Pansystolic murmur
Reading File
Finding Sources
Finding Sources
Searching PubMed
pansystolic murmur diagnosis causes
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks plus excellent diagrams. Here is the full answer:
Pansystolic (Holosystolic) Murmur
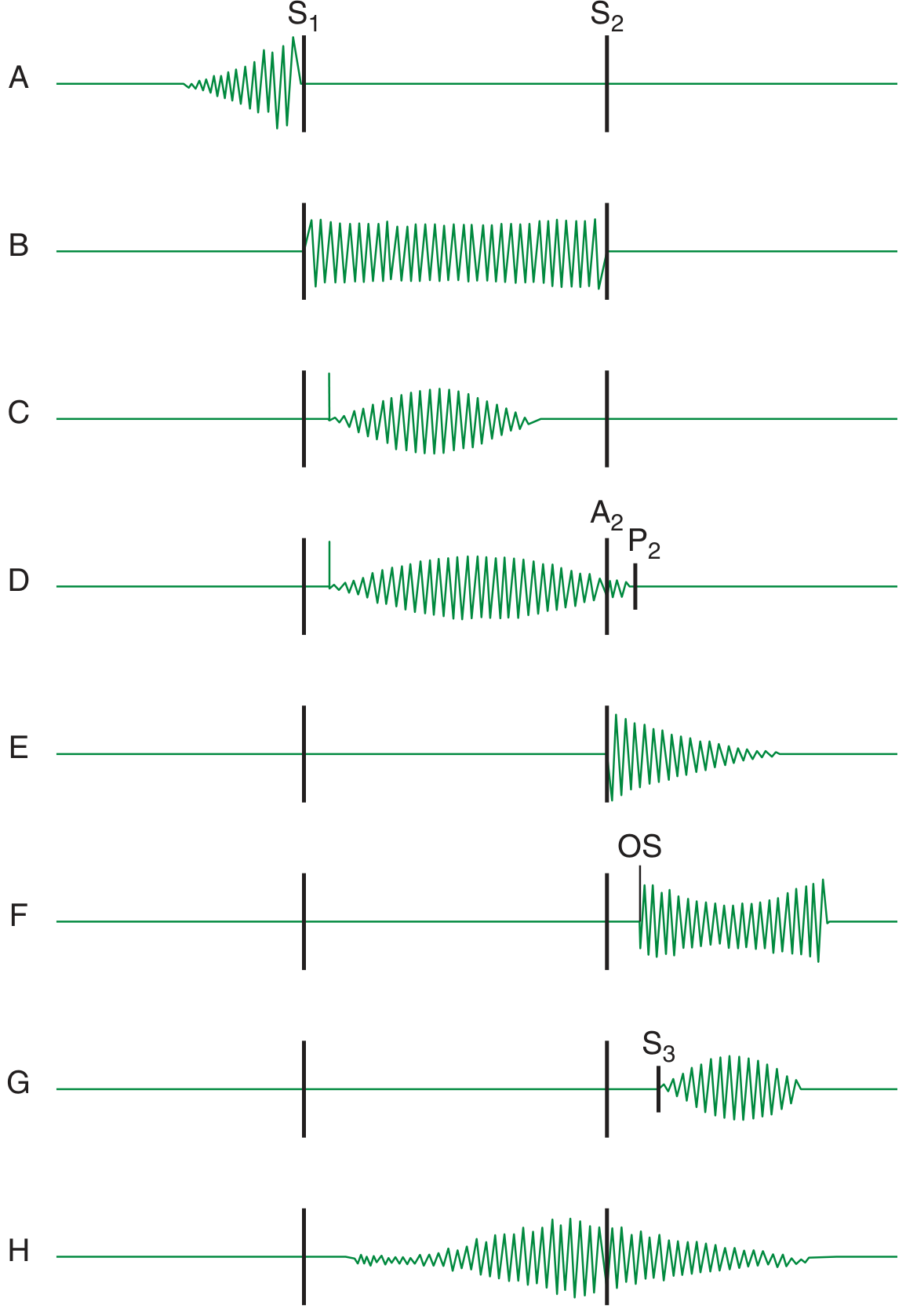
A pansystolic murmur occupies the entire systole from S1 to S2, without any gap on either side. It arises when there is a sustained pressure difference between two cardiac chambers throughout the whole of systole - the elevated pressure chamber continuously drives blood through an abnormal opening into the lower-pressure chamber from the moment the ventricle contracts until it relaxes.
