cytokines in health and diseases
cytokines immune regulation disease
cytokines in health and disease overview 2024 2025
Cytokines in Health and Disease
What Are Cytokines?
Classification of Cytokines
| Classification Basis | Examples |
|---|---|
| Numeric (order of discovery) | IL-1 through IL-41 |
| Functional activity | TNF-alpha, G-CSF |
| Kinetic/inflammatory role | Early/late, pro- vs anti-inflammatory |
| Cell of origin | Monokines (monocyte-derived), lymphokines (lymphocyte-derived) |
| Structural superfamily | IL-1 family, TNF family, IL-6 family, common-gamma-chain family |
- TNF/TNFR superfamily: TNF, lymphotoxins, CD40L (B/T cell activation), FasL (apoptosis)
- IL-1/IL-1R superfamily: IL-1α, IL-1β, IL-18, IL-33, IL-36; plus IL-1RA (receptor antagonist) and Toll-like receptors (TLRs) - pattern recognition molecules for microbial products
- Common gamma-chain family: IL-2, IL-4, IL-7, IL-9, IL-15, IL-21 - all share the γc receptor subunit
- IL-6/gp130 family: IL-6, IL-11, IL-27, oncostatin M - share the gp130 signaling chain
Cytokine Receptors
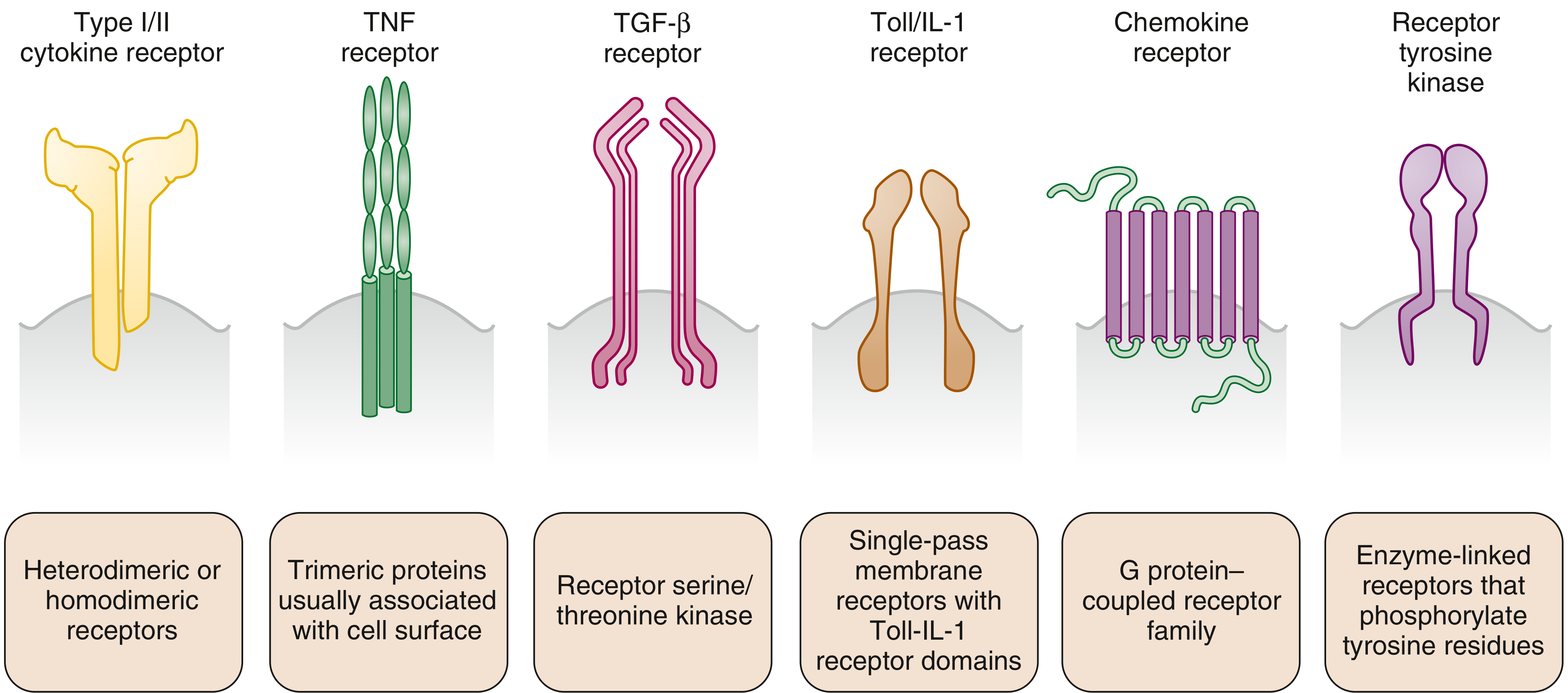
| Receptor Family | Structure | Signaling | Examples |
|---|---|---|---|
| Type I/II cytokine receptors | Heterodimeric/homodimeric | JAK-STAT | IL-2R, IL-4R, IL-6R |
| TNF receptors | Trimeric, cell-surface associated | Death domain, NF-kB | TNFR1, TNFR2, FasR |
| TGF-beta receptors | Dimers | Serine/threonine kinase | TGFβR1/2 |
| Toll/IL-1 receptors | Single-pass membrane | NF-kB, MAPK | IL-1R, TLR4 |
| Chemokine receptors | 7-transmembrane | G protein-coupled | CXCR4, CCR5 |
| Receptor tyrosine kinases | Enzyme-linked dimers | Phosphorylation of tyrosine | EGFR, FGFR |
Cytokine Signaling
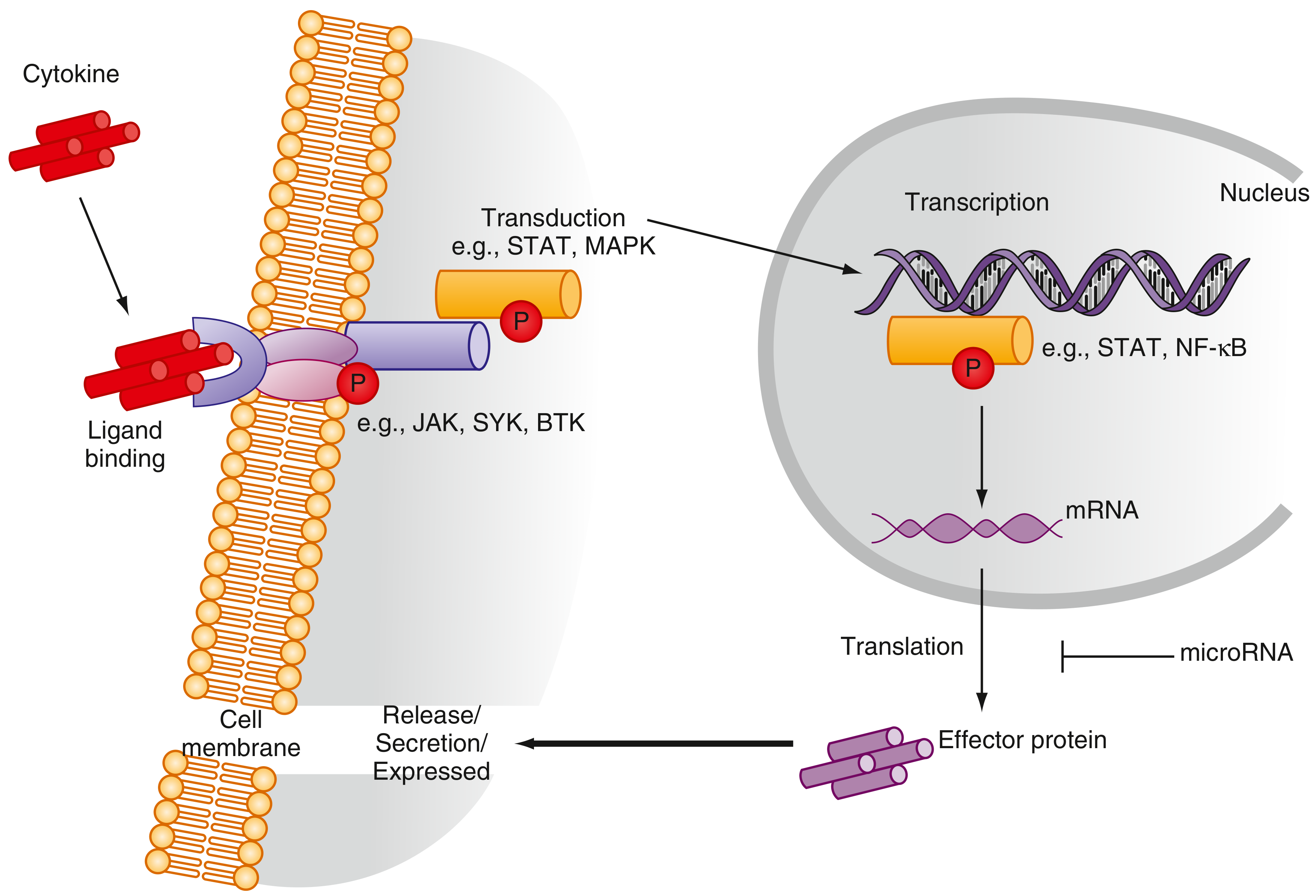
- Cytokine binds receptor, inducing dimerization
- Receptor-associated JAK (Janus kinase) is activated and auto-phosphorylates
- JAK phosphorylates STAT (Signal Transducer and Activator of Transcription) proteins
- Phosphorylated STATs dimerize and translocate to the nucleus to drive gene transcription
- mRNA is translated to effector proteins, which are secreted or expressed on the cell membrane
- microRNAs provide post-transcriptional regulation, dampening the response
Cytokines in Health
1. Innate Immune Defense
- IL-1, IL-6, TNF-alpha: Fever, acute phase response, neutrophil and monocyte recruitment
- IL-12, IL-18: Drive NK cell and later Th1 CD4+ T cell responses
- Type I interferons (IFN-alpha/beta): Antiviral; induce an antiviral state in neighboring cells, activate NK cells, upregulate MHC class I
"Viral infection can induce the release of cytokines (e.g., TNF, IL-1) and type 1 and 3 interferon from infected cells, macrophages, and especially plasmacytoid DCs." - Medical Microbiology 9e
2. Adaptive Immunity
- IL-2: T cell proliferation and survival (the quintessential T cell growth factor)
- IL-4, IL-13: B cell class switching to IgE; Th2 polarization
- IFN-gamma: Activates macrophages for killing intracellular pathogens; Th1 polarization; upregulates MHC II
- IL-10: Anti-inflammatory; suppresses pro-inflammatory cytokine production; produced by regulatory T cells (Tregs) and Th2 cells
- TGF-beta: Suppresses immune activation; promotes Treg differentiation; tissue repair
3. Hematopoiesis
- G-CSF: Neutrophil production (clinical use: post-chemotherapy neutropenia)
- GM-CSF: Granulocyte and macrophage production
- IL-3: Multi-lineage progenitor growth
- IL-5: Eosinophil production and activation; anti-IL-5 (mepolizumab) reduces eosinophils in severe asthma
4. Tissue Repair
- TGF-beta, PDGF: Fibroblast activation, wound healing
- VEGF: Angiogenesis
- IL-10: Limits excessive inflammation to prevent tissue damage
Cytokines in Disease
Rheumatoid Arthritis (RA)
- TNF-alpha and IL-1beta: Drive synoviocyte proliferation, cartilage destruction (matrix metalloproteinases), osteoclast activation (bone erosion)
- IL-6: Drives acute phase response (CRP, SAA, fibrinogen); serum levels correlate with disease activity in RA, juvenile arthritis, ankylosing spondylitis, and polymyalgia rheumatica; more sensitive than ESR for detecting activity in giant cell arteritis
- IL-17: Tissue inflammation, neutrophil recruitment
- IL-15: Promotes T cell activation; downregulated by methotrexate
Psoriasis and Psoriatic Arthritis (PsA)
- Psoriatic plaques and synovium show elevated IL-17A, IL-17F, IL-22, and TNF-alpha
- IL-23 drives Th17 differentiation; IL-17 promotes keratinocyte proliferation and neutrophil recruitment
- Genetic polymorphisms in IL-12 and IL-23 are associated with susceptibility to psoriasis and PsA
- Blocking the shared IL-12/IL-23 p40 subunit (ustekinumab) improves both skin and joint disease; blocking p19 (IL-23 only, e.g., guselkumab) achieves near-complete skin clearance
Allergic Disease and Asthma
- IL-4: Drives B cell class switching to IgE; upregulates VCAM-1 for eosinophil recruitment
- IL-5: Eosinophil production; anti-IL-5 (mepolizumab) reduces asthma exacerbations
- IL-13: Airway hyperresponsiveness, mucus production
- IL-9: Mast cell proliferation
- Mast cells, when activated, release TNF, IL-1, IL-4, IL-5, IL-6, IL-9, IL-13, CCL3, and CCL4 - fueling the allergic late-phase reaction
Sepsis and Cytokine Storm
- TNF, IL-1, IL-6, IL-8, IL-12, IFN-gamma - rapid systemic release causes fever, vasodilation, capillary leak, coagulopathy
- Can progress to septic shock, multi-organ failure
- Superantigen-mediated cytokine storm (e.g., Staphylococcal toxic shock syndrome toxin): activates 20-30% of all T cells simultaneously, generating enormous TNF and IL-2 release
- Viral cytokine storm: Seen in highly virulent influenza (H5N1, H1N1), dengue haemorrhagic fever, and COVID-19 - characterised by elevated IL-6, IL-1beta, IL-18, TNF, IFN-gamma
Cancer
- IFN-alpha: Anti-tumor (used in hairy cell leukemia, melanoma)
- IL-2: T cell expansion; high-dose IL-2 used in metastatic melanoma and renal carcinoma
- TNF: Can induce tumor cell apoptosis but chronic low-level TNF promotes NF-kB-driven tumor survival and angiogenesis
- IL-6: Promotes survival of myeloma cells; tocilizumab is used for cytokine release syndrome (CRS) post-CAR-T therapy
- TGF-beta: Profoundly immunosuppressive in the tumor microenvironment; inhibits T cell killing
Inflammatory Bowel Disease (IBD)
- TNF-alpha: Central in both Crohn's disease and ulcerative colitis; anti-TNF agents (infliximab, adalimumab) are mainstay therapy
- IL-23/IL-17 axis: Genetic studies show IL-23R variants associate with Crohn's disease
- IL-10: Deficiency leads to spontaneous colitis in mouse models; mutations cause early-onset IBD in infants
Neurological Disease
- IL-6, TNF, IL-1beta: Elevated in CSF and serum during neuroinflammatory conditions (MS, encephalitis)
- Type I interferons: Central to MS pathogenesis and also to treatment (IFN-beta reduces relapse rate in relapsing-remitting MS)
Cytokine Measurement in Clinical Practice
- ELISA and multiplex assays (measure 25-360 cytokines in ~20 µL sample simultaneously)
- Quantitative PCR / TaqMan arrays at the mRNA level
- Single-cell sequencing to identify cytokine sources in complex tissue biopsies
Cytokine-Targeted Therapeutics
| Target | Drug Class | Examples | Disease |
|---|---|---|---|
| TNF-alpha | Anti-TNF mAb / fusion protein | Infliximab, adalimumab, etanercept | RA, PsA, IBD, AS |
| IL-1 | IL-1RA, anti-IL-1beta | Anakinra, canakinumab | RA, Still's disease, gout |
| IL-6/IL-6R | Anti-IL-6R mAb | Tocilizumab, sarilumab | RA, GCA, CRS after CAR-T |
| IL-12/IL-23 (p40) | Anti-p40 mAb | Ustekinumab | Psoriasis, PsA, Crohn's |
| IL-23 (p19) | Anti-p19 mAb | Guselkumab, risankizumab | Psoriasis, PsA |
| IL-17A | Anti-IL-17A mAb | Secukinumab, ixekizumab | Psoriasis, AS |
| IL-5 | Anti-IL-5 mAb | Mepolizumab, reslizumab | Severe eosinophilic asthma |
| IL-4R/IL-13 | Anti-IL-4Ra | Dupilumab | Atopic dermatitis, asthma |
| JAK1/2/3 (intracellular) | JAK inhibitors | Tofacitinib, baricitinib | RA, PsA, IBD |
