Dysplastic hip in adults for 10marks.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hip dysplasia" adults treatment
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information to write a thorough 10-mark answer on dysplastic hip in adults. Let me compose the full response:
Dysplastic Hip in Adults
Definition
Hip dysplasia (developmental dysplasia of the hip, DDH) in adults refers to a condition of inadequate coverage of the femoral head due to a shallow, maloriented acetabulum. It is one of the leading causes of hip pain in adults under 50 years and, if untreated, is a major precursor of early-onset hip osteoarthritis.
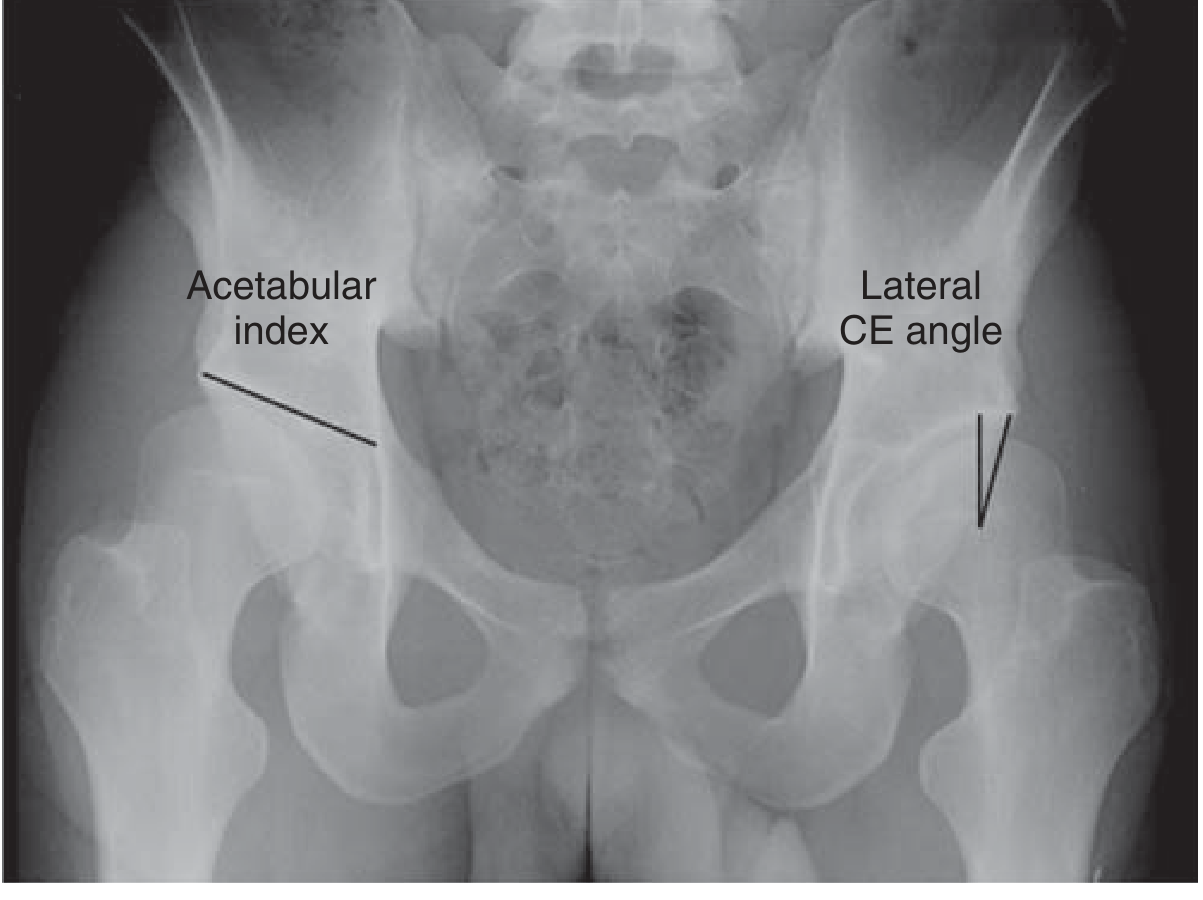
Radiographic Definitions (Box 5.1)
The classical radiographic criteria for acetabular dysplasia are measured on an AP pelvis radiograph:
| Parameter | Dysplastic Value |
|---|---|
| Lateral Center Edge (CE) angle | < 20° (normal ~30°) |
| Anterior CE angle | < 20° (on standing lateral view) |
| Acetabular index (Tonnis angle) | > 5–10° (normally horizontal) |
The lateral CE angle is the angle between a vertical line through the femoral head center and a line from the femoral head center to the lateral acetabular edge.
