L carnitine
Reading File
Finding Sources
Searching the Web
L-carnitine pharmacology clinical uses mechanism of action 2025
Searching PubMed
L-carnitine supplementation clinical outcomes
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of L-carnitine:
L-Carnitine
Structure & Chemistry
L-carnitine (β-hydroxy-γ-N-trimethylaminobutyric acid) is a quaternary ammonium compound derived from the amino acids lysine and methionine. It exists as two isoforms — L-carnitine and D-carnitine — but only L-carnitine is biologically active in animals. Acetyl-L-carnitine (ALCAR) is an acetylated form with higher bioavailability and distinct neurological roles.
Biosynthesis & Sources
- Endogenous synthesis: Primarily in the liver and kidneys (skeletal/cardiac muscle cannot synthesize it and depend entirely on uptake)
- Dietary sources: Meat, fish, and dairy products (red meat is the richest source)
- ~97% of total body carnitine is stored in skeletal muscle
- Homeostasis is maintained by endogenous synthesis + dietary absorption + renal reabsorption
Core Biochemical Role: The Carnitine Shuttle
The central function of L-carnitine is transporting long-chain fatty acids (LCFA) across the inner mitochondrial membrane for β-oxidation, since CoA-bound fatty acids cannot cross on their own.
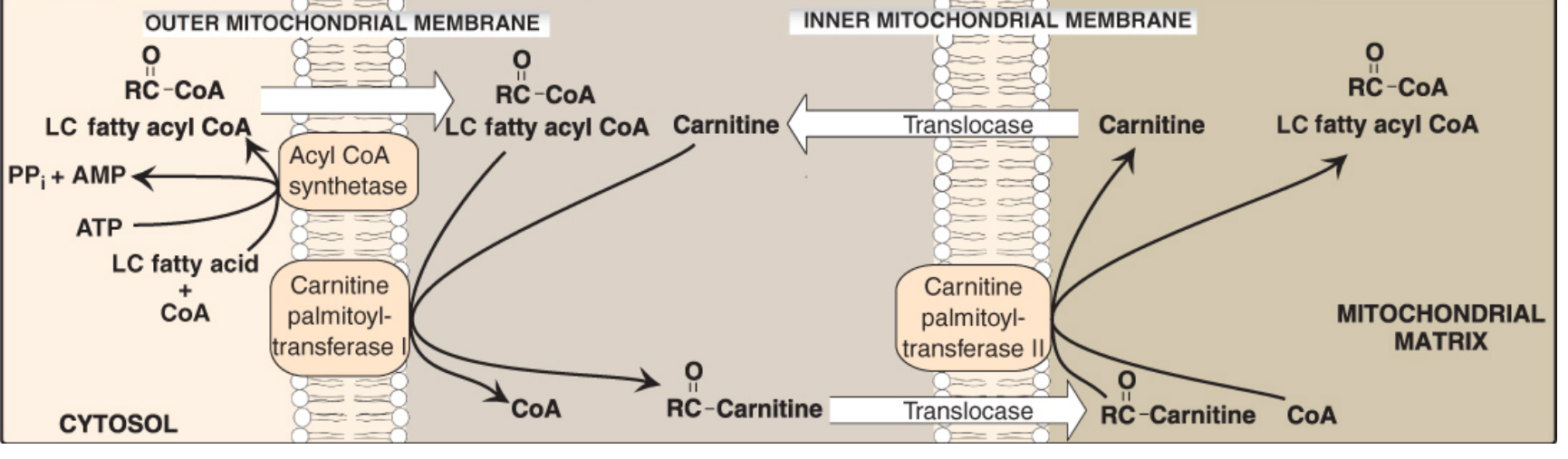
Figure 16.16 — The carnitine shuttle. LC fatty acyl CoA is transferred from the cytosol into the mitochondrial matrix via CPT-I, the acylcarnitine translocase, and CPT-II. (Lippincott's Biochemistry, 8th ed.)
