Febella Orthopedics what's it etiology pathology signs symptoms and investigations treatment explain everything with appropriate illustrative diagrams for 10 marks
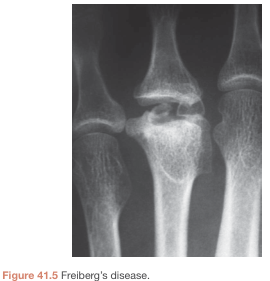
Freiberg disease metatarsal osteochondrosis X-ray
Smillie classification Freiberg infraction stages metatarsal
Freiberg disease Smillie classification stages etiology pathology treatment orthopedics
Freiberg's Disease (Freiberg's Infraction / Osteochondrosis of the Metatarsal Head)
Note: "Febella Orthopedics" in your question refers to Freiberg's Disease — an osteochondrosis/avascular necrosis of the metatarsal head, a classic orthopedics topic.
1. Definition
- First described by Alfred Henry Freiberg in 1914
- The term "infraction" (from the Latin infractio, to break) refers to the subchondral fracture that initiates the process
2. Etiology
| Factor | Detail |
|---|---|
| Repetitive trauma / overload | Most accepted cause — repetitive compressive forces on the metatarsal head disrupt subchondral blood supply |
| Long second metatarsal | A disproportionately long 2nd metatarsal increases local stress concentration at the metatarsal head |
| Gastrocnemius contracture | Tight calf muscles increase forefoot loading during gait |
| Hallux valgus / 1st ray insufficiency | Transfers load to the lesser rays, particularly the 2nd |
| High-heeled footwear | Increases forefoot pressures, especially in adolescent females |
| Vascular insufficiency | The metatarsal head has a relatively tenuous blood supply through end-arteries in the metaphysis, making it susceptible to ischaemia |
| Female sex / adolescent age | Female : Male ratio ≈ 5:1; onset typically 13–18 years |
"A long second metatarsal may be a risk factor (additionally, gastrocnemius contracture may be associated)." — Miller's Review of Orthopaedics, 9th Ed.
- 2nd metatarsal: >66% of cases
- 3rd metatarsal: most remaining cases
- 4th metatarsal: <5%
- 1st and 5th: rarely affected
3. Pathology
Vascular insult to metatarsal head epiphysis
↓
Subchondral bone ischaemia → necrosis
↓
Loss of structural support → subchondral fracture (infraction)
↓
Central collapse and flattening of metatarsal head
↓
Bony resorption, marginal osteophyte formation
↓
Fragmentation → intra-articular loose bodies
↓
End-stage degenerative joint disease
4. Smillie Classification (1967)
| Stage | Features |
|---|---|
| I | Subtle subchondral fracture (fissure in the epiphysis); often only visible on MRI |
| II | Earliest plain-film changes — mild central flattening/sinking of the dorsal metatarsal head |
| III | Further flattening and resorption; medial and lateral bony projections (marginal osteophytes) develop |
| IV | Osteophytes fracture → intra-articular loose bodies; plantar cartilage becomes damaged |
| V | End-stage arthrosis — marked flattening, widening, joint space obliteration |
5. Signs & Symptoms
Symptoms
- Pain over the affected metatarsal head — worse on weight-bearing and activity, relieved by rest
- Swelling around the metatarsophalangeal (MTP) joint
- Stiffness of the MTP joint, particularly dorsiflexion
- Gradual onset; may follow a period of increased activity
Signs
- Localised tenderness on direct palpation of the affected metatarsal head
- Swelling / fullness of the MTP joint
- Restricted range of motion at the MTP joint, especially dorsiflexion
- Antalgic gait — patient offloads the affected forefoot
- In late stages: palpable osteophytes, crepitus, and a widened toe or splayed forefoot
- MTP joint effusion may be palpable
- No systemic features (no fever, no lymphadenopathy)