Summary Table of Key Cytokines
| Cytokine | Main Source | Main Function | Disease Relevance |
|---|---|---|---|
| IL-1beta | Macrophages, DCs | Fever, acute phase, inflammasome | RA, gout, autoinflammatory syndromes |
| IL-2 | T cells | T cell proliferation/survival | Cancer immunotherapy (high-dose), SCID (deficiency) |
| IL-4 | Th2 cells, mast cells | IgE class switching, Th2 polarization | Allergy, asthma, atopic dermatitis |
| IL-5 | Th2, ILC2 | Eosinophil production | Asthma, eosinophilic esophagitis |
| IL-6 | Macrophages, T cells, synoviocytes | Acute phase, B cell differentiation | RA, sepsis, CRS, plasma cell myeloma |
| IL-10 | Tregs, Th2, macrophages | Anti-inflammatory, suppresses pro-inflammatory cytokines | IBD (deficiency), immune regulation |
| IL-12 | DCs, macrophages | Th1 polarization, IFN-gamma induction | Psoriasis (IL-12/23 axis), mycobacterial defense |
| IL-17A | Th17 cells, CD8+ T cells | Neutrophil recruitment, barrier defense | Psoriasis, PsA, AS |
| IL-23 | DCs, macrophages | Th17 maintenance | Psoriasis, PsA, Crohn's |
| TNF-alpha | Macrophages, T cells | Inflammation, apoptosis, NF-kB | RA, IBD, sepsis, cachexia |
| IFN-gamma | Th1, NK, CD8+ T cells | Macrophage activation, MHC II upregulation | Infection, granuloma formation, HLH |
| IFN-alpha/beta | Plasmacytoid DCs, virally-infected cells | Antiviral state | Viral infections, SLE (type I IFN signature) |
| TGF-beta | Tregs, fibroblasts | Immune suppression, fibrosis | Fibrotic diseases, tumor immune evasion |
- Firestein & Kelley's Textbook of Rheumatology - Classification, receptors, signaling, regulation, RA, PsA
- Cellular and Molecular Immunology - Allergic disease, mast cells, eosinophils
- Medical Microbiology 9e - Cytokine storm, antiviral responses
- Goodman & Gilman's The Pharmacological Basis of Therapeutics - Innate/adaptive immunity overview
- Henry's Clinical Diagnosis and Management by Laboratory Methods - Cytokine measurement
Generate a clinical decision flowchart for when to use different anti-cytokine therapies
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace dir"
mkdir -p /home/daytona/workspace/anti-cytokine-flowchart
~/anti-cytokine-flowchart/build.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_WIDE"; // 13.3" × 7.5"
pres.title = "Clinical Decision Flowchart: Anti-Cytokine Therapies";
pres.author = "Orris Medical AI";
// ─── Colour Palette ───────────────────────────────────────────────
const C = {
navy: "0D1F3C",
teal: "0B7285",
tealLt: "1A9BAF",
amber: "E67700",
green: "2E7D32",
purple: "6A1E8F",
red: "B71C1C",
orange: "E65100",
steel: "37474F",
white: "FFFFFF",
offWhite:"F4F6F9",
ltGray: "E8ECF0",
midGray: "9EA9B0",
gold: "F59F00",
lime: "558B2F",
};
// ─── Helpers ──────────────────────────────────────────────────────
function box(slide, opts) {
const {
x, y, w, h,
fill = C.white, line = C.steel, lineW = 1.5,
text, fontSize = 11, bold = false, color = C.steel,
align = "center", valign = "middle",
radius, textArr,
} = opts;
slide.addShape(pres.ShapeType.roundRect, {
x, y, w, h,
fill: { color: fill },
line: { color: line, width: lineW },
rectRadius: radius !== undefined ? radius : 0.12,
});
if (textArr) {
slide.addText(textArr, { x, y, w, h, align, valign, fontSize, color, margin: 4 });
} else if (text) {
slide.addText(text, { x, y, w, h, align, valign, fontSize, bold, color, margin: 4 });
}
}
function diamond(slide, opts) {
const { x, y, w, h, fill, line = C.steel, text, fontSize = 10, color = C.white, bold = true } = opts;
slide.addShape(pres.ShapeType.diamond, {
x, y, w, h,
fill: { color: fill },
line: { color: line, width: 1.5 },
});
slide.addText(text, { x, y, w, h, align: "center", valign: "middle", fontSize, bold, color, margin: 4 });
}
function arrow(slide, x1, y1, x2, y2, color = C.steel) {
slide.addShape(pres.ShapeType.line, {
x: x1, y: y1, w: x2 - x1, h: y2 - y1,
line: { color, width: 1.5, endArrowType: "triangle" },
});
}
function label(slide, x, y, text, fontSize = 8.5, color = C.amber, bold = true) {
slide.addText(text, { x, y, w: 0.7, h: 0.22, fontSize, bold, color, align: "center" });
}
function sectionHeader(slide, x, y, w, text, fill, textColor = C.white) {
slide.addShape(pres.ShapeType.roundRect, {
x, y, w, h: 0.38,
fill: { color: fill },
line: { color: fill },
rectRadius: 0.1,
});
slide.addText(text, { x, y, w, h: 0.38, align: "center", valign: "middle", fontSize: 10, bold: true, color: textColor, margin: 0 });
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 1 — Title / Overview
// ═══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
// Dark background
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 13.3, h: 7.5, fill: { color: C.navy }, line: { color: C.navy } });
// Accent bar
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.18, h: 7.5, fill: { color: C.tealLt }, line: { color: C.tealLt } });
// Title
s.addText("Clinical Decision Flowchart", {
x: 0.5, y: 1.4, w: 12.3, h: 0.85,
fontSize: 36, bold: true, color: C.white, align: "center",
});
s.addText("Anti-Cytokine Therapy Selection by Disease", {
x: 0.5, y: 2.3, w: 12.3, h: 0.55,
fontSize: 22, bold: false, color: C.tealLt, align: "center",
});
s.addText("For Medical Students & Trainees", {
x: 0.5, y: 2.9, w: 12.3, h: 0.35,
fontSize: 14, bold: false, color: C.midGray, align: "center",
});
// Disease area pills
const pills = [
{ label: "Rheumatic Diseases", fill: C.teal },
{ label: "GI / IBD", fill: C.green },
{ label: "Respiratory / Allergy", fill: C.purple },
{ label: "Oncology / CRS", fill: C.red },
{ label: "Emergency / Sepsis", fill: C.orange },
];
const pillW = 2.2, gap = 0.2;
const totalW = pills.length * pillW + (pills.length - 1) * gap;
let px = (13.3 - totalW) / 2;
pills.forEach(p => {
s.addShape(pres.ShapeType.roundRect, { x: px, y: 3.65, w: pillW, h: 0.38, fill: { color: p.fill }, line: { color: p.fill }, rectRadius: 0.19 });
s.addText(p.label, { x: px, y: 3.65, w: pillW, h: 0.38, align: "center", valign: "middle", fontSize: 9.5, bold: true, color: C.white, margin: 0 });
px += pillW + gap;
});
// Legend
s.addText("How to use this flowchart:", { x: 1.5, y: 4.35, w: 10.3, h: 0.3, fontSize: 11, bold: true, color: C.gold, align: "center" });
s.addText([
{ text: "1. Identify the patient's primary diagnosis ", options: {} },
{ text: "2. Navigate to the relevant slide ", options: {} },
{ text: "3. Follow the decision nodes (diamonds) to select the appropriate biologic or JAK inhibitor", options: {} },
], { x: 1.5, y: 4.65, w: 10.3, h: 0.5, fontSize: 10, color: C.ltGray, align: "center", margin: 0 });
// Note
s.addText("⚠ Always individualise therapy. Check contraindications, TB screening, and local formulary before prescribing.", {
x: 1.0, y: 5.45, w: 11.3, h: 0.45,
fontSize: 9.5, italic: true, color: C.midGray, align: "center",
});
// Footer
s.addText("Sources: Firestein & Kelley's Rheumatology | Goodman & Gilman's Pharmacology | Cellular & Molecular Immunology", {
x: 0.4, y: 7.1, w: 12.5, h: 0.25, fontSize: 7.5, color: C.midGray, align: "center",
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 2 — Rheumatic Diseases
// ═══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 13.3, h: 7.5, fill: { color: C.offWhite }, line: { color: C.offWhite } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 13.3, h: 0.52, fill: { color: C.navy }, line: { color: C.navy } });
s.addText("RHEUMATIC DISEASES — Anti-Cytokine Therapy Flowchart", {
x: 0.2, y: 0, w: 12.9, h: 0.52, fontSize: 13, bold: true, color: C.white, valign: "middle",
});
// ── START BOX ──
box(s, { x: 5.4, y: 0.7, w: 2.5, h: 0.45, fill: C.navy, line: C.navy, text: "Inflammatory Arthritis / Connective Tissue Disease", fontSize: 8.5, color: C.white, bold: true });
arrow(s, 6.65, 1.15, 6.65, 1.42);
// ── Q1: Diagnosis ──
diamond(s, { x: 5.2, y: 1.42, w: 2.9, h: 0.7, fill: C.teal, text: "Primary Diagnosis?", fontSize: 10 });
// ─ Branch arrows from diamond center (6.65, 1.77)
// Left → RA