Mechanism
The duration of a murmur depends on the length of time over which a pressure difference exists between two chambers. In pansystolic murmurs, the pressure gradient persists from the very onset to the very end of systole, so the murmur fills it completely without fading before S2. - Harrison's Principles of Internal Medicine 22E
The Three Classic Causes
1. Mitral Regurgitation (MR)
| Feature | Detail |
|---|---|
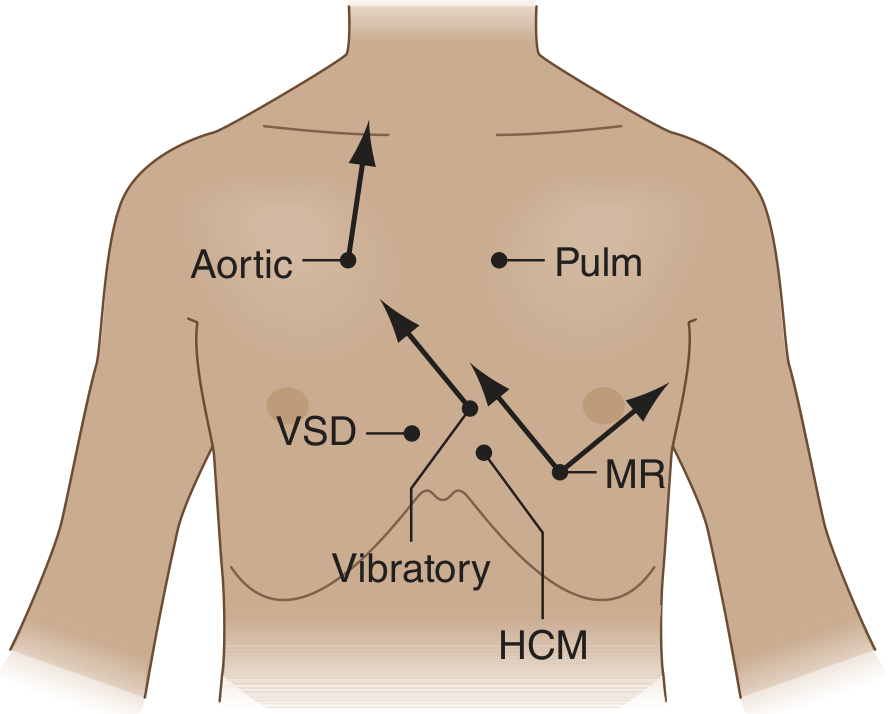
| Location | Apex / left lower sternal border |
| Radiation | Left axilla and back |
| Quality | High-pitched, blowing |
| Pitch | High frequency |
| Associated | S3 gallop, displaced apex beat, signs of left heart failure |
Mitral regurgitation results in a high-pitched pansystolic murmur that can overlap with S1 or S2. It is heard best at the left lower sternal border and apex, and may radiate to the left axilla and back. - Fuster and Hurst's The Heart, 15th Edition
In acute MR (e.g. papillary muscle rupture after MI, chordal rupture), the murmur is actually an early systolic decrescendo rather than pansystolic, because the sudden volume load into a non-compliant left atrium causes rapid equalisation of pressures. The classic pansystolic pattern is seen in chronic MR where the atrium has had time to dilate and remain compliant. - Harrison's, 22E
Causes of MR: rheumatic heart disease, myxomatous degeneration (MVP), infective endocarditis, papillary muscle dysfunction (ischaemia), dilated cardiomyopathy (functional MR), connective tissue disorders.
Bedside maneuver: The intensity of MR is constant from beat to beat (unlike AS, which increases after a premature beat). MR murmur increases with handgrip (increased afterload, more regurgitation) and decreases with amyl nitrite (reduced afterload). - Harrison's, 22E
2. Tricuspid Regurgitation (TR)
| Feature | Detail |
|---|---|
| Location | Lower left sternal border / subxiphoid |
| Radiation | Precordium if RV dilated; may mimic MR at apex |
| Quality | High-pitched when associated with pulmonary hypertension |
| Key sign | Increases with inspiration (Carvallo's sign / Rivero-Carvallo sign) |
| Associated | Prominent cv waves in JVP, pulsatile liver, RV heave |
When TR occurs in the presence of pulmonary hypertension, the systolic murmur is high-pitched, pansystolic, and loudest in the fourth intercostal space in the parasternal region but occasionally loudest in the subxiphoid area. When the right ventricle is greatly dilated and occupies the anterior surface of the heart, the murmur may be prominent at the apex and difficult to distinguish from MR. - Braunwald's Heart Disease, 2-Vol Set
TR without pulmonary hypertension (e.g. infective endocarditis, trauma) produces only a soft, early systolic murmur - not pansystolic.
