

00573747-38b6-4d7f-8f54-5734263af256.jpeg
6a0c5a79-7f13-4433-965f-2f463a531f41.jpeg
Interpret for an 80 year old male having burning sensation in urine
analyse_media
analyse_media
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have sufficient information to provide a thorough interpretation. Let me compile the full clinical analysis.
Ultrasound Report Interpretation - 80-Year-Old Male with Dysuria (Burning Urination)
The patient had two separate USG scans (likely done at different times or centers). Here is a combined interpretation:
Findings Summary
Report 1
| Structure | Finding |
|---|---|
| Spleen | Normal size (72 mm), homogeneous |
| Abdomen | No ascites, no retroperitoneal lymphadenopathy |
| Urinary Bladder | Normal size/echotexture, bladder wall thickening (5 mm), low-level internal echoes, pre-void ~100 cc |
| Prostate | Enlarged: 57 x 40 x 37 mm, volume 44.25 cc |
| Impression | Grade II Fatty Liver, Right Renal Simple Cortical Cyst (Bosniak I), Grade II BPH, Cystitis |
Report 2
| Structure | Finding |
|---|---|
| Bladder | Well distended, normal wall thickness |
| Pre-void | 149 cc, post-void residual urine (PVRU) = 35.9 cc (significant) |
| Prostate | Enlarged ~49 cc |
| Impression | Grade II Fatty Liver, Right Renal Cortical Cyst, Prostatomegaly with significant PVRU |
Detailed Clinical Interpretation
1. Benign Prostatic Hyperplasia (BPH) - Grade II / Prostatomegaly
This is the central finding driving all urinary symptoms.
- Normal prostate volume in an adult male is 20-30 cc. This patient's prostate measures 44-49 cc - approximately 1.5 to 2x the normal size
- This qualifies as Grade II BPH (moderate enlargement)
- The enlarged prostate causes bladder outlet obstruction (BOO), leading to:
- Incomplete bladder emptying
- Increased intravesical pressure
- Bladder wall hypertrophy (explaining the 5 mm wall thickening seen in Report 1; normal is < 3-4 mm in a full bladder)
- Urinary stasis favoring bacterial colonization
At age 80, BPH is extremely common. As per Campbell-Walsh Urology, the risk of requiring intervention for BPH increases progressively with age and prostate volume. A volume >40 cc is associated with higher risk of acute urinary retention and progression.
2. Cystitis (Bladder Infection)
This is the direct cause of the burning sensation (dysuria).
- The bladder wall thickening to 5 mm and low-level internal echoes within the bladder on USG are classic sonographic signs of cystitis (inflammatory/infective thickening of the bladder mucosa)
- In this patient, cystitis is secondary to BPH - the enlarged prostate leads to urinary stasis and incomplete voiding, which provides a fertile medium for bacterial growth
- As per Campbell-Walsh Urology: "acute onset of dysuria and acute change in baseline voiding symptoms are most consistent with a diagnosis of acute uncomplicated cystitis" - exactly this patient's presentation
- In elderly men, the most common pathogens are E. coli, Klebsiella, Proteus (gram-negative rods)
- Important note: UTI/cystitis in men is considered complicated UTI (unlike women) because there is almost always an underlying structural or functional cause (here: BPH with urinary stasis)
3. Post-Void Residual Urine (PVRU) = 35.9 cc
- Normal PVRU is < 50 cc. A value of 35.9 cc is technically within borderline range, but the report labels it "significant" in the clinical context of prostatomegaly
- Elevated PVRU confirms incomplete bladder emptying due to BPH obstructing outflow
- Persistent PVRU predisposes to recurrent UTIs and, if untreated, can progress to bladder decompensation, hydronephrosis, and renal impairment
4. Right Renal Simple Cortical Cyst - Bosniak Grade I
- A Bosniak Grade I cyst is a simple benign cyst - thin-walled, anechoic, no septations, no solid components
- No treatment or follow-up required for Bosniak I
- Not related to urinary symptoms
5. Grade II Fatty Liver (Hepatic Steatosis)
- Incidental finding; moderate hepatic fat infiltration
- Not related to the presenting complaint of burning urination
- May warrant metabolic workup (lipid profile, blood glucose, liver function tests)
Clinical Correlation and Recommended Next Steps
| Priority | Action |
|---|---|
| Urgent | Urine routine microscopy + culture & sensitivity - to identify the causative organism and guide antibiotic selection |
| Urgent | Antibiotics - in elderly men with complicated UTI, a fluoroquinolone (Ciprofloxacin) or trimethoprim-sulfamethoxazole for 7-14 days (based on culture) is typically used. Nitrofurantoin should be avoided in elderly men (reduced renal function risk) |
| Important | Serum PSA - to help differentiate BPH from prostate carcinoma (prostate volume ~44-49 cc warrants this; inflammation can transiently raise PSA, so recheck after treating infection) |
| Important | BPH management - Start alpha-1 blocker (e.g., Tamsulosin 0.4 mg OD) to relax prostatic smooth muscle and improve urine flow; add 5-alpha reductase inhibitor (e.g., Finasteride or Dutasteride) for long-term prostate volume reduction |
| Monitor | Serum creatinine + eGFR - to assess renal function given long-standing prostatic obstruction at age 80 |
| Monitor | Uroflowmetry + repeat PVRU after treating UTI and starting BPH medications |
| If refractory | Urology referral for possible TURP (transurethral resection of prostate) if medical management fails |
Summary for the Patient's Family
This 80-year-old gentleman has an enlarged prostate (~1.5-2x normal size) that is blocking normal urine flow. Urine is not fully emptying from the bladder, and this stagnant urine has developed a bladder infection - which is causing the burning sensation. There is also a harmless fluid cyst on the right kidney and mild fatty changes in the liver (unrelated to urinary symptoms). He needs antibiotics for the infection (guided by urine culture) and medications for the enlarged prostate to prevent recurrence. A urology consultation is recommended.