6. Investigations
Plain Radiograph (First-line)
- May be normal in Stage I
- Subtle widening of MTP joint space (3–6 weeks after onset)
- Flattening of the metatarsal head (pathognomonic)
- Subchondral sclerosis and lucency
- Marginal osteophyte formation
- Osteochondral loose bodies
- Joint space narrowing in advanced disease


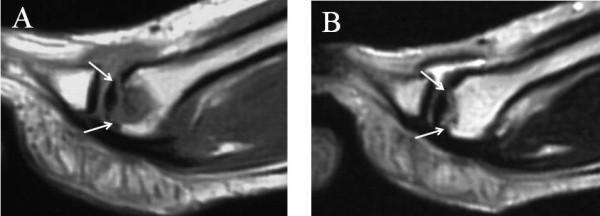
MRI (Gold Standard for Early Disease)
- Most sensitive for detecting Stage I disease (before plain film changes)
- T1-weighted: Low-signal (hypointense) area in the metatarsal head = necrotic bone/fibrous replacement
- T2-weighted: High-signal (hyperintense) = subchondral oedema, fluid accumulation
Bone Scan
- Increased uptake in the affected metatarsal head in active disease
- Useful when MRI is unavailable; less specific
Laboratory Tests
- Usually not diagnostic but may be performed to exclude:
- Infection (WBC, CRP, ESR)
- Rheumatoid arthritis (RF, anti-CCP)
- Gout (serum uric acid)
- Tumour
7. Treatment
A. Conservative (Non-operative) — First-line for ALL stages
| Modality | Details |
|---|---|
| Activity modification | Reduce high-impact activities (running, jumping) |
| Rest + protected weight-bearing | Short-term immobilisation in cast or boot |
| Shoe modification | Hard-soled shoes to reduce forefoot flexion stress |
| Metatarsal bar/pad orthotics | Transfers load proximally, away from the metatarsal head |
| NSAIDs | Analgesia and anti-inflammatory effect |
| Physiotherapy | Stretching gastrocnemius-soleus complex, low-impact strengthening |
"Common strategies consist of activity modification, shoe wear modification (hard sole), orthotics (metatarsal bar), and a period of protected weight bearing." — Miller's Review of Orthopaedics, 9th Ed.
B. Operative Treatment — For failed conservative management (Smillie III–V)
1. Joint Débridement (Stage II–III)
- Dorsal incision to the MTP joint
- Excision of inflamed synovium, loose bodies, osteophytes, and necrotic bone
- Indication: Relatively intact articular surface, minimal metatarsal deformity
- Good results in early-to-moderate disease
2. Dorsal Closing-Wedge Osteotomy (Gauthier/Weil) — Procedure of Choice (Stage III–IV)
- A dorsal wedge of bone is removed from the metatarsal neck/head
- The metatarsal head is plantarflexed — this rotates the healthy plantar articular cartilage (which is spared in Freiberg's) dorsally into a weight-bearing position
- Performed with thorough débridement
- Good to excellent results in the majority of studies

"Dorsal closed-wedge metaphyseal osteotomy … serves to rotate the plantar aspect of the articular surface, which is typically well preserved, to a more superior position, where it then articulates with the phalanx." — Miller's Review of Orthopaedics, 9th Ed.
3. Core Decompression
- Used in very early disease (Stage I–II)
- Drilling of the metatarsal head to decompress intraosseous pressure and stimulate revascularisation
4. Metatarsal Head Excision / Resection Arthroplasty (Stage V)
- For severe end-stage arthrosis refractory to other measures
- Excision of the whole metatarsal head should NOT be performed (leads to transfer metatarsalgia)
- Acceptable: excision of the proximal phalangeal base in adults with joint destruction
- Silicone or implant arthroplasty has been described but carries risk of silicone synovitis
"Reshaping osteotomies are described, or excision of the proximal phalangeal head for severe adult cases with joint destruction. Excision of the whole metatarsal head should never be performed." — Bailey & Love's Surgery, 28th Ed.