Causes of TR: most commonly functional (RV dilatation from pulmonary hypertension, dilated cardiomyopathy); primary causes include rheumatic disease, infective endocarditis (especially in IV drug users), carcinoid syndrome, Ebstein's anomaly, radiation-induced, trauma. - Braunwald's Heart Disease
Key distinguishing feature from MR: Increases in intensity during inspiration (Rivero-Carvallo sign) - increased venous return to the right heart augments the regurgitant volume.
3. Ventricular Septal Defect (VSD)
| Feature | Detail |
|---|---|
| Location | Left sternal border (3rd-4th intercostal space) |
| Radiation | Throughout precordium |
| Quality | Harsh, loud (often with thrill) |
| Associated | Thrill in ~50%, signs of left heart volume overload |
The typical murmur associated with a VSD is harsh, pansystolic, and best heard at the lower left sternal border. In a membranous (perimembranous) VSD, the LV-RV pressure gradient is maintained throughout systole, producing the holosystolic character. A systolic thrill at the left sternal border is present in nearly all patients with post-MI ventricular septal rupture. - Harrison's 22E / Swanson's Family Medicine Review
Important caveat: In small muscular VSDs, septal contraction progressively closes the defect during systole, so the murmur is confined to early systole only - not pansystolic. In large VSDs complicated by Eisenmenger syndrome (severe pulmonary hypertension with reversed shunt), the LV-RV gradient is abolished and the murmur may disappear entirely. - Harrison's, 22E
Differentiating the Three Causes at the Bedside
| Feature | MR | TR | VSD |
|---|---|---|---|
| Best heard | Apex | Lower LSB / subxiphoid | 3rd-4th ICS LSB |
| Radiation | Left axilla | Precordium | Across precordium |
| Respiratory change | No change | Increases on inspiration | No change |
| Valsalva | Decreases | Decreases | Decreases |
| Handgrip | Increases | No change | Increases |
| Thrill | Occasionally | Rarely | Common (especially post-MI VSD) |
| JVP | Normal (unless PHT) | Prominent cv wave | Normal |
| Associated sounds | S3 at apex | S3 (right-sided, inspiration) | Thrill, S2 may be loud |
| Key clue | Displaced apex, AF | Pulsatile liver, edema | Harsh murmur, post-MI setting |
Additional/Rarer Causes
- Functional MR in dilated cardiomyopathy - a pansystolic murmur may be heard at the apex radiating to the axilla, but frequently no murmur is audible even with significant MR if cardiac output is very low. - Goldman-Cecil Medicine
- Functional TR with severe pulmonary hypertension from any cause (MS, PHT) - a pansystolic TR murmur along the left sternal border may develop. - Harrison's, 22E
- Post-MI ventricular septal rupture - distinguishable from papillary muscle rupture (acute MR) by: (a) pansystolic vs early systolic murmur; (b) thrill at LSB in VSD; (c) right-sided heart catheterization showing step-up in O2 saturation in the RV/PA (VSD) vs tall V-wave in PCWP (MR). - Harrison's, 22E
Bedside Maneuvers Summary
- Inspiration - selectively increases right-sided murmurs (TR) - Rivero-Carvallo sign
- Expiration - selectively increases left-sided murmurs (MR)
- Handgrip - increases systemic vascular resistance, augments MR and VSD murmurs
- Valsalva - decreases preload, reduces all three; on release, right-sided murmurs return first
- Amyl nitrite - decreases afterload, reduces MR; increases VSD murmur (increases LV-RV gradient)
- Squatting - increases preload and afterload, augments MR and TR
Investigations
- Echocardiography (TTE/TOE) - primary modality; confirms diagnosis, quantifies severity, assesses ventricular function and pulmonary pressures. Colour flow Doppler is definitive. Suspicion of VSD, MR, or TR is an indication for TTE. - Fuster & Hurst's 15th Ed.
- ECG - may show LA enlargement (MR), RVH (TR with PHT), or signs of MI (post-MI VSD/MR)
- Chest X-ray - cardiomegaly, pulmonary venous congestion (MR), right heart enlargement (TR)
- Cardiac catheterization - used in complex cases; serial O2 saturations distinguish VSD from MR
This is a shared conversation. Sign in to Orris to start your own chat.