Steps:
- In the cytosol, LCFA is activated to acyl-CoA by acyl-CoA synthetase (outer mitochondrial membrane)
- CPT-I (carnitine palmitoyltransferase I) transfers the acyl group from CoA to carnitine → acylcarnitine (outer membrane)
- Acylcarnitine translocase transports acylcarnitine into the matrix in exchange for free carnitine
- CPT-II (inner membrane) transfers the acyl group back to CoA → regenerates free carnitine and delivers acyl-CoA to the matrix for β-oxidation
Key regulation: Malonyl-CoA (the first intermediate in fatty acid synthesis) inhibits CPT-I, thereby preventing futile cycling — when fat is being made, it cannot simultaneously be degraded.
Carnitine Transporters
- OCTN2 (organic cation transporter novel 2): high-affinity transporter in heart, skeletal muscle, and kidney
- Liver uses a lower-affinity, higher-capacity transporter
Deficiency States
Primary Carnitine Deficiency
- Cause: Autosomal recessive defect in OCTN2 → failure of cellular uptake → urinary wasting of carnitine
- Features: Cardiomyopathy, skeletal muscle weakness, hypoglycemia (inability to oxidize LCFA for energy)
- Treatment: Oral L-carnitine supplementation
Secondary Carnitine Deficiency
| Cause | Mechanism |
|---|---|
| Chronic renal failure / hemodialysis | Loss by dialysis + impaired synthesis |
| Fanconi syndrome | Impaired tubular reabsorption |
| Liver disease (especially alcohol-induced) | Altered synthesis; alcohol-induced cirrhosis may actually raise plasma carnitine due to muscle turnover |
| Valproic acid use | Decreased renal reabsorption |
| Chronic parenteral nutrition | Lack of dietary carnitine → elevated liver enzymes early sign |
| CPT-I deficiency | Cannot transfer acyl group to carnitine; severe hypoglycemia during fasting |
| CPT-II deficiency | Most common form: exercise-induced muscle weakness + myoglobinuria |
(Yamada's Gastroenterology, 7th ed.; Lippincott's Biochemistry, 8th ed.)
Clinical Applications
Approved Indications
- Carnitine deficiency (primary and secondary)
- End-stage renal disease / hemodialysis — L-carnitine is specifically recommended for dialysis-related carnitine deficiency
- Inborn errors of metabolism involving the carnitine cycle
Investigational / Supplemental Uses
- Coronary artery disease: A 2026 systematic review (PMID 41709059) suggests therapeutic potential in reducing angina, improving lipid profiles, and reducing oxidative stress in CAD
- Hemodialysis lipid profile: A 2024 meta-analysis (PMID 39687901) examined effects on lipid profiles in hemodialysis patients
- Female infertility: Reviewed in a 2024 umbrella review of nutrient supplements (PMID 39796491)
- Exercise performance: Reduces post-exercise oxidative stress and inflammation; improves energy metabolism
- Weight loss: Evidence is weak and inconsistent
- Neuroprotection (ALCAR): Acetyl-L-carnitine studied in Parkinson's disease, peripheral neuropathy, and cognitive decline
Dosing
| Indication | Typical Dose |
|---|---|
| Primary deficiency | 50–100 mg/kg/day (oral) |
| Hemodialysis | 20 mg/kg IV after each dialysis session, or 1–3 g/day oral |
| General supplementation | 1–3 g/day |
Safety
- Generally well-tolerated
- High doses may cause fishy body odor (due to trimethylamine production by gut bacteria), nausea, diarrhea
- D-carnitine (as found in some supplements) competitively inhibits L-carnitine and can worsen carnitine deficiency — avoid
- Caution in seizure patients (may lower seizure threshold at very high doses)
Summary: L-carnitine is an essential cofactor for mitochondrial fatty acid β-oxidation via the carnitine shuttle. It is indispensable in tissues that rely on fat oxidation (heart, skeletal muscle) but cannot synthesize it. Its supplementation is evidence-based in primary/secondary deficiency states, particularly dialysis patients, and has emerging evidence in cardiovascular disease and metabolic conditions.
This is a shared conversation. Sign in to Orris to start your own chat.