8. Prognosis
- Early disease (Stages I–II): Usually resolves well with conservative treatment; remodelling can occur in skeletally immature patients
- Moderate disease (Stages III–IV): Good results with dorsal osteotomy + débridement
- Late disease (Stage V): Chronic pain, stiffness, and transfer metatarsalgia are common; salvage procedures have variable outcomes
- Key principle: Early diagnosis and early treatment prevent progression to advanced arthrosis
Summary Table
| Aspect | Key Point |
|---|---|
| Definition | Avascular necrosis of lesser metatarsal head |
| Most common site | 2nd metatarsal (>2/3 cases) |
| Demographics | Adolescent/young adult females (F:M = 5:1) |
| Key etiology | Repetitive trauma + vascular insufficiency; long 2nd metatarsal |
| Pathology | Subchondral fracture → collapse → fragmentation → arthrosis |
| Staging | Smillie I–V (subchondral fracture → end-stage arthritis) |
| Investigations | X-ray (flattening of MT head); MRI (early disease) |
| Conservative Rx | Activity mod, orthotics, metatarsal bar, NSAIDs |
| Surgical Rx | Débridement (early); Dorsal closing-wedge osteotomy (moderate–severe); Arthroplasty (salvage) |
Fabella Orthopedics what's it etiology pathology signs symptoms and investigations treatment explain everything with appropriate illustrative diagrams for 10 marks
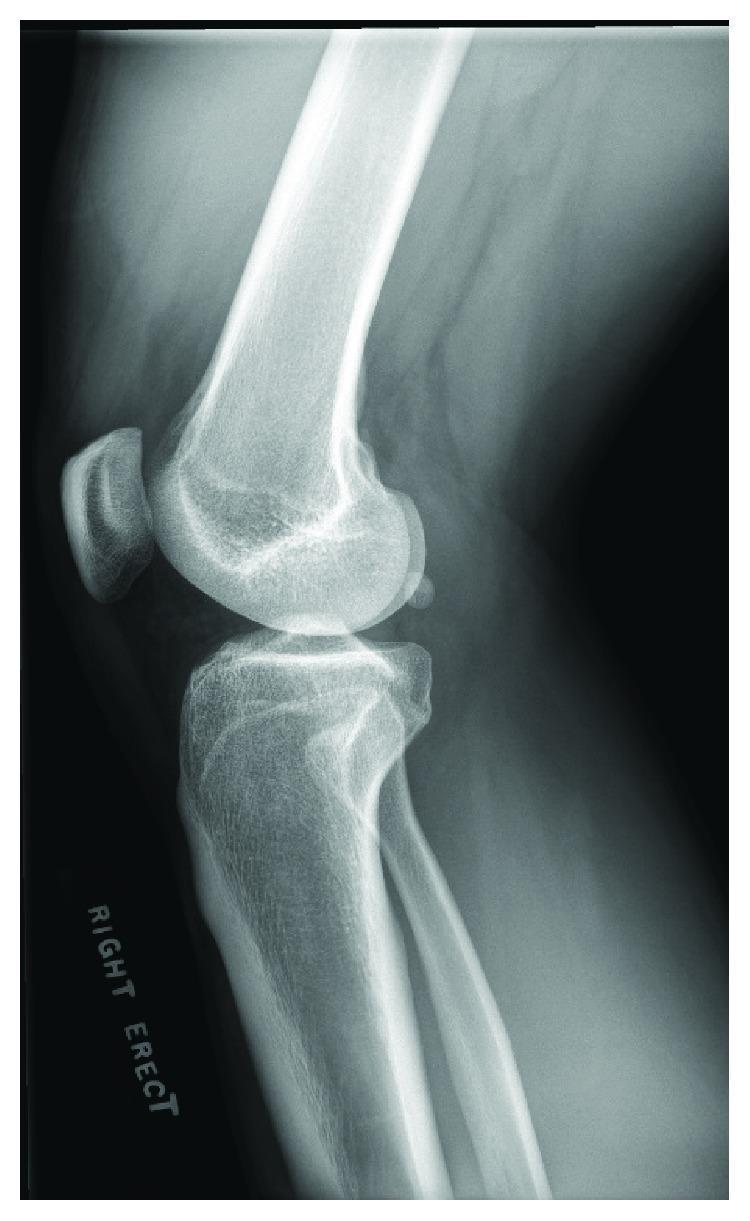
fabella sesamoid bone knee anatomy X-ray
fabella orthopedics syndrome etiology pathology signs symptoms treatment 2024
fabella syndrome etiology pathology signs symptoms investigations treatment
fabella syndrome posterolateral knee pain MRI peroneal nerve compression
fabella syndrome knee pain treatment
Fabella Syndrome — Orthopedics (10 Marks)
1. Definition & Anatomy
"The fabella, present in some patients, is a sesamoid bone located in the lateral head of the gastrocnemius muscle and should not be mistaken for an intra-articular loose body or fracture fragment." — Rosen's Emergency Medicine, 9th Ed.