arrow(s, 5.2, 1.77, 2.55, 1.77);
label(s, 4.0, 1.6, "RA / JIA");
// Right → SpA/PsA
arrow(s, 8.1, 1.77, 10.25, 1.77);
label(s, 8.9, 1.6, "PsA / AS");
// Down → SLE / other
arrow(s, 6.65, 2.12, 6.65, 2.38);
label(s, 6.75, 2.15, "SLE / PMR / GCA");
// ─── RA branch ───
diamond(s, { x: 0.7, y: 1.42, w: 2.5, h: 0.7, fill: C.tealLt, text: "Adequate response to MTX / csDMARD?", fontSize: 9 });
// Yes → continue MTX
arrow(s, 1.95, 1.42, 1.95, 0.95);
label(s, 2.0, 1.05, "YES");
box(s, { x: 0.7, y: 0.55, w: 2.5, h: 0.38, fill: C.lime, line: C.lime, text: "Continue csDMARD (MTX) + monitor", fontSize: 8, color: C.white });
// No → next q
arrow(s, 1.95, 2.12, 1.95, 2.4);
label(s, 2.05, 2.2, "NO");
diamond(s, { x: 0.7, y: 2.4, w: 2.5, h: 0.7, fill: C.tealLt, text: "High disease activity or poor prognosis?", fontSize: 9 });
// → bDMARD
arrow(s, 1.95, 3.1, 1.95, 3.38);
box(s, { x: 0.25, y: 3.38, w: 3.4, h: 1.1, fill: C.white, line: C.teal,
textArr: [
{ text: "Anti-TNF (1st line bDMARD)\n", options: { bold: true, color: C.teal, fontSize: 10, breakLine: false } },
{ text: "Infliximab, Adalimumab,\nEtanercept, Certolizumab\n", options: { color: C.steel, fontSize: 9, breakLine: false } },
{ text: "Baricitinib / Tofacitinib (JAKi)\n", options: { bold: true, color: C.purple, fontSize: 9, breakLine: false } },
{ text: "if anti-TNF fails or contraindicated", options: { color: C.midGray, fontSize: 8 } },
],
align: "left", valign: "top",
});
// IL-6R if anti-TNF fails
arrow(s, 1.95, 4.48, 1.95, 4.75);
box(s, { x: 0.25, y: 4.75, w: 3.4, h: 0.65, fill: C.white, line: C.purple,
textArr: [
{ text: "Anti-TNF failure? → ", options: { bold: true, color: C.steel, fontSize: 9 } },
{ text: "Tocilizumab (anti-IL-6R)\nor Sarilumab / Abatacept / Rituximab", options: { color: C.purple, fontSize: 9 } },
],
align: "left", valign: "middle",
});
// IL-1RA for Still's
arrow(s, 1.95, 5.4, 1.95, 5.65);
box(s, { x: 0.25, y: 5.65, w: 3.4, h: 0.5, fill: C.white, line: C.orange,
textArr: [
{ text: "Still's Disease / Autoinflammatory: ", options: { bold: true, color: C.steel, fontSize: 9 } },
{ text: "Anakinra (IL-1RA) or Canakinumab", options: { color: C.orange, fontSize: 9 } },
],
align: "left", valign: "middle",
});
// ─── PsA / AS branch ───
diamond(s, { x: 9.5, y: 1.42, w: 2.8, h: 0.7, fill: C.tealLt, text: "Prominent skin disease (psoriasis)?", fontSize: 9 });
// YES →
arrow(s, 10.9, 1.42, 10.9, 0.92);
label(s, 10.98, 1.1, "YES");
box(s, { x: 9.5, y: 0.55, w: 2.8, h: 0.35, fill: C.purple, line: C.purple, text: "IL-17A inhibitor: Secukinumab / Ixekizumab", fontSize: 8.5, color: C.white });
// NO → anti-TNF preferred
arrow(s, 12.3, 1.77, 12.6, 1.77);
label(s, 12.35, 1.6, "NO");
box(s, { x: 12.6, y: 1.6, w: 0.65, h: 0.35, fill: C.teal, line: C.teal, text: "Anti-TNF", fontSize: 8, color: C.white });
arrow(s, 10.9, 2.12, 10.9, 2.38);
diamond(s, { x: 9.5, y: 2.38, w: 2.8, h: 0.7, fill: C.tealLt, text: "Predominant axial disease (AS)?", fontSize: 9 });
arrow(s, 10.9, 3.08, 10.9, 3.38);
box(s, { x: 9.5, y: 3.38, w: 2.8, h: 0.95, fill: C.white, line: C.teal,
textArr: [
{ text: "Anti-TNF (1st line):\n", options: { bold: true, color: C.teal, fontSize: 9, breakLine: false } },
{ text: "Adalimumab, Certolizumab,\nEtanercept\n", options: { color: C.steel, fontSize: 8.5, breakLine: false } },
{ text: "OR IL-17A inhibitor (secukinumab)\nif anti-TNF contraindicated", options: { color: C.purple, fontSize: 8.5 } },
],
align: "left", valign: "top",
});
arrow(s, 10.9, 4.33, 10.9, 4.6);
box(s, { x: 9.5, y: 4.6, w: 2.8, h: 0.65, fill: C.white, line: C.purple,
textArr: [
{ text: "Skin + joints (PsA): ", options: { bold: true, color: C.steel, fontSize: 9 } },
{ text: "IL-23 inhibitor\n(Guselkumab, Risankizumab)", options: { color: C.purple, fontSize: 9 } },
],
align: "left", valign: "middle",
});
// ─── SLE / PMR / GCA branch ───
diamond(s, { x: 5.2, y: 2.38, w: 2.9, h: 0.7, fill: C.tealLt, text: "Specific diagnosis?", fontSize: 10 });
// GCA
arrow(s, 7.5, 2.73, 8.5, 3.5);
label(s, 7.8, 2.8, "GCA/PMR");
box(s, { x: 7.8, y: 3.5, w: 2.1, h: 0.55, fill: C.white, line: C.teal, text: "Tocilizumab (IL-6R)\n+ steroids taper", fontSize: 8.5, color: C.steel });
// SLE
arrow(s, 6.65, 3.08, 6.65, 3.38);
label(s, 6.75, 3.15, "SLE");
box(s, { x: 5.2, y: 3.38, w: 2.9, h: 0.8, fill: C.white, line: C.teal,
textArr: [
{ text: "Anifrolumab (anti-IFN-α receptor)\n", options: { bold: true, color: C.teal, fontSize: 9, breakLine: false } },
{ text: "Belimumab (anti-BLyS)\n", options: { color: C.steel, fontSize: 8.5, breakLine: false } },
{ text: "Baricitinib (JAKi – lupus nephritis)", options: { color: C.purple, fontSize: 8.5 } },
],
align: "left", valign: "top",
});
// Key box
s.addShape(pres.ShapeType.roundRect, { x: 3.7, y: 5.6, w: 5.9, h: 1.65, fill: { color: C.ltGray }, line: { color: C.midGray, width: 1 }, rectRadius: 0.1 });
s.addText("📋 Screen before any biologic:", { x: 3.8, y: 5.65, w: 5.7, h: 0.28, fontSize: 9.5, bold: true, color: C.navy });
s.addText([
{ text: "• TB (Quantiferon/TST) • Hepatitis B & C serology • Varicella immunity\n", options: { fontSize: 8.5, color: C.steel, breakLine: false } },
{ text: "• Pregnancy / breastfeeding • Live vaccine history • Renal/hepatic function\n", options: { fontSize: 8.5, color: C.steel, breakLine: false } },
{ text: "• Active infection = HOLD biologic • Heart failure (NYHA III/IV) = avoid anti-TNF", options: { fontSize: 8.5, color: C.red, bold: true } },
], { x: 3.8, y: 5.95, w: 5.7, h: 1.2, margin: 0 });
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 3 — GI / Respiratory / Oncology / Emergency
// ═══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 13.3, h: 7.5, fill: { color: C.offWhite }, line: { color: C.offWhite } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 13.3, h: 0.52, fill: { color: C.navy }, line: { color: C.navy } });
s.addText("GI · RESPIRATORY · ONCOLOGY · EMERGENCY — Anti-Cytokine Therapy Flowchart", {
x: 0.2, y: 0, w: 12.9, h: 0.52, fontSize: 12, bold: true, color: C.white, valign: "middle",
});
// ── Column dividers ──
s.addShape(pres.ShapeType.line, { x: 3.3, y: 0.6, w: 0, h: 6.7, line: { color: C.ltGray, width: 1.5 } });
s.addShape(pres.ShapeType.line, { x: 6.65, y: 0.6, w: 0, h: 6.7, line: { color: C.ltGray, width: 1.5 } });
s.addShape(pres.ShapeType.line, { x: 9.95, y: 0.6, w: 0, h: 6.7, line: { color: C.ltGray, width: 1.5 } });
// Column headers
sectionHeader(s, 0.1, 0.58, 3.1, "🩺 GI / IBD", C.green);
sectionHeader(s, 3.4, 0.58, 3.15, "🫁 Respiratory / Allergy", C.purple);
sectionHeader(s, 6.75, 0.58, 3.1, "🔬 Oncology / CAR-T", C.red);
sectionHeader(s, 10.05, 0.58, 3.15, "🚨 Emergency / Critical Care", C.orange);
// ── GI / IBD ──
diamond(s, { x: 0.3, y: 1.1, w: 2.7, h: 0.65, fill: C.green, text: "IBD Subtype?", fontSize: 10 });
// Crohn's
arrow(s, 1.65, 1.1, 1.65, 0.85);
s.addText("Crohn's", { x: 0.3, y: 0.64, w: 1.1, h: 0.2, fontSize: 8, color: C.amber, bold: true });
box(s, { x: 0.1, y: 0.15, w: 1.5, h: 0.5, fill: C.white, line: C.green,
text: "Anti-TNF\n(Infliximab /\nAdalimumab)", fontSize: 7.5, color: C.steel });
// UC / both
arrow(s, 1.65, 1.75, 1.65, 2.05);
s.addText("UC / Both", { x: 1.8, y: 1.55, w: 0.9, h: 0.2, fontSize: 8, color: C.amber, bold: true });
box(s, { x: 0.1, y: 2.05, w: 3.1, h: 1.0, fill: C.white, line: C.green,
textArr: [
{ text: "Vedolizumab (anti-α4β7 integrin)\n", options: { bold: true, color: C.green, fontSize: 9, breakLine: false } },
{ text: "Ustekinumab (anti-IL-12/23 p40)\n", options: { color: C.steel, fontSize: 8.5, breakLine: false } },
{ text: "Risankizumab (anti-IL-23 p19)\n", options: { color: C.steel, fontSize: 8.5, breakLine: false } },
{ text: "Tofacitinib / Upadacitinib (JAKi – UC)\n", options: { color: C.purple, fontSize: 8.5, breakLine: false } },
{ text: "Anti-TNF: if above fail or severe flare", options: { color: C.midGray, fontSize: 8 } },
],
align: "left", valign: "top",
});
arrow(s, 1.65, 3.05, 1.65, 3.3);