Anatomy of Adult Hip Dysplasia
1. Acetabular Side
- Shallow acetabulum with deficient anterior and lateral coverage
- Decreased acetabular depth (socket less than a hemisphere; upsloping acetabular index)
- Varying degrees of superolateral subluxation and lateralization of the femoral head
- High articular contact stresses concentrated near the superolateral rim - the mechanical basis for early cartilage damage
2. Proximal Femur
- High neck-shaft angle (coxa valga)
- Increased femoral anteversion
Crowe Classification
Used to grade femoral head subluxation in DDH adults:
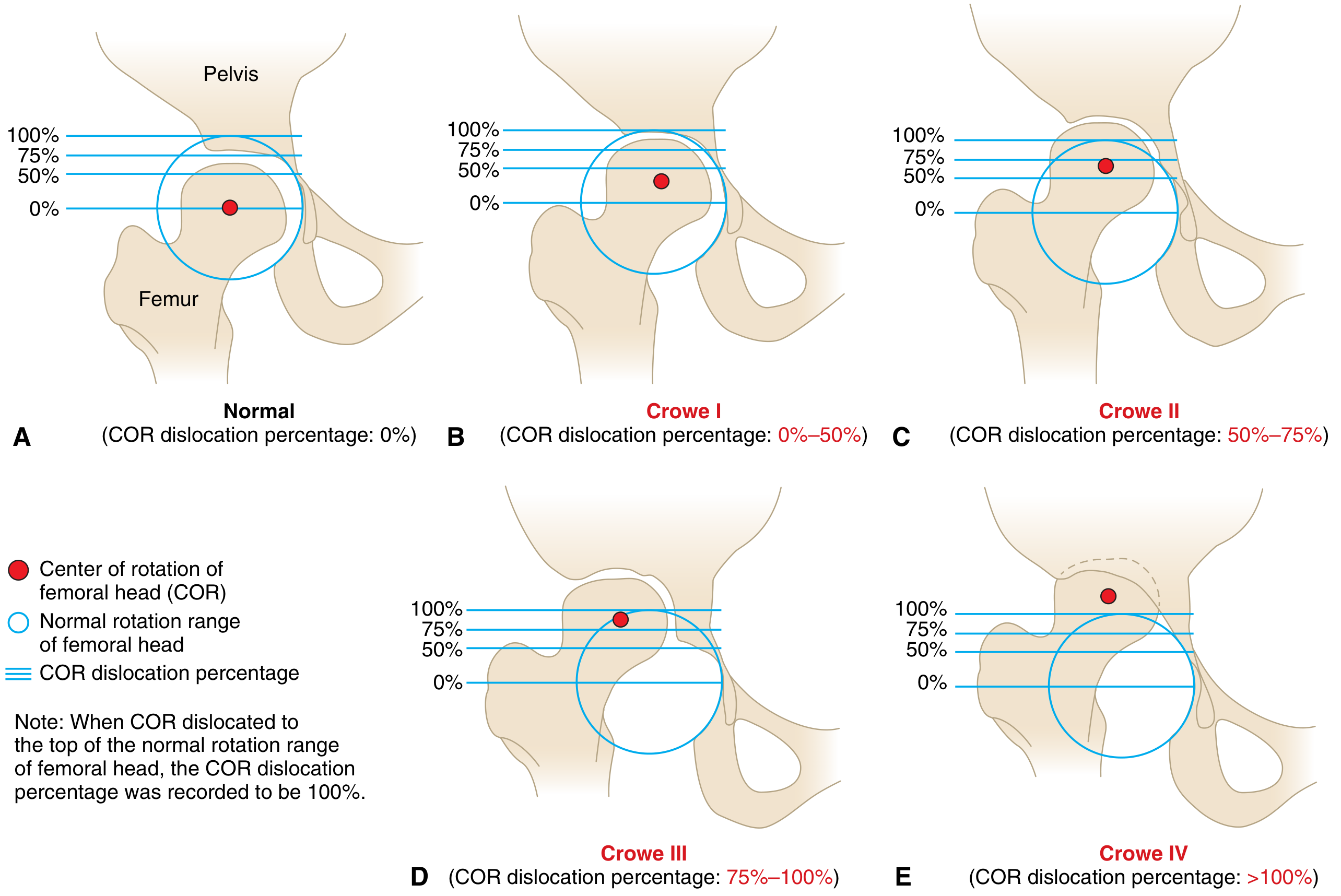
| Grade | Subluxation | Proximal Displacement |
|---|---|---|
| I (mild) | < 50% | < 10% |
| II | 50-75% | 10-15% |
| III | 75-100% | 15-20% |
| IV (severe) | > 100% | > 20% (deficient true acetabulum) |
Natural History
- Many mild cases are asymptomatic and go unrecognized on radiographs in childhood
- Hip pain in adults younger than 50 years is often the result of an underlying structural problem (dysplasia or FAI)
- Initial presentation of symptoms may be soon followed by rapid degeneration
- Abnormal biomechanics leads to progressive chondral damage and labral tears
- Untreated dysplasia progresses to secondary osteoarthritis (OA) - the main long-term sequela
Clinical Presentation (Spectrum)
- Presentation is often subtle; patients may describe it as a "groin pull"
- Anterior groin pain, aggravated by activity
- Mechanical symptoms (clicking, catching, giving way) from associated labral pathology
- Chondral surface delamination and chondral flap tears may also produce symptoms
- Examination: positive impingement test (flexion + adduction + internal rotation elicits groin pain), positive Stinchfield test
Investigations
Radiographs - Standard initial modality (AP pelvis, lateral views); measure CE angle and acetabular index.