Key Anatomical Facts
| Feature | Detail |
|---|---|
| Location | Posterior to lateral femoral condyle, within lateral gastrocnemius tendon |
| Prevalence | Approximately 10–30% of the population (varies by ethnicity; higher in Asians) |
| Composition | Ossified (true bone) or fibrocartilaginous |
| Associated structures | Common peroneal (fibular) nerve runs in close proximity; posterior capsule, arcuate ligament, fabellofibular ligament |
| Normal function | Provides mechanical advantage to lateral gastrocnemius; acts as a pulley during knee flexion |
Anatomy Diagrams
2. Etiology
A. Mechanical Friction / Impingement
- Repetitive friction of the fabella against the posterolateral femoral condyle during knee motion
- Occurs especially with full extension (fabella is compressed against the condyle) and deep flexion
- Worsened by activities with repeated knee loading: running, cycling, squatting, ascending stairs
B. Enlargement of the Fabella
- The fabella can hypertrophy (enlarge) due to osteoarthritis — in the arthritic knee, the fabella grows larger and moves more anteriorly, compressing posterior structures
- Associated with knee osteoarthritis (Prichett 1984: fabella associated with increased OA risk)
C. Post-Total Knee Arthroplasty (TKA)
- A well-recognised cause of post-TKA posterolateral knee pain
- The posterior femoral condyle is resected during TKA, altering the biomechanics and causing the fabella to impinge on the posterior prosthesis
- Fabella syndrome is an important differential in the painful TKA
D. Peroneal Nerve Compression
- When the fabella is enlarged or displaced, it may compress the common peroneal (fibular) nerve posterolaterally
- Can cause neuropraxia → foot drop, paresthesias in the lateral leg and dorsum of foot
E. Fracture of the Fabella
- Rare — acute trauma to the posterolateral knee or repetitive stress can cause fabella fracture
F. Bipartite Fabella
- A congenitally bipartite fabella (divided into two fragments by a fibrocartilaginous interface) may become symptomatic with activity
3. Pathology
Repetitive mechanical friction / impingement
↓
Synovitis of fabella-femoral articulation
↓
Periosteal irritation and bursitis (fabellofemoral bursitis)
↓
Cartilage erosion on posterolateral femoral condyle (articular wear)
↓
Secondary enlargement of fabella (in OA setting)
↓
Progressive worsening: impingement, peroneal nerve compression
4. Signs & Symptoms
Symptoms
| Symptom | Detail |
|---|---|
| Posterolateral knee pain | Sharp, localised pain at the back-outer aspect of the knee — the cardinal symptom |
| Pain on full knee extension | Compression of the fabella against the femoral condyle at terminal extension |
| Pain on deep flexion | Stretch of posterior structures over the fabella |
| Catching / clicking sensation | Fabella subluxating or rubbing during knee motion |
| Pain on stair climbing | Increased posterolateral compressive forces |
| Pain with athletic activity | Running, jumping, cycling |
| Cross-legged sitting | Stretches posterolateral structures |
| Neurological symptoms | Tingling, numbness in the lateral leg/foot (peroneal nerve); in severe cases, foot drop and steppage gait |
Signs
| Sign | Detail |
|---|---|
| Localised posterior tenderness | Tenderness on direct palpation over the posterior lateral femoral condyle (fabella point) |
| Pain on terminal extension | Reproduction of symptoms when the knee is fully extended and slightly varus-stressed |
| Pain on varus stress | Varus loading compresses the lateral compartment, pressing the fabella |
| Pain on active/passive tibial internal rotation | Rotational forces irritate the fabella-condyle interface |
| Palpable fabella | A bony nodule may be palpable posterolaterally |
| Reduced range of motion | Especially terminal extension due to pain |
| Antalgic gait | Patient avoids full extension while walking |
| Peroneal nerve signs | Weakness of foot dorsiflexion/eversion, decreased sensation in lateral leg (if peroneal nerve compressed) |
| Foot drop / steppage gait | In severe peroneal nerve compression |
5. Investigations
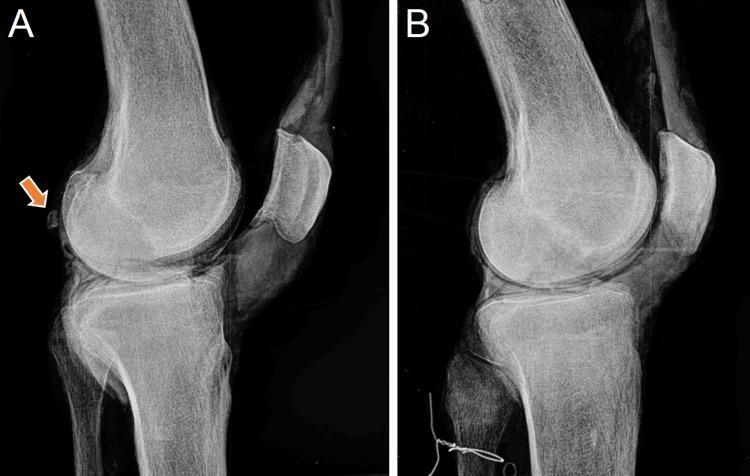
A. Plain Radiography (First-line)
- Lateral and AP views of the knee
- Fabella visible as an ovoid, well-corticated ossific body in the posterolateral knee on lateral view
- May show: increased size, osteoarthritic changes in the fabella, proximity to the posterior femoral condyle, fracture line (bipartite vs. fracture — bipartite has smooth sclerotic margins)

B. MRI (Investigation of Choice for Soft-Tissue Assessment)
- Demonstrates the fabella and its relationship to surrounding structures
- Shows bone marrow oedema within the fabella (stress response)
- Periarticular soft-tissue oedema, bursitis, or effusion
- Cartilage loss on the posterior femoral condyle
- Common peroneal nerve — oedema / thickening suggests neuropathy
- Rules out other causes of posterolateral knee pain (lateral meniscus tear, PCL injury, popliteus tendinopathy)

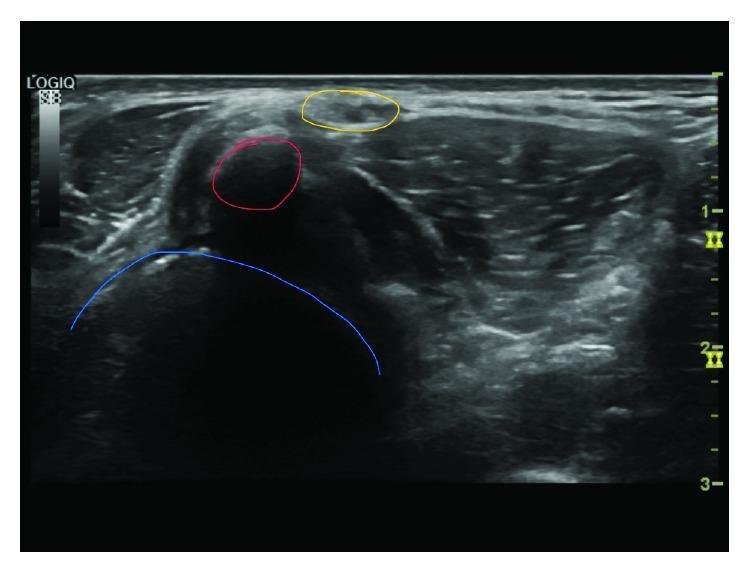
C. Ultrasound
- Dynamic assessment of the fabella during knee motion
- Identifies fabellofemoral bursitis (fluid around the fabella)
- Visualises the common peroneal nerve in relation to the fabella
- Guides diagnostic / therapeutic injections
D. CT Scan
- Delineates the bony anatomy of the fabella
- Useful pre-operatively to assess size, position, and relationship to the prosthesis (in post-TKA cases)
- Distinguishes bipartite fabella from acute fracture
E. Nerve Conduction Studies (NCS) / Electromyography (EMG)
- Indicated when peroneal nerve compression is suspected
- Demonstrates reduced conduction velocity or denervation changes in the peroneal nerve territory
- Helps quantify the degree of neuropathy
F. Diagnostic Local Anaesthetic Injection
- A critically important diagnostic test
- Injection of local anaesthetic (± corticosteroid) directly around the fabella
- Relief of posterolateral knee pain confirms the diagnosis
- Also serves as first-line therapeutic intervention
G. Laboratory Tests
- Not diagnostic but used to exclude differentials:
- Infection (WBC, CRP, ESR)
- Gout / pseudogout (serum uric acid, synovial fluid crystals)
- Rheumatoid arthritis (RF, anti-CCP)
Differential Diagnosis of Posterolateral Knee Pain
| Condition | Distinguishing Feature |
|---|---|
| Lateral meniscus tear | McMurray / Thessaly test positive; meniscal signal on MRI |
| Popliteus tendinopathy | Pain with downhill walking; MRI shows tendon changes |
| PCL injury | Posterior drawer positive |
| Lateral collateral ligament injury | Varus stress test positive |
| Common peroneal nerve entrapment (other) | No fabella on imaging |
| Popliteal cyst | Posterior midline swelling, ultrasound confirms |
| Biceps femoris tendinopathy | Tenderness along biceps tendon |
6. Treatment
A. Conservative (Non-operative) — First-line
| Modality | Details |
|---|---|
| Activity modification | Avoid provocative activities (running, deep squatting, stair climbing) |
| RICE | Rest, Ice, Compression, Elevation — acute phase |
| NSAIDs / Analgesics | Reduce inflammation and pain |
| Physiotherapy | Gastrocnemius stretching; hamstring strengthening; patellar/patellofemoral mobilisation; manual therapy |
| Splinting / casting | Short-term immobilisation for severe acute pain |
| Local corticosteroid injection | First-line intervention — injection of corticosteroid ± local anaesthetic around the fabella; relieves bursitis/synovitis; both diagnostic and therapeutic |
| Orthotics / Knee bracing | Reduce varus stress on the lateral compartment |
"Fabella pain syndrome should initially be managed conservatively… Injecting local anaesthetics or steroids near the site should be performed as a first intervention." — Physiopedia / Driessen et al., 2014
B. Surgical Treatment — For failed conservative management
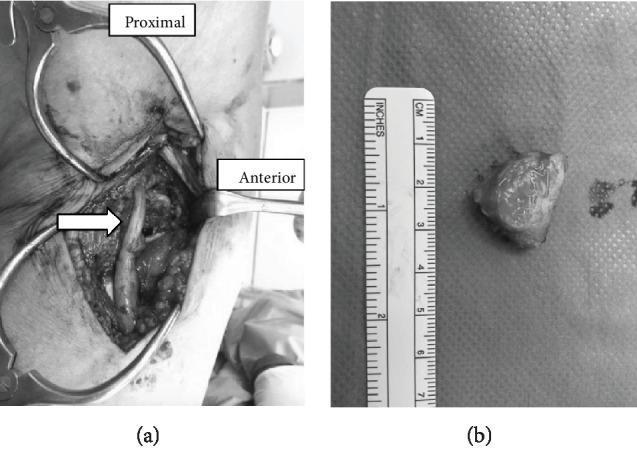
1. Fabellectomy (Excision of the Fabella) — Definitive Treatment
- Failure of conservative management (typically >3–6 months)
- Recurrent posterolateral knee pain
- Progressive peroneal nerve compression
- Post-TKA fabella syndrome
- Open fabellectomy — posterolateral approach; the fabella is excised with reconstruction of the posterolateral corner
- Arthroscopic fabellectomy — minimally invasive; allows simultaneous inspection and treatment of intra-articular pathology (meniscal tears, synovitis)
"Consistent posterolateral pain during exercise might indicate the presence of a fabella syndrome. Resecting the fabella can be indicated and is a minor surgical procedure with minimal risk." — Driessen et al. (PMID: 24666711)
2. Posterolateral Corner Reconstruction
- If fabellectomy destabilises the posterolateral corner (fabellofibular ligament, arcuate ligament attachments), reconstruction may be required
- More relevant in cases where the fabella contributes significantly to lateral stabilisation
3. Management of Peroneal Nerve Compression
- Urgent fabellectomy if progressive foot drop
- Nerve decompression / neurolysis if intraneural fibrosis has developed
7. Summary Table
| Aspect | Key Point |
|---|---|
| Definition | Symptomatic sesamoid in lateral gastrocnemius causing posterolateral knee pain |
| Prevalence | ~10–30% of population have a fabella; most are asymptomatic |
| Etiology | Friction against lateral femoral condyle; OA enlargement; post-TKA; peroneal nerve compression; fracture |
| Pathology | Synovitis → bursitis → cartilage wear → osteophytes; peroneal neuropraxia |
| Key symptom | Posterolateral knee pain worse on full extension; clicking/catching |
| Key sign | Posterior lateral condyle tenderness; pain on varus stress + terminal extension |
| Investigations | X-ray (visualise fabella); MRI (soft tissue); Ultrasound (dynamic + guided injection); NCS/EMG (nerve); Diagnostic LA injection (confirmatory) |
| Conservative Rx | Activity mod, NSAIDs, physio, corticosteroid injection |
| Surgical Rx | Fabellectomy (open or arthroscopic) — definitive |
| Prognosis | Generally good with fabellectomy; minor procedure, low risk |