diamond(s, { x: 0.3, y: 3.3, w: 2.7, h: 0.65, fill: C.green, text: "Steroid-dependent?", fontSize: 9.5 });
arrow(s, 1.65, 3.95, 1.65, 4.2);
box(s, { x: 0.1, y: 4.2, w: 3.1, h: 0.55, fill: C.white, line: C.green,
text: "Escalate to biologic + step-up steroid-free maintenance protocol", fontSize: 8.5, color: C.steel });
arrow(s, 1.65, 4.75, 1.65, 5.0);
box(s, { x: 0.1, y: 5.0, w: 3.1, h: 0.7, fill: C.white, line: C.orange,
textArr: [
{ text: "Peri-operative / fistulising Crohn's:\n", options: { bold: true, color: C.orange, fontSize: 9, breakLine: false } },
{ text: "Infliximab (induction) + consider\ncombination therapy with MTX/AZA", options: { color: C.steel, fontSize: 8.5 } },
],
align: "left", valign: "top",
});
// ── Respiratory / Allergy ──
diamond(s, { x: 3.5, y: 1.1, w: 3.0, h: 0.65, fill: C.purple, text: "Respiratory / Allergic Condition?", fontSize: 9 });
// Severe asthma branch
arrow(s, 5.0, 1.75, 5.0, 2.05);
s.addText("Severe asthma", { x: 5.1, y: 1.77, w: 1.3, h: 0.2, fontSize: 8, color: C.amber, bold: true });
diamond(s, { x: 3.5, y: 2.05, w: 3.0, h: 0.65, fill: C.purple, text: "Eosinophilic phenotype\n(eos ≥ 300)?", fontSize: 9 });
arrow(s, 5.0, 2.7, 5.0, 2.98);
s.addText("YES", { x: 5.1, y: 2.75, w: 0.5, h: 0.2, fontSize: 8, color: C.amber, bold: true });
box(s, { x: 3.5, y: 2.98, w: 3.0, h: 0.75, fill: C.white, line: C.purple,
textArr: [
{ text: "Anti-IL-5: Mepolizumab / Reslizumab\n", options: { bold: true, color: C.purple, fontSize: 9, breakLine: false } },
{ text: "Anti-IL-5Rα: Benralizumab\n", options: { color: C.steel, fontSize: 8.5, breakLine: false } },
{ text: "Anti-IL-4Rα: Dupilumab (IL-4 + IL-13)\nif atopic + eosinophilic", options: { color: C.steel, fontSize: 8.5 } },
],
align: "left", valign: "top",
});
arrow(s, 3.5, 2.37, 3.2, 2.37);
s.addText("NO", { x: 3.0, y: 2.2, w: 0.5, h: 0.2, fontSize: 8, color: C.amber, bold: true });
box(s, { x: 3.4, y: 3.85, w: 3.0, h: 0.55, fill: C.white, line: C.purple,
text: "Tezepelumab (anti-TSLP)\nfor uncontrolled severe asthma, any phenotype", fontSize: 8.5, color: C.steel });
arrow(s, 5.0, 3.73, 5.0, 3.85);
// Atopic derm
arrow(s, 5.0, 4.4, 5.0, 4.65);
s.addText("Atopic dermatitis /\nChronic urticaria", { x: 5.1, y: 4.35, w: 1.8, h: 0.28, fontSize: 8, color: C.amber, bold: true });
box(s, { x: 3.5, y: 4.65, w: 3.0, h: 0.65, fill: C.white, line: C.purple,
textArr: [
{ text: "Dupilumab (anti-IL-4Rα, blocks IL-4 + IL-13)\n", options: { bold: true, color: C.purple, fontSize: 9, breakLine: false } },
{ text: "Tralokinumab (anti-IL-13)\n", options: { color: C.steel, fontSize: 8.5, breakLine: false } },
{ text: "Omalizumab (anti-IgE) for urticaria / allergic asthma", options: { color: C.steel, fontSize: 8.5 } },
],
align: "left", valign: "top",
});
// ── Oncology / CAR-T ──
diamond(s, { x: 6.85, y: 1.1, w: 2.95, h: 0.65, fill: C.red, text: "Oncology Indication?", fontSize: 9.5 });
// Cytokine release syndrome (CRS)
arrow(s, 8.32, 1.75, 8.32, 2.05);
s.addText("CAR-T CRS\n/ immune effector\ncell toxicity", { x: 8.4, y: 1.6, w: 1.5, h: 0.45, fontSize: 7.5, color: C.amber, bold: true });
diamond(s, { x: 6.85, y: 2.05, w: 2.95, h: 0.65, fill: C.red, text: "CRS Grade?", fontSize: 10 });
arrow(s, 8.32, 2.7, 8.32, 2.98);
s.addText("Grade ≥2", { x: 8.4, y: 2.72, w: 0.9, h: 0.2, fontSize: 8, color: C.amber, bold: true });
box(s, { x: 6.85, y: 2.98, w: 2.95, h: 0.7, fill: C.white, line: C.red,
textArr: [
{ text: "Tocilizumab (anti-IL-6R) — FIRST LINE\n", options: { bold: true, color: C.red, fontSize: 9, breakLine: false } },
{ text: "± Corticosteroids\n", options: { color: C.steel, fontSize: 8.5, breakLine: false } },
{ text: "Grade 3–4: ICU support; repeat tocilizumab\nor siltuximab if refractory", options: { color: C.orange, fontSize: 8.5 } },
],
align: "left", valign: "top",
});
// Grade 1
arrow(s, 6.85, 2.37, 6.65, 2.37);
s.addText("Grade 1", { x: 6.5, y: 2.18, w: 0.7, h: 0.2, fontSize: 8, color: C.amber, bold: true });
box(s, { x: 6.0, y: 2.25, w: 0.6, h: 0.28, fill: C.lime, line: C.lime, text: "Supportive", fontSize: 7.5, color: C.white });
// Immunotherapy checkpoint
arrow(s, 8.32, 3.68, 8.32, 3.95);
s.addText("Checkpoint\ninhibitor irAEs", { x: 8.4, y: 3.58, w: 1.2, h: 0.35, fontSize: 7.5, color: C.amber, bold: true });
box(s, { x: 6.85, y: 3.95, w: 2.95, h: 0.7, fill: C.white, line: C.red,
textArr: [
{ text: "Steroids (1st line for most irAEs)\n", options: { bold: true, color: C.steel, fontSize: 9, breakLine: false } },
{ text: "Infliximab: colitis grades 3–4\n", options: { color: C.red, fontSize: 8.5, breakLine: false } },
{ text: "Tocilizumab: myocarditis / pneumonitis\nBaricitinib: steroid-refractory", options: { color: C.red, fontSize: 8.5 } },
],
align: "left", valign: "top",
});
// Cancer with IL-2
arrow(s, 8.32, 4.65, 8.32, 4.9);
box(s, { x: 6.85, y: 4.9, w: 2.95, h: 0.65, fill: C.white, line: C.orange,
textArr: [
{ text: "Cancer immunotherapy (adjuvant):\n", options: { bold: true, color: C.orange, fontSize: 9, breakLine: false } },
{ text: "High-dose IL-2 (metastatic melanoma / RCC)\nIFN-α (hairy cell leukaemia)", options: { color: C.steel, fontSize: 8.5 } },
],
align: "left", valign: "top",
});
// ── Emergency / Critical Care ──
diamond(s, { x: 10.15, y: 1.1, w: 3.0, h: 0.65, fill: C.orange, text: "Emergency Condition?", fontSize: 9.5 });
// Sepsis / septic shock
arrow(s, 11.65, 1.75, 11.65, 2.05);
box(s, { x: 10.15, y: 2.05, w: 3.0, h: 1.0, fill: C.white, line: C.orange,
textArr: [
{ text: "Sepsis / Septic Shock\n", options: { bold: true, color: C.orange, fontSize: 9, breakLine: false } },
{ text: "No cytokine-targeted biologic approved\nas standard of care for sepsis.\n", options: { color: C.steel, fontSize: 8.5, breakLine: false } },
{ text: "Anakinra (IL-1RA): emerging evidence in\nmacrophage activation syndrome (MAS/HLH)\nand sHLH complicating sepsis", options: { color: C.red, fontSize: 8.5, bold: true } },
],
align: "left", valign: "top",
});
// HLH / MAS
arrow(s, 11.65, 3.05, 11.65, 3.3);
diamond(s, { x: 10.15, y: 3.3, w: 3.0, h: 0.65, fill: C.orange, text: "Macrophage Activation\nSyndrome (MAS/HLH)?", fontSize: 9 });
arrow(s, 11.65, 3.95, 11.65, 4.22);
box(s, { x: 10.15, y: 4.22, w: 3.0, h: 0.8, fill: C.white, line: C.red,
textArr: [
{ text: "Anakinra (IL-1RA) — first line\n", options: { bold: true, color: C.red, fontSize: 9, breakLine: false } },
{ text: "Tocilizumab (anti-IL-6R) — 2nd line\n", options: { color: C.steel, fontSize: 8.5, breakLine: false } },
{ text: "Emapalumab (anti-IFN-γ) for primary HLH\nin children", options: { color: C.steel, fontSize: 8.5 } },
],
align: "left", valign: "top",
});
// COVID-19 CRS
arrow(s, 11.65, 5.02, 11.65, 5.28);
box(s, { x: 10.15, y: 5.28, w: 3.0, h: 0.9, fill: C.white, line: C.orange,
textArr: [
{ text: "Severe COVID-19 / viral CRS:\n", options: { bold: true, color: C.orange, fontSize: 9, breakLine: false } },
{ text: "Baricitinib (JAKi) — WHO strong recommendation\nTocilizumab — hospitalised, requiring O₂\nDexamethasone — all hospitalised requiring O₂", options: { color: C.steel, fontSize: 8.5 } },
],
align: "left", valign: "top",
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 4 — Quick Reference Table
// ═══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 13.3, h: 7.5, fill: { color: C.navy }, line: { color: C.navy } });
s.addText("Quick Reference — Anti-Cytokine Drugs at a Glance", {
x: 0.3, y: 0.12, w: 12.7, h: 0.45, fontSize: 15, bold: true, color: C.white, align: "center",
});
const rows = [
// [Drug, Target, Disease Use, Class]
["Drug / Class", "Target", "Key Indication(s)", "Monitoring"],
["Infliximab / Adalimumab\nEtanercept / Certolizumab", "TNF-α", "RA, PsA, AS, IBD, Psoriasis", "TB screen, LFTs, HBsAg"],
["Tocilizumab / Sarilumab", "IL-6 receptor", "RA, GCA, CAR-T CRS, COVID-19", "Neutrophil count, LFTs"],
["Anakinra / Canakinumab", "IL-1 / IL-1β", "RA, Still's, gout, MAS/HLH, FMF", "Injection site, neutropenia"],
["Ustekinumab", "IL-12/23 (p40)", "Psoriasis, PsA, Crohn's", "Infections, TB screen"],