CT scan (3D with pelvic remodeling) - Indicated for preoperative planning for reconstruction in dysplasia surgery and complex cases.
MRI / Gadolinium MR arthrogram - When labral pathology is suspected; may also identify associated chondral damage and labral tears.
Treatment
Treatment depends on the extent of deformity, location of the problem, patient age, and degree of secondary arthritis.
Goals of Surgical Correction
- Relieve pain
- Correct anatomic deformity
- Long-term: reduce the occurrence of degenerative joint disease (DJD)
Options
1. Non-operative Management
- Activity modification, physiotherapy, analgesia
- Appropriate in mild/asymptomatic cases or those unfit for surgery
2. Hip Arthroscopy
- For mild dysplasia with labral tears and early chondral damage
- Minimally invasive; rapid recovery but steep learning curve
- Limited role - does not address the underlying bony deformity
3. Periacetabular Osteotomy (PAO) - the gold standard hip preservation procedure
The most common technique used to correct acetabular tilt and version in the young adult with preserved joint space.
Technical features:
- The posterior column is preserved - maintains pelvic stability
- Does not violate the abductors
- Allows early weight bearing
- Permits significant correction of acetabular tilt and version
- Allows joint medialization (repositions center of hip rotation medially, lowering joint reactive forces)
Goals of PAO correction:
- Acetabular roof index to zero
- Lateral CE angle restored to normal range
- Appropriate socket anteversion restored
- Overcorrection (retroversion → secondary FAI) must be avoided
Conversion to THA after prior PAO:
- Previous hardware may be left in place if it does not interfere with acetabular component placement
- A retroverted socket from prior osteotomy means internal landmarks may not be reliable for cup positioning
4. Femoral Osteotomy
- Varus femoral osteotomy corrects excessive valgus neck-shaft angle (coxa valga) and lateral uncovering
- Typically reserved for pediatric patients; less commonly used in adults
- Can be combined with PAO in selected cases
5. Total Hip Arthroplasty (THA)
- Reserved for patients with established degenerative joint disease (DJD) who are no longer candidates for hip preservation
- Technical challenges in dysplastic THA: small true acetabulum, high-riding femoral head, short femoral canal, increased anteversion
Summary Table
| Feature | Detail |
|---|---|
| Definition | Under-coverage of femoral head (shallow acetabulum) |
| Key measurement | Lateral CE angle < 20°, Acetabular index > 10° |
| Classification | Crowe I-IV (based on femoral head subluxation %) |
| Pathology | Increased rim stress → labral tears → chondral damage → OA |
| Presentation | Groin pain, mechanical symptoms, positive impingement test |
| Gold standard surgery | Periacetabular Osteotomy (PAO) |
| End-stage disease | Total Hip Arthroplasty (THA) |
Sources:
- Miller's Review of Orthopaedics, 9th Edition, Section 2: Structural Hip Disorders in the Adult, pp. 422-425
- Bailey and Love's Short Practice of Surgery, 28th Edition, Ch. 39: Hip dysplasia in young adults, p. 575
Recent evidence note: A 2024 systematic review (PMID: 38919352) found that PAO in patients over 40 remains a viable option with acceptable outcomes in appropriately selected patients without significant pre-existing arthritis.
This is a shared conversation. Sign in to Orris to start your own chat.