Disclaimer: This is an educational interpretation for informational purposes. Treatment decisions must be made by the treating physician after full clinical examination, laboratory workup, and appropriate history.
Treatment for bph and uti in this patient
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"benign prostatic hyperplasia" AND treatment AND "alpha blocker"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
I now have everything needed for a complete, evidence-based treatment plan. Here is the full answer:
Treatment Plan: BPH + UTI (Cystitis) in an 80-Year-Old Male
PART 1 - Treating the UTI (Immediate Priority)
Why this is a Complicated UTI
UTI in an elderly male is never considered uncomplicated. Per Bailey & Love's Surgery: male gender, age, and a functional urinary tract abnormality (BPH causing bladder outlet obstruction + urinary stasis) are all factors that classify this as a complicated UTI. The organisms responsible are: E. coli (50%), Enterococci, Klebsiella, Pseudomonas - a broader spectrum than simple female cystitis.
Step 1 - Urine Culture First
- Send urine for routine microscopy + culture & sensitivity (C&S) before starting antibiotics (ideally midstream clean-catch)
- Start empiric antibiotics simultaneously; adjust once C&S report is available (48-72 hrs)
Step 2 - Antibiotic Selection
| Drug | Dose | Duration | Notes |
|---|---|---|---|
| Ciprofloxacin (preferred 1st line) | 500 mg PO twice daily | 7-14 days | Fluoroquinolone; achieves excellent urinary & tissue penetration; good for complicated UTI |
| Levofloxacin (alternative) | 750 mg PO once daily | 5-7 days | Once-daily dosing, good compliance |
| Trimethoprim-Sulfamethoxazole (Co-trimoxazole) | 960 mg PO twice daily | 10-14 days | Use only if local resistance rates <20% |
| Nitrofurantoin | ❌ AVOID | - | Poor tissue penetration; not for complicated UTI; use with caution in elderly due to reduced renal clearance |
Per Katzung's Pharmacology: "A fluoroquinolone that achieves good urinary and systemic levels (ciprofloxacin or levofloxacin) would be a reasonable choice for empiric treatment of complicated urinary tract infection."
Important: Check eGFR/creatinine before prescribing - dose-adjust ciprofloxacin if eGFR < 30 mL/min.
Step 3 - Supportive Measures
- Oral hydration - increase fluid intake to 2-3 L/day to flush bacteria
- Urinary analgesic - Phenazopyridine 200 mg TDS for 1-2 days for immediate symptom relief (turns urine orange - warn the patient)
- Avoid catheterization unless urinary retention develops - catheters increase risk of resistant organisms
PART 2 - Treating BPH (Prostate Volume ~44-49 cc, Grade II)
This patient has an enlarged prostate with bladder wall thickening and borderline PVRU - the combination of an alpha-blocker + 5-alpha reductase inhibitor is the optimal long-term strategy for a prostate >40 cc.