["Secukinumab / Ixekizumab", "IL-17A", "Psoriasis, PsA, AS", "IBD caution, candida"],
["Guselkumab / Risankizumab", "IL-23 (p19)", "Psoriasis, PsA, Crohn's (ris.)", "Infections"],
["Dupilumab", "IL-4Rα (IL-4+IL-13)", "Atopic dermatitis, asthma, CRSwNP", "Eosinophilia (transient)"],
["Mepolizumab / Benralizumab", "IL-5 / IL-5Rα", "Severe eosinophilic asthma, EGPA", "Eosinophil count, parasites"],
["Tofacitinib / Baricitinib\nUpadacitinib", "JAK 1/2/3", "RA, PsA, UC, COVID-19, AD", "VTE risk, CBC, lipids, malignancy"],
["Anifrolumab", "IFN-α/β receptor", "Systemic lupus erythematosus", "Infections, herpes zoster"],
["Emapalumab", "IFN-γ", "Primary HLH (paediatric)", "Infections (prophylaxis needed)"],
];
const colW = [2.7, 1.8, 4.4, 3.8];
const colX = [0.15, 2.85, 4.65, 9.05];
const rowH = 0.53;
const startY = 0.65;
rows.forEach((row, ri) => {
const isHeader = ri === 0;
const fillColor = isHeader ? C.teal : (ri % 2 === 0 ? "182D4A" : "152540");
row.forEach((cell, ci) => {
s.addShape(pres.ShapeType.rect, {
x: colX[ci], y: startY + ri * rowH, w: colW[ci], h: rowH,
fill: { color: fillColor }, line: { color: "1A3A5C", width: 0.5 },
});
s.addText(cell, {
x: colX[ci] + 0.07, y: startY + ri * rowH, w: colW[ci] - 0.12, h: rowH,
fontSize: isHeader ? 9.5 : 8.5, bold: isHeader, color: isHeader ? C.white : C.offWhite,
valign: "middle", align: "left", margin: 2,
});
});
});
// Footer note
s.addText("⚠ Check for active infection, TB, hepatitis B, pregnancy, and cardiovascular risk before initiating any biologic or JAK inhibitor.", {
x: 0.2, y: 7.18, w: 12.9, h: 0.25, fontSize: 8.5, color: C.gold, italic: true, align: "center",
});
}
// ─── Write file ───────────────────────────────────────────────────
const outPath = "/home/daytona/workspace/anti-cytokine-flowchart/Anti_Cytokine_Therapy_Flowchart.pptx";
pres.writeFile({ fileName: outPath })
.then(() => console.log("SUCCESS: " + outPath))
.catch(err => { console.error("ERROR:", err); process.exit(1); });
cd /home/daytona/workspace/anti-cytokine-flowchart && node build.js 2>&1
ls -lh /home/daytona/workspace/anti-cytokine-flowchart/Anti_Cytokine_Therapy_Flowchart.pptx
Anti Cytokine Therapy Flowchart
Presentation · PPTX
What's inside (4 slides)
- RA / JIA: csDMARD (MTX) → Anti-TNF → Tocilizumab (IL-6R) → JAK inhibitors → Anakinra/Canakinumab (Still's)
- PsA / AS: IL-17A inhibitors vs. anti-TNF based on skin vs. axial dominance; IL-23 inhibitors for PsA
- SLE: Anifrolumab (anti-IFNαR) / Belimumab / Baricitinib
- GCA / PMR: Tocilizumab + steroid taper
- Pre-biologic screening checklist (TB, HBV, pregnancy, heart failure warning)
- IBD: Vedolizumab, Ustekinumab, Risankizumab, JAK inhibitors, Anti-TNF
- Severe asthma: Eosinophilic → Anti-IL-5 (Mepolizumab/Benralizumab) / Dupilumab; Tezepelumab (any phenotype)
- Atopic dermatitis/urticaria: Dupilumab, Tralokinumab, Omalizumab
- CAR-T CRS: Tocilizumab (grade ≥2), Siltuximab if refractory
- Checkpoint inhibitor irAEs: Steroids, Infliximab (colitis), Tocilizumab (myocarditis)
- MAS/HLH: Anakinra → Tocilizumab → Emapalumab
- Severe COVID-19: Baricitinib (WHO strong recommendation), Tocilizumab, Dexamethasone
cytokines in systemic diseases
cytokines systemic inflammation disease pathogenesis
cytokines systemic diseases 2024 2025 pathogenesis review
Cytokines in Systemic Diseases
1. The Acute-Phase Response: The Prototypic Systemic Cytokine Effect
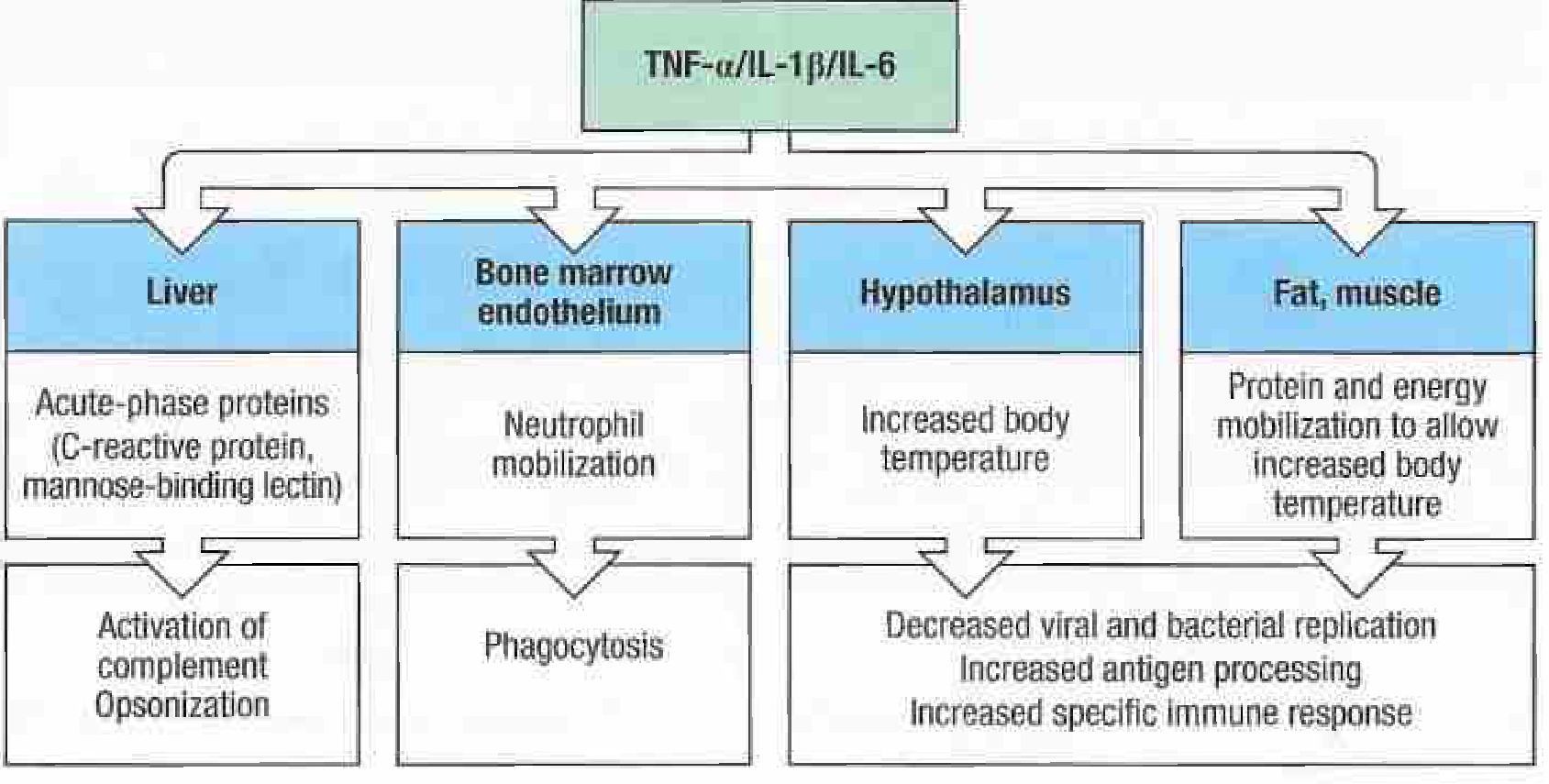
| Target Organ | Effect | Outcome |
|---|---|---|
| Liver | Induces acute-phase proteins (CRP, fibrinogen, SAA, MBL) | Opsonization, complement activation, pathogen neutralization |
| Bone marrow / endothelium | Neutrophil mobilization | Phagocytosis, bacterial killing |
| Hypothalamus | Prostaglandin E2 synthesis via COX-2 → fever | Impaired viral/bacterial replication; enhanced immune response |
| Fat and muscle | Protein and energy mobilization, catabolism | Substrate for thermogenesis and immune cell fuel |
"Endogenous pyrogens cause fever by inducing the synthesis of prostaglandin E2 by the enzyme cyclooxygenase-2... Prostaglandin E2 then acts on the hypothalamus, resulting in an increase in both heat production from the catabolism of brown fat and heat retention from vasoconstriction." - Janeway's Immunobiology 10e
- C-reactive protein (CRP): Binds phosphocholine on bacterial/fungal surfaces - acts as opsonin and activates classical complement. Rises faster than ESR; most clinically used inflammatory marker
- Serum amyloid A (SAA): Can accumulate in tissues in chronic disease causing secondary AA amyloidosis
- Fibrinogen: Elevated ESR; coagulation; contributes to hypercoagulability in inflammatory states
- Mannose-binding lectin (MBL): Activates lectin complement pathway; pattern recognition
2. Sepsis and SIRS: Cytokines Turned Lethal
Mechanism
- IL-1beta and TNF-alpha cause neutrophil adhesion to endothelium at sites remote from infection
- Activated neutrophils release reactive oxygen species (ROS), lysosomal enzymes, and free radicals
- This damages distant organ endothelium, increasing vascular permeability
- Coagulation, complement, and fibrinolytic pathways activate simultaneously
- Result: Multi-Organ Dysfunction Syndrome (MODS) → Multiple System Organ Failure (MSOF)
"Septic manifestations and MODS in SIRS are mediated by the release of pro-inflammatory cytokines such as IL-1 and TNF-alpha. These cytokines... stimulate neutrophil adhesion to endothelial surfaces adjacent to the source of infection... The activated neutrophils adhere to vascular endothelium in key organs remote from the source of infection and damage it, leading to increased vascular permeability... which in turn leads to cellular damage within the organs." - Bailey & Love's Surgery
The Sepsis Cytokine Cascade
| Phase | Key Cytokines | Clinical Effect |
|---|---|---|
| Hyperinflammatory (early) | TNF-alpha, IL-1beta, IL-6, IL-8, IL-12 | Fever, tachycardia, vasodilation, shock |
| Immunosuppressive (late) | IL-10, TGF-beta | Lymphocyte apoptosis, "immune paralysis", secondary infection susceptibility |
| Cytokine storm (toxin-mediated) | TNF-alpha, IL-2 (superantigen-driven) | Toxic shock syndrome - 20-30% T cells activated at once |
- Lungs: IL-8-mediated neutrophil recruitment → ARDS
- Kidneys: Macrophage ROS + pro-inflammatory cytokines → acute tubular necrosis
- Liver: TNF-driven hepatocyte apoptosis; cholestasis
- Brain: Sepsis-associated encephalopathy - occurs in the majority of patients with sepsis and MODS
- Heart: TNF-alpha directly depresses myocardial contractility (negative inotrope)
3. Autoimmune Systemic Diseases
Systemic Lupus Erythematosus (SLE)
- Plasmacytoid dendritic cells (pDCs) produce enormous quantities of IFN-alpha in response to nucleic acid-containing immune complexes
- IFN-alpha activates DCs, promotes autoreactive B and T cells, enhances autoantibody production
- The "interferon signature" (elevated IFN-stimulated gene expression) is detectable in >75% of SLE patients
- Complement deficiency/excess activation triggers IFN production, perpetuating a vicious cycle
- IL-6: Drives B cell differentiation into antibody-secreting plasma cells; elevated in active SLE; levels correlate with anti-dsDNA titres
- BLyS/BAFF: B lymphocyte survival factor - massively overproduced; promotes autoreactive B cell survival (target of belimumab)
- IL-17: Elevated in SLE nephritis; promotes renal inflammation
- IL-10: Paradoxically elevated in SLE - promotes autoreactive B cell survival despite being "anti-inflammatory"
- TNF-alpha: Complex role - may be protective (promoting apoptotic clearance) but drives organ inflammation
- Some autoantibodies in SLE directly target signaling cytokines, acting as natural immunomodulators
Systemic Sclerosis (Scleroderma / SSc)
- TGF-beta: The master fibrotic cytokine - activates fibroblasts, stimulates collagen synthesis, promotes myofibroblast differentiation in skin, lungs, and heart
- IL-4 and IL-13: Th2 cytokines that amplify TGF-beta-driven fibrosis
- IL-6: Promotes fibroblast activation; elevated levels predict worse lung disease
- CXCL4 (PF4): A chemokine elevated early in SSc; correlates with lung fibrosis and pulmonary hypertension
- VEGF: Paradoxically elevated but ineffective - drives abnormal vascular remodeling and pulmonary arterial hypertension (PAH)
Rheumatoid Arthritis (RA) - Systemic Manifestations
- IL-6: Causes anaemia of chronic disease (induces hepcidin, reducing iron availability); elevated CRP/ESR; fatigue; constitutional symptoms
- TNF-alpha: Cachexia (muscle/fat wasting), cardiovascular risk (accelerates atherosclerosis)
- IL-1beta: Bone loss, cartilage catabolism, fever
- Elevated cardiovascular mortality in RA is partly mediated by chronic cytokine-driven endothelial dysfunction and accelerated atherosclerosis
4. Haemophagocytic Lymphohistiocytosis / Macrophage Activation Syndrome (HLH/MAS)
- Failure of cytotoxic T cells and NK cells to eliminate virally infected cells (e.g., EBV) creates a positive feedback loop
- Massive overproduction of cytokines - especially IFN-gamma, IL-6, IL-18, IL-12, TNF-alpha - drives uncontrolled macrophage activation
- Macrophages consume normal marrow elements (hemophagocytosis), causing cytopenias
- Systemic inflammation, coagulopathy (DIC), hepatic failure, and CNS involvement follow
"Failure to kill virally infected cells elicits a positive feedback loop that leads to overproduction of cytokines and excessive activation of macrophages, which often consume normal marrow elements." - Robbins & Kumar Basic Pathology
- Ferritin (>500 µg/L; often >10,000 µg/L in HLH) - reflects macrophage activation
- sCD25 (soluble IL-2 receptor) - T cell activation marker; elevated
- IL-18: Markedly elevated - distinguishes primary HLH from MAS
- IFN-gamma: Drives macrophage activation; target of emapalumab in primary HLH
5. Systemic Inflammation in Gastrointestinal Disease
Inflammatory Bowel Disease (IBD)
- Extraintestinal manifestations (EIMs): Arthritis, uveitis, skin lesions (erythema nodosum, pyoderma gangrenosum) - all cytokine-mediated
- TNF-alpha: The key driver; elevated in mucosa and circulation; anti-TNF therapy (infliximab) revolutionized IBD care
- IL-23/IL-17 axis: Genetic variants in IL-23R associated with Crohn's disease; drives mucosal and systemic inflammation
- IL-6: Systemic acute-phase response; anaemia of chronic disease
- IL-10 deficiency (genetic): Causes severe early-onset IBD by removing the key anti-inflammatory brake
Liver Disease (Hepatic Cytokine Effects)
- TNF-alpha and IL-6 drive hepatic stellate cell activation → cirrhosis and fibrosis in chronic viral hepatitis, NASH
- IL-6: Hepatocyte growth factor (hepatoprotective in acute injury but pro-oncogenic in chronic HCC)
- In NASH/metabolic-associated fatty liver disease (MAFLD): TNF-alpha and IL-6 produced by visceral adipose tissue macrophages drive hepatic steatosis, insulin resistance, and progression to cirrhosis
6. Cytokines in Renal Disease
- Pro-inflammatory cytokines (IL-1, TNF, IL-6): Produced by macrophages infiltrating the renal interstitium; generate ROS and nitric oxide that directly damage tubular cells; correlate with degree of renal dysfunction
- TGF-beta: The dominant pro-fibrotic cytokine in the kidney - promotes epithelial-to-mesenchymal transition (EMT) of tubular cells into fibroblasts, depositing collagen in the interstitium
- Chemokines (CCL2/MCP-1): Recruit monocytes/macrophages into the interstitium, amplifying inflammation
- Tubule epithelial cells themselves synthesize cytokines and chemokines when exposed to excess filtered protein (proteinuria), activating local DCs and T cells
"Direct damage to resident cells is caused through the generation by macrophages of reactive oxygen species, nitric oxide, complement factors, and proinflammatory cytokines. Macrophages can also affect the supporting matrix and vasculature through the expression of metalloproteinases and vasoactive peptides." - Brenner & Rector's The Kidney
7. Cytokines in Cancer (Systemic Effects)
| Cytokine | Source | Effect in Cancer |
|---|---|---|
| TGF-beta | Tumour cells, Tregs | Suppresses T cell killing; promotes tumour invasion and metastasis |
| IL-10 | Tumour-infiltrating macrophages, Tregs | Impairs DC maturation; systemic immunosuppression |
| IL-6 | Tumour cells, TME stroma | Promotes STAT3-driven tumour cell survival; supports plasma cell myeloma growth; drives cachexia |
| VEGF | Tumour cells | Systemic angiogenesis; promotes metastatic niche |
| TNF-alpha | Tumour cells and macrophages | Chronic low-level expression activates NF-kB → tumour survival and immune evasion |
| IL-2 | Therapeutic use | Expands anti-tumour T cells; used in melanoma and renal cell carcinoma |
| IFN-alpha | Therapeutic use | Anti-proliferative, pro-apoptotic; hairy cell leukaemia, melanoma |
- Cachexia / cancer wasting: TNF-alpha and IL-6 drive profound muscle and fat catabolism
- Anaemia of chronic disease: IL-6 induces hepcidin, blocking iron mobilization
- Fever: IL-1, IL-6, TNF act as endogenous pyrogens
- Hypercalcaemia: PTHrP + IL-6 drive osteoclast activation (myeloma, solid tumours)
8. Cytokines in Cardiovascular and Metabolic Disease
- IL-6, TNF-alpha, IL-1beta: Promote endothelial activation, VCAM-1/ICAM-1 upregulation, monocyte recruitment into plaques
- CANTOS trial (canakinumab, anti-IL-1beta): Reduced cardiovascular events independently of lipid lowering - confirming the causal role of IL-1beta in atherosclerosis
- IL-18: Destabilizes atherosclerotic plaques; promotes vulnerable plaque formation
- Visceral adipose tissue macrophages produce IL-6 and TNF-alpha chronically
- TNF-alpha inhibits insulin receptor signaling (serine phosphorylation of IRS-1) → insulin resistance
- IL-6 induces hepatic insulin resistance
- Adiponectin (an anti-inflammatory adipokine) is reduced in obesity, removing its protective cytokine-suppressing effects
9. Cytokines in Neurological Disease
- Type I interferons (IFN-beta): Pathogenic in multiple sclerosis (MS); IFN-beta therapy reduces relapse by modulating Th1/Th17 activity
- IL-17: Elevated in MS plaques; promotes blood-brain barrier disruption
- TNF-alpha, IL-1, IL-6: Elevated in CSF during neuroinflammation (encephalitis, MS)
- Sepsis-associated encephalopathy: Systemic cytokine spillover into the CNS causes confusion and coma in sepsis (occurs in the majority of septic patients with MODS)
- Alzheimer's disease: Microglia produce IL-1beta, TNF-alpha, and IL-6 in response to amyloid-beta; chronic neuroinflammation accelerates neurodegeneration
Summary: Cytokine Roles Across Systemic Diseases
| Disease / Condition | Dominant Cytokines | Net Effect |
|---|---|---|
| Acute-phase response | TNF-alpha, IL-1beta, IL-6 | CRP, fever, neutrophilia, metabolic catabolism |
| Sepsis / SIRS | IL-1, TNF, IL-6, IL-8 → late IL-10 | MODS, shock, organ failure, immune paralysis |
| SLE | Type I IFNs, BLyS, IL-6, IL-17 | Autoantibodies, nephritis, multi-organ damage |
| Systemic sclerosis | TGF-beta, IL-6, IL-4/13 | Progressive fibrosis (skin, lung, heart) |
| RA (systemic) | TNF, IL-6, IL-1 | Anaemia, cardiovascular disease, cachexia |
| HLH / MAS | IFN-gamma, IL-18, IL-6, IL-12 | Cytophagocytosis, cytopenias, DIC, organ failure |
| IBD | TNF, IL-23/17, IL-6 | Extraintestinal manifestations, anaemia |
| CKD / renal fibrosis | TGF-beta, IL-1, TNF, MCP-1 | Tubulointerstitial fibrosis, progression to ESRD |
| Cancer | TGF-beta, IL-10, IL-6, TNF | Immune evasion, cachexia, paraneoplastic syndromes |
| Atherosclerosis | IL-1beta, IL-6, TNF, IL-18 | Plaque formation, acute coronary syndromes |
| Metabolic syndrome | TNF, IL-6 | Insulin resistance, hepatic steatosis |
| Neurological disease | Type I IFNs, IL-17, TNF | BBB disruption, neurodegeneration, encephalopathy |
- Janeway's Immunobiology 10e - Acute-phase response, type I interferons, systemic cytokine effects
- Bailey & Love's Surgery - Sepsis, SIRS, MODS pathophysiology
- Firestein & Kelley's Textbook of Rheumatology - Autoimmune disease cytokine networks
- Rheumatology (Elsevier 2022) - SLE, complement, autoimmune cytokine loops
- Brenner & Rector's The Kidney - Renal interstitial cytokines, TGF-beta, fibrosis
- Robbins & Kumar Basic Pathology - HLH/macrophage activation syndrome
- Recent literature: 2025 cytokine storm review | EULAR/ACR HLH guidelines (PMID: 37487610)
anaesthetic managaement in laproscopic surgery ppt
mkdir -p /home/daytona/workspace/laparoscopic-anaesthesia-ppt
~/laparoscopic-anaesthesia-ppt/build.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_WIDE"; // 13.3 × 7.5 inches
pres.title = "Anaesthetic Management in Laparoscopic Surgery";
pres.author = "Orris Medical AI";
// ── Palette ──────────────────────────────────────────────────────
const C = {
navy: "0A1628",
teal: "0E7490",
tealLt: "22D3EE",
tealDk: "164E63",
amber: "D97706",
amberLt: "FCD34D",
red: "B91C1C",
redLt: "FCA5A5",
green: "166534",
greenLt: "86EFAC",
purple: "6D28D9",
purpleLt:"C4B5FD",
orange: "C2410C",
slate: "334155",
white: "FFFFFF",
offWhite:"F8FAFC",
ltGray: "E2E8F0",
midGray: "94A3B8",
gold: "F59E0B",
lime: "15803D",
};
// ── Helpers ───────────────────────────────────────────────────────
function bg(s, color) {
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:13.3, h:7.5, fill:{color}, line:{color} });
}
function headerBar(s, text, sub) {
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:13.3, h:1.1, fill:{color:C.navy}, line:{color:C.navy} });
s.addShape(pres.ShapeType.rect, { x:0, y:1.1, w:13.3, h:0.06, fill:{color:C.teal}, line:{color:C.teal} });
s.addText(text, { x:0.35, y:0.1, w:12.6, h:0.6, fontSize:22, bold:true, color:C.white });
if (sub) s.addText(sub, { x:0.35, y:0.68, w:12.6, h:0.38, fontSize:12, color:C.tealLt });
}
function card(s, x, y, w, h, title, items, titleColor, accentColor) {
s.addShape(pres.ShapeType.roundRect, { x, y, w, h, fill:{color:C.white}, line:{color:accentColor||C.teal, width:1.8}, rectRadius:0.14 });
s.addShape(pres.ShapeType.roundRect, { x, y, w, h:0.36, fill:{color:accentColor||C.teal}, line:{color:accentColor||C.teal}, rectRadius:0.14 });
// cover bottom corners of top bar
s.addShape(pres.ShapeType.rect, { x, y:y+0.22, w, h:0.14, fill:{color:accentColor||C.teal}, line:{color:accentColor||C.teal} });
s.addText(title, { x:x+0.1, y:y+0.02, w:w-0.2, h:0.32, fontSize:10, bold:true, color:C.white, valign:"middle" });
const bulletArr = items.map((t,i)=>({
text: t,
options:{ bullet:true, color:C.slate, fontSize:9, breakLine: i<items.length-1 }
}));
s.addText(bulletArr, { x:x+0.12, y:y+0.4, w:w-0.22, h:h-0.48, valign:"top", margin:2 });
}
function badge(s, x, y, text, fill, textColor=C.white) {
s.addShape(pres.ShapeType.roundRect, { x, y, w:2.5, h:0.34, fill:{color:fill}, line:{color:fill}, rectRadius:0.1 });
s.addText(text, { x, y, w:2.5, h:0.34, fontSize:10, bold:true, color:textColor, align:"center", valign:"middle" });
}
function sectionPill(s, x, y, text, fill) {
s.addShape(pres.ShapeType.roundRect, { x, y, w:12.6, h:0.38, fill:{color:fill}, line:{color:fill}, rectRadius:0.1 });
s.addText(text, { x:x+0.15, y, w:12.3, h:0.38, fontSize:11, bold:true, color:C.white, valign:"middle" });
}
function twoCol(s, leftCards, rightCards, startY, cardW=6.1, gap=0.3) {
leftCards.forEach(c => card(s, 0.35, c.y, cardW, c.h, c.title, c.items, C.white, c.color||C.teal));
rightCards.forEach(c => card(s, 0.35+cardW+gap, c.y, cardW, c.h, c.title, c.items, C.white, c.color||C.teal));
}
function footer(s, text=`Source: Barash, Cullen & Stoelting's Clinical Anesthesia 9e | Miller's Anesthesia 10e`) {
s.addShape(pres.ShapeType.rect, { x:0, y:7.28, w:13.3, h:0.22, fill:{color:C.navy}, line:{color:C.navy} });
s.addText(text, { x:0.3, y:7.28, w:12.7, h:0.22, fontSize:7.5, color:C.midGray, align:"center", valign:"middle" });
}
// ═══════════════════════════════════════════════════════════════
// SLIDE 1 — TITLE
// ═══════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
// Deep gradient-like background
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:13.3, h:7.5, fill:{color:C.navy}, line:{color:C.navy} });
s.addShape(pres.ShapeType.rect, { x:0, y:4.5, w:13.3, h:3.0, fill:{color:C.tealDk}, line:{color:C.tealDk} });
// Accent lines
s.addShape(pres.ShapeType.rect, { x:0, y:4.48, w:13.3, h:0.05, fill:{color:C.tealLt}, line:{color:C.tealLt} });
s.addShape(pres.ShapeType.rect, { x:0.35, y:1.8, w:0.07, h:1.8, fill:{color:C.tealLt}, line:{color:C.tealLt} });
s.addText("Anaesthetic Management in", { x:0.6, y:1.3, w:12.1, h:0.65, fontSize:28, bold:false, color:C.tealLt });
s.addText("Laparoscopic Surgery", { x:0.6, y:1.9, w:12.1, h:0.9, fontSize:42, bold:true, color:C.white });
s.addText("A comprehensive clinical overview for anaesthesiologists", {
x:0.6, y:2.88, w:12.1, h:0.4, fontSize:14, color:C.midGray, italic:true
});
// Topic pills
const topics = [
{t:"Physiology of Pneumoperitoneum", c:C.teal},
{t:"Preoperative Assessment", c:C.purple},
{t:"Intraoperative Management", c:C.orange},
{t:"Complications & Recovery", c:C.red},
];
let px = 0.6;
topics.forEach(tp => {
const w = 2.85;
s.addShape(pres.ShapeType.roundRect, { x:px, y:4.9, w, h:0.42, fill:{color:tp.c}, line:{color:tp.c}, rectRadius:0.1 });
s.addText(tp.t, { x:px, y:4.9, w, h:0.42, fontSize:9.5, bold:true, color:C.white, align:"center", valign:"middle" });
px += w + 0.25;
});
// Bottom info
s.addText([
{text:"Reference: ", options:{bold:true, color:C.amberLt, fontSize:10}},
{text:"Barash, Cullen & Stoelting's Clinical Anesthesia, 9e (Chapter 44) | Miller's Anesthesia, 10e (Chapter 50)", options:{color:C.midGray, fontSize:10}},
], { x:0.6, y:5.62, w:12.1, h:0.35, margin:0 });
s.addText([
{text:"Key principle: ", options:{bold:true, color:C.amberLt, fontSize:10}},
{text:"General endotracheal anaesthesia (GETA) with muscle relaxation and controlled mechanical ventilation is the preferred technique for laparoscopic surgery.", options:{color:C.ltGray, fontSize:10}},
], { x:0.6, y:5.95, w:12.1, h:0.42, margin:0 });
}
// ═══════════════════════════════════════════════════════════════
// SLIDE 2 — ADVANTAGES & BASICS
// ═══════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
bg(s, C.offWhite);
headerBar(s, "Overview & Advantages of Laparoscopy", "Minimally invasive technique — key concepts for the anaesthesiologist");
card(s, 0.35, 1.3, 5.9, 2.2, "Advantages Over Open Surgery", [
"Small (~1 cm) skin incisions — reduced postoperative pain",
"Lower wound infection rates & blood loss",
"Faster recovery and shorter hospital stay",
"Equivalent oncological outcomes (colorectal, urologic)",
"Better visualisation with magnified camera view",
"NICE recommends laparoscopic colorectal surgery for suitable patients",
], C.white, C.teal);
card(s, 6.55, 1.3, 6.4, 2.2, "Disadvantages & Anaesthetic Challenges", [
"Physiologic derangements from pneumoperitoneum",
"Extreme patient positioning required",
"Longer operative times vs. open surgery",
"Higher equipment costs",
"Limited patient access in robotic surgery",
"Cardiopulmonary instability — especially in high-risk patients",
], C.white, C.orange);
card(s, 0.35, 3.65, 5.9, 1.85, "Pneumoperitoneum: How it Works", [
"CO₂ insufflation via Veress needle → intraperitoneal pressure",
"Target IAP: 12–15 mmHg (max 15 mmHg)",
"CO₂ preferred: highly soluble in blood, non-flammable, safe with diathermy",
"Automated insufflator maintains preset IAP",
"Alternative: gasless abdominal wall lift (rarely used)",
], C.white, C.purple);
card(s, 6.55, 3.65, 6.4, 1.85, "Patient Positioning Used", [
"Trendelenburg (head-down): pelvic / lower abdominal surgery",
"Reverse Trendelenburg (head-up): upper abdominal / bariatric",
"Lateral decubitus: nephrectomy, adrenalectomy",
"Lithotomy + Trendelenburg: gynaecology, robotic prostatectomy",
"Combination positions worsen physiologic derangements",
], C.white, C.purple);
// Why CO2?
s.addShape(pres.ShapeType.roundRect, { x:0.35, y:5.65, w:12.6, h:1.4, fill:{color:C.navy}, line:{color:C.navy}, rectRadius:0.12 });
s.addText("Why CO₂ for Insufflation?", { x:0.55, y:5.7, w:5, h:0.3, fontSize:11, bold:true, color:C.amberLt });
const co2 = [
["Highly blood-soluble","Rapid pulmonary clearance if vascular embolism occurs"],
["Non-flammable","Safe with electrocautery — no fire/explosion risk"],
["Non-oxidising","Does not support combustion"],
["Rapidly absorbed","Metabolised/excreted quickly reducing anaesthesia duration"],
];
co2.forEach((row, i) => {
const cx = 0.55 + i * 3.1;
s.addText("✓ " + row[0], { x:cx, y:6.05, w:3.0, h:0.25, fontSize:9.5, bold:true, color:C.tealLt });
s.addText(row[1], { x:cx, y:6.3, w:3.0, h:0.5, fontSize:8.5, color:C.ltGray });
});
footer(s);
}
// ═══════════════════════════════════════════════════════════════
// SLIDE 3 — CARDIOVASCULAR PHYSIOLOGY
// ═══════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
bg(s, C.offWhite);
headerBar(s, "Cardiovascular Physiology of Pneumoperitoneum", "CO₂ insufflation + positioning cause predictable, manageable haemodynamic changes");
// Central diagram concept
s.addShape(pres.ShapeType.roundRect, { x:4.8, y:1.25, w:3.7, h:1.0, fill:{color:C.navy}, line:{color:C.tealLt, width:2}, rectRadius:0.14 });
s.addText("CO₂ Pneumoperitoneum\n+ Patient Position", { x:4.8, y:1.25, w:3.7, h:1.0, fontSize:12, bold:true, color:C.white, align:"center", valign:"middle" });
// Left effects
const leftEff = [
{t:"↑ SVR (Systemic Vascular Resistance)", c:C.red, y:1.25},
{t:"↑ MAP (Mean Arterial Pressure)", c:C.red, y:1.72},
{t:"↑ Myocardial O₂ Consumption", c:C.orange, y:2.19},
{t:"↓ Venous Return (IVC compression)", c:C.red, y:2.66},
];
leftEff.forEach(e => {
s.addShape(pres.ShapeType.roundRect, { x:0.35, y:e.y, w:4.25, h:0.38, fill:{color:e.c}, line:{color:e.c}, rectRadius:0.08 });
s.addText(e.t, { x:0.4, y:e.y, w:4.15, h:0.38, fontSize:9.5, bold:true, color:C.white, valign:"middle" });
// Arrow
s.addShape(pres.ShapeType.line, { x:4.6, y:e.y+0.19, w:0.2, h:0, line:{color:C.slate, width:1.5, endArrowType:"triangle"} });
});
// Right effects
const rightEff = [
{t:"Dysrhythmias (CO₂ / vagal)", c:C.red, y:1.25},
{t:"Reduced Cardiac Output", c:C.orange, y:1.72},
{t:"↓ Renal / Portal / Splanchnic Flow", c:C.orange, y:2.19},
{t:"VTE risk ↑ (femoral vein stasis)", c:C.orange, y:2.66},
];
rightEff.forEach(e => {
s.addShape(pres.ShapeType.roundRect, { x:8.7, y:e.y, w:4.25, h:0.38, fill:{color:e.c}, line:{color:e.c}, rectRadius:0.08 });
s.addText(e.t, { x:8.75, y:e.y, w:4.15, h:0.38, fontSize:9.5, bold:true, color:C.white, valign:"middle" });
s.addShape(pres.ShapeType.line, { x:8.5, y:e.y+0.19, w:0.2, h:0, line:{color:C.slate, width:1.5, endArrowType:"triangle"} });
});
// IAP mechanism
sectionPill(s, 0.35, 3.22, "Mechanism: Intra-Abdominal Pressure (IAP) Effects on Heart", C.tealDk);
card(s, 0.35, 3.68, 3.9, 2.0, "Low IAP (< 10 mmHg)", [
"IVC compression minimal",
"Venous return maintained or slightly ↑",
"CO relatively preserved",
"Preferred target in high-risk patients",
], C.white, C.green);
card(s, 4.45, 3.68, 4.3, 2.0, "High IAP (> 15 mmHg)", [
"IVC compressed — venous return ↓↓",
"Cardiac filling ↓ → CO ↓",
"Combined with hypovolaemia = cardiovascular collapse",
"Associated with postoperative AKI",
"AVOID IAP > 15 mmHg",
], C.white, C.red);
card(s, 8.95, 3.68, 3.9, 2.0, "Hypercarbia (absorbed CO₂)", [
"Acidosis → ↓ myocardial contractility",
"Dysrhythmias",
"Arterial vasodilation (paradoxical hypotension)",
"↑ Catecholamine release",
"Monitor ETCO₂ continuously",
], C.white, C.orange);
// Bottom warning
s.addShape(pres.ShapeType.roundRect, { x:0.35, y:5.85, w:12.6, h:1.15, fill:{color:"FFF7ED"}, line:{color:C.amber, width:1.5}, rectRadius:0.1 });
s.addText("⚠ Clinical Pearls", { x:0.55, y:5.9, w:3, h:0.3, fontSize:11, bold:true, color:C.amber });
s.addText([
{text:"• Severe hypotension during pneumoperitoneum → desufflate immediately; may require conversion to open procedure\n", options:{color:C.slate, fontSize:9, breakLine:false}},
{text:"• High IAP + hypovolaemia = severe cardiac failure risk • Position Trendelenburg initially improves venous return, but impairs respiratory mechanics\n", options:{color:C.slate, fontSize:9, breakLine:false}},
{text:"• Cardiac ischaemia can develop in patients with coronary artery disease — have vasopressors and inotropes available", options:{color:C.red, fontSize:9, bold:true}},
], { x:0.55, y:6.2, w:12.2, h:0.72, margin:0, valign:"top" });
footer(s);
}
// ═══════════════════════════════════════════════════════════════
// SLIDE 4 — RESPIRATORY PHYSIOLOGY
// ═══════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
bg(s, C.offWhite);
headerBar(s, "Respiratory Physiology of Pneumoperitoneum", "Ventilatory management is critical — understand the mechanical and metabolic effects");
sectionPill(s, 0.35, 1.22, "Mechanical Effects (Pneumoperitoneum + Trendelenburg)", C.tealDk);
const mechCards = [
{title:"↓ FRC & Vital Capacity", items:["Diaphragm displaced cephalad","Reduced lung volume available for ventilation","Basal atelectasis — especially in obese patients","Worsened in Trendelenburg position"], color:C.red, y:1.68},
{title:"↓ Pulmonary Compliance", items:["Stiff lungs = higher peak airway pressure needed","↑ Peak inspiratory pressure (PIP)","Risk of barotrauma at high pressures","V/Q mismatch → hypoxaemia"], color:C.orange, y:1.68},
{title:"ETT Migration Risk", items:["Diaphragm pushed up into thorax","ETT may advance into right main bronchus","Check bilateral breath sounds after position change","Confirm tube position after insufflation"], color:C.red, y:1.68},
];
const mW = 4.0;
mechCards.forEach((c, i) => {
card(s, 0.35 + i*(mW+0.22), 1.68, mW, 2.2, c.title, c.items, C.white, c.color);
});
sectionPill(s, 0.35, 4.0, "Metabolic Effect: CO₂ Absorption & Respiratory Acidosis", C.tealDk);
card(s, 0.35, 4.46, 5.9, 2.0, "CO₂ Absorption Pathway", [
"CO₂ absorbed from peritoneal surface into bloodstream",
"↑ PaCO₂ and ↑ ETCO₂",
"Respiratory acidosis if ventilation not adjusted",
"Require ↑ minute ventilation to maintain normocapnia",
"Rate of absorption varies with IAP and vascularity",
"Subcutaneous emphysema = massive CO₂ absorption",
], C.white, C.teal);
card(s, 6.55, 4.46, 6.4, 2.0, "Ventilatory Strategy", [
"Increase tidal volume or RR to compensate for CO₂",
"Target ETCO₂ 35–45 mmHg (higher acceptable if needed)",
"PEEP (5–8 cmH₂O): reduces atelectasis, improves oxygenation",
"Low tidal volumes (6–8 mL/kg IBW) — lung-protective",
"Recruitment manoeuvres for refractory hypoxaemia",
"FiO₂ titrated to SpO₂ > 95%",
], C.white, C.green);
// key note
s.addShape(pres.ShapeType.roundRect, { x:0.35, y:6.6, w:12.6, h:0.58, fill:{color:C.navy}, line:{color:C.navy}, rectRadius:0.1 });
s.addText([
{text:"Key: ", options:{bold:true, color:C.amberLt, fontSize:10}},
{text:"Reductions in pulmonary compliance and FRC, combined with CO₂ absorption, often cause respiratory acidosis. Cephalad displacement of abdominal contents — particularly in obese patients — adds atelectasis and V/Q mismatch. ETCO₂ monitoring is mandatory.", options:{color:C.ltGray, fontSize:9.5}},
], { x:0.55, y:6.62, w:12.2, h:0.52, valign:"middle", margin:0 });
footer(s);
}
// ═══════════════════════════════════════════════════════════════
// SLIDE 5 — REGIONAL PERFUSION & CNS EFFECTS
// ═══════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
bg(s, C.offWhite);
headerBar(s, "Regional Perfusion & CNS/Ocular Effects", "Pneumoperitoneum reduces splanchnic and renal perfusion; raises ICP and IOP");
card(s, 0.35, 1.28, 3.85, 2.7, "Renal Effects", [
"↓ Renal blood flow due to direct compression",
"↓ GFR and urine output during pneumoperitoneum",
"↑ Vasopressin → reduced free-water excretion",
"Activation of renin–angiotensin system",
"IAP >15 mmHg → postoperative AKI risk",
"Oliguria may persist post-nephrectomy despite haemodynamic stability (self-limited)",
"Preoperative renal impairment, HTN = increased risk",
"Hydration + limiting IAP <12 mmHg — protective strategy",
], C.white, C.teal);
card(s, 4.4, 1.28, 4.15, 2.7, "Splanchnic/Hepatic Effects", [
"↓ Intestinal blood flow (compression + vasoconstriction)",
"Hypercapnia-driven mesenteric vasodilatation (partially offsets)",
"↓ Hepatic arterial and portal flow",
"Bowel ischaemia risk in prolonged procedures",
"↓ Splanchnic flow → reduced drug hepatic clearance",
"Relevant in bariatric surgery (already altered liver function)",
], C.white, C.orange);
card(s, 8.75, 1.28, 4.2, 2.7, "Femoral/IVC Effects", [
"IVC compressed by IAP → femoral vein stasis",
"↓ Femoral venous blood flow",
"↑ DVT / VTE risk — particularly in long procedures",
"Pneumatic compression stockings mandatory",
"Early mobilisation postoperatively",
"Pharmacological thromboprophylaxis as indicated",
], C.white, C.purple);
sectionPill(s, 0.35, 4.15, "CNS & Ocular Effects (Critical in Steep Trendelenburg / Robotic Surgery)", C.tealDk);
card(s, 0.35, 4.62, 5.9, 2.3, "Intracranial Pressure (ICP) Effects", [
"Both pneumoperitoneum AND Trendelenburg ↑ ICP",
"Mechanism: ↓ cerebral venous outflow + hypercarbia → