpretation |
|---|---|---|---|
| Normal transition | ≥95% | ≥95% | Normal |
| PDA with R→L shunt (PPHN/DA-level) | Higher | Lower | Right-to-left DA shunting |
| Transposition of Great Arteries | Lower | Higher | Reversed differential cyanosis |
| Normal healthy term neonate (first 10 min) | May be 85-90% | Slightly lower | Normal transition; use Dawson saturation targets |
9. Summary Diagram - Fetal vs Neonatal Circulation
| Parameter | Fetal Circulation | Neonatal (After Transition) |
|---|---|---|
| Gas exchange | Placenta | Lungs |
| Umbilical vein | Carries O2-rich blood | Becomes ligamentum teres |
| Ductus venosus | Bypasses liver | Becomes ligamentum venosum |
| Foramen ovale | Open, L→R in fetus | Closes (fossa ovalis) |
| Ductus arteriosus | Open, maintains with PGE2 | Closes (ligamentum arteriosum) |
| PVR | Very high | Low |
| SVR | Low | High |
| Dominant ventricle | Right | Left |
| ECG | Right axis, R dominant V1 | Gradually becomes left dominant |
| SpO2 umbilical vein | ~80% | N/A |
| SpO2 umbilical arteries | ~55-58% | N/A |
Sources: The Developing Human - Clinically Oriented Embryology (Moore), p.869-873; Langman's Medical Embryology, p.236-238; Guyton and Hall Textbook of Medical Physiology, p.1050-1053; Ganong's Review of Medical Physiology (26e), p.614; Harriet Lane Handbook 23e, p.651-652
Teach me like neonatologist/paeditrcian in depth topic -
This is a shared conversation. Sign in to Orris to start your own chat.