High bp
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"hypertension" AND "treatment" AND "guidelines"
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information to give a thorough answer. Here it is:
Treatment of High Blood Pressure (Hypertension)
BP Classification & Treatment Thresholds (ACC/AHA 2017)
| Category | Systolic | Diastolic | Action |
|---|---|---|---|
| Normal | <120 | <80 | No intervention |
| Elevated | 120-129 | <80 | Lifestyle modification only |
| Stage 1 HTN | 130-139 | 80-89 | Lifestyle ± drug therapy (based on CVD risk) |
| Stage 2 HTN | ≥140 | ≥90 | Lifestyle + drug therapy |
| Target (treated) | <130 | <80 | - |
- The ACC/AHA 2017 guidelines define hypertension at ≥130/80 mm Hg
- European (ESC/ESH 2018) and NICE 2019 guidelines define it at ≥140/90 mm Hg - so thresholds differ depending on which guideline is followed
Step 1 - Lifestyle Modifications
These can lower systolic BP by 7-15 mm Hg and should be tried first in Stage 1 low-risk patients, and continued alongside medications in everyone:
- Diet: Mediterranean or DASH diet - high in fruits, vegetables, whole grains, low-fat dairy, fish; low in refined carbs and saturated fats
- Sodium: Reduce to <1,500 mg/day (most sodium comes from processed foods, not added salt)
- Exercise: 90-150 min/week of moderate aerobic or dynamic resistance training (lowers BP by ~4-8 mm Hg)
- Alcohol: ≤2 drinks/day for men, ≤1 drink/day for women
- Weight loss, smoking cessation, stress management also contribute
Step 2 - Drug Therapy: The Four Core Classes
Current US and European guidelines converge on four preferred drug classes:
| Class | Examples | Mechanism | Key Notes |
|---|---|---|---|
| ACE Inhibitors | Lisinopril, Ramipril | Block angiotensin I → II conversion | First-line; avoid in pregnancy, bilateral RAS, hyperkalemia; causes dry cough |
| ARBs (Angiotensin Receptor Blockers) | Losartan, Valsartan | Block angiotensin II at AT1 receptor | Same profile as ACEi, no cough; avoid in pregnancy |
| CCBs (Calcium Channel Blockers) | Amlodipine (DHP), Diltiazem/Verapamil (non-DHP) | Vasodilation, reduce cardiac contractility | Non-DHPs: avoid in AV block, severe LV dysfunction |
| Thiazide/Thiazide-like Diuretics | Hydrochlorothiazide, Chlorthalidone (preferred in US) | Reduce sodium absorption | Avoid in gout; caution in metabolic syndrome, hypokalemia |
Beta-blockers are no longer first-line unless there is a specific compelling indication (angina, heart failure with reduced EF, atrial fibrillation for rate control, post-MI).
Step 3 - How to Start and Escalate
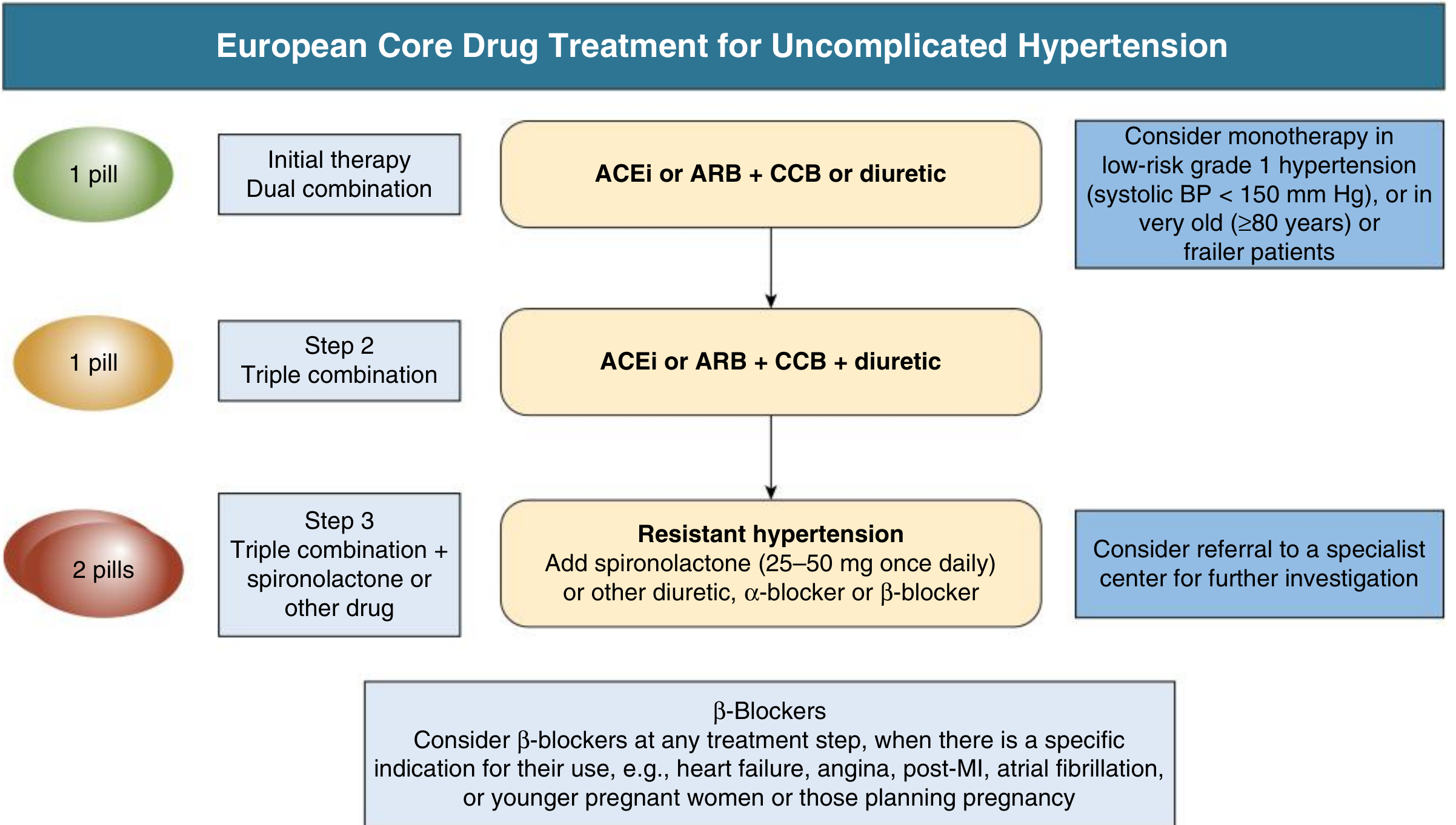
From: Comprehensive Clinical Nephrology, 7th Ed.
Step 1 (Initial - Dual Combination): ACEi or ARB + CCB or Diuretic
- Monotherapy considered only in low-risk Grade 1 HTN (SBP <150) or frail elderly (≥80 years)
Step 2 (Triple Combination): ACEi or ARB + CCB + Diuretic
Step 3 (Resistant HTN): Add spironolactone 25-50 mg once daily, or an alpha-blocker or beta-blocker; refer to specialist
Most patients require ≥2 drugs to achieve target. Single-pill combinations are strongly preferred to reduce pill burden and improve adherence - roughly 50% of patients stop antihypertensives within 1 year, and 20% never fill the first prescription.
Compelling Indications - Choose Specific Drug Classes
| Comorbidity | Preferred Agents |
|---|---|
| Heart failure (reduced EF) | ACEi/ARB + beta-blocker + aldosterone antagonist |
| Post-MI / CAD | Beta-blocker + ACEi/ARB |
| Chronic kidney disease | ACEi or ARB (slow progression, reduce proteinuria) |
| Diabetes | ACEi or ARB (renal protection) |
| Stroke / cerebrovascular disease | ACEi + thiazide diuretic |
| Atrial fibrillation | Beta-blocker or non-DHP CCB (rate control) |
| Pregnancy | Labetalol, nifedipine, methyldopa; avoid ACEi/ARBs |
Contraindications Summary
| Drug | Hard Contraindications |
|---|---|
| ACEi | Pregnancy, angioedema, hyperkalemia, bilateral renal artery stenosis |
| ARB | Pregnancy, hyperkalemia, bilateral renal artery stenosis |
| Non-DHP CCB | AV block grade 2-3, severe LV dysfunction |
| Thiazides | Gout |
| Beta-blockers | Asthma, AV block grade 2-3 |
| MRAs (spironolactone) | Hyperkalemia, creatinine >2.5 mg/dL (men) or >2.0 mg/dL (women) |
Key Takeaways
- Most patients need at least 2 drugs - don't wait with monotherapy if BP is significantly elevated
- Foundation of therapy: RAS blockade (ACEi or ARB) is the backbone for most patients
- Single-pill combinations improve adherence significantly
- Lifestyle modification is always concurrent with medications, not replaced by them
- Each 5 mm Hg reduction in SBP corresponds to ~10% reduction in cardiovascular events
Sources: Comprehensive Clinical Nephrology 7th Ed.; Goldman-Cecil Medicine; The Washington Manual of Medical Therapeutics; Goodman & Gilman's Pharmacological Basis of Therapeutics
Disclaimer: This is educational information only. Antihypertensive treatment should be individualized by a healthcare provider based on the patient's full clinical picture, comorbidities, and lab values.
This is a shared conversation. Sign in to Orris to start your own chat.