Drug Class Comparison (from Lippincott Pharmacology)
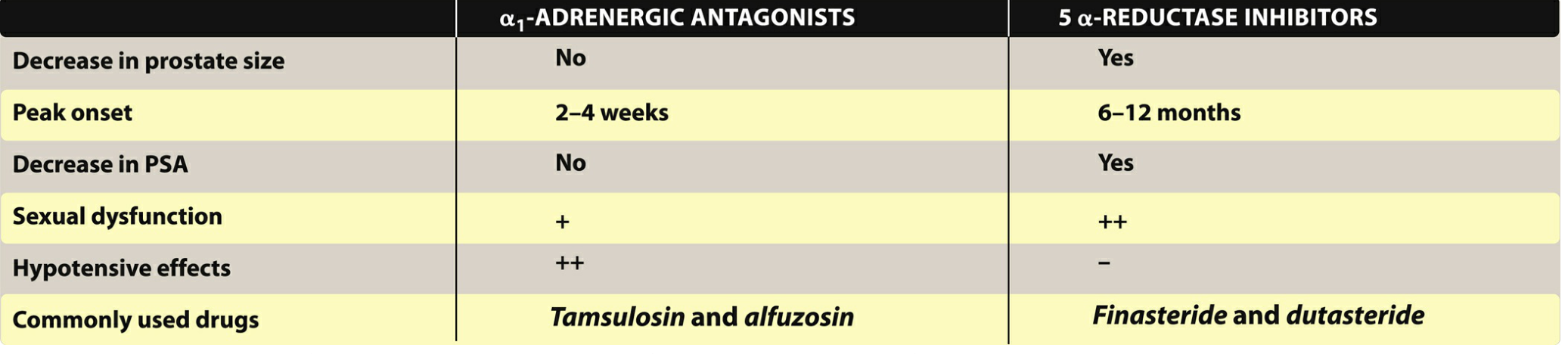
Drug 1 - Alpha-1 Blocker (Start immediately - symptom relief in 2-4 weeks)
Tamsulosin 0.4 mg orally once daily (30 min after a meal)
- Mechanism: Blocks alpha-1A receptors in prostatic smooth muscle → relaxes urethral resistance → better urine flow
- Most suitable for an 80-year-old because it is prostate-selective (alpha-1A > alpha-1B) - minimal blood pressure drop compared to doxazosin or terazosin (critical in elderly at risk of orthostatic hypotension and falls)
- Onset: symptom relief in 2-4 weeks
- Side effects to counsel: retrograde ejaculation, dizziness, nasal congestion
- Caution - Intraoperative Floppy Iris Syndrome (IFIS): If this patient ever needs cataract surgery, inform the ophthalmologist that he is on tamsulosin
Alternative: Alfuzosin 10 mg OD (also prostate-selective, possibly fewer ejaculatory side effects)
Drug 2 - 5-Alpha Reductase Inhibitor (Long-term prostate shrinkage - takes 6-12 months)
Finasteride 5 mg orally once daily OR Dutasteride 0.5 mg orally once daily
- Mechanism: Inhibits conversion of testosterone → DHT (dihydrotestosterone). DHT drives prostate growth. By reducing DHT, the prostate physically shrinks over time (typically 20-30% reduction)
- Finasteride takes 6-12 months for full effect; dutasteride is more potent (inhibits both type 1 and type 2 5-alpha reductase)
- Only effective when prostate is enlarged - this patient qualifies (44-49 cc vs normal 20-30 cc)
- Side effects: decreased libido, erectile dysfunction, gynecomastia, reduced ejaculate volume
- Important PSA note: 5-alpha reductase inhibitors reduce PSA by ~50% after 6 months. The baseline PSA must be checked before starting and then multiplied by 2 when interpreting future PSA values to screen for prostate cancer
Combination Therapy
Per Symptom to Diagnosis (Evidence-Based Guide): "Combination therapy with an alpha-blocker and 5-alpha reductase inhibitor is more effective than monotherapy."
- The MTOPS trial and CombAT trial established that combination therapy (tamsulosin + dutasteride) is superior for prostate volumes >40 cc
- A fixed-dose combination is available: Duodart (dutasteride 0.5 mg + tamsulosin 0.4 mg) once daily for convenience
When to Consider Surgery (TURP)
Refer to a urologist for Transurethral Resection of the Prostate (TURP) if:
- Symptoms do not improve after 3-6 months of combination medical therapy
- Progressive increase in PVRU (>200 cc)
- Acute urinary retention (inability to void)
- Recurrent UTIs due to urinary stasis
- Hydronephrosis develops on repeat ultrasound
Summary Drug Chart for This Patient
| Drug | Dose | Indication | When to Expect Effect |
|---|---|---|---|
| Ciprofloxacin 500 mg | BD x 10-14 days | UTI/Cystitis | 48-72 hrs (symptom relief) |
| Tamsulosin 0.4 mg | OD after meal | BPH - symptom relief | 2-4 weeks |
| Dutasteride 0.5 mg | OD | BPH - prostate shrinkage | 6-12 months |
| Phenazopyridine 200 mg | TDS x 2 days | Dysuria (symptom relief only) | Immediate |
Monitoring Plan
| Test | Timing | Purpose |
|---|---|---|
| Urine C&S report | 48-72 hrs | Antibiotic adjustment |
| Serum creatinine + eGFR | Now | Assess renal function from chronic obstruction |
| Serum PSA | After UTI resolves (4-6 weeks) | Prostate cancer screening baseline (UTI falsely elevates PSA) |
| Repeat USG with PVRU | 3-6 months | Assess treatment response |
| Blood pressure sitting/standing | Each visit | Orthostatic hypotension monitoring (especially with alpha-blocker in elderly) |
Sources: Lippincott Illustrated Reviews Pharmacology | Campbell-Walsh Urology | Symptom to Diagnosis (4th Ed.) | Bailey & Love's Surgery (28th Ed.) | Katzung's Basic & Clinical Pharmacology | AUA BPH Guideline 2026 (PMID 42095481)
This information is for clinical education. All prescribing decisions must be made by the treating physician after full patient evaluation.
This is a shared conversation. Sign in to Orris to start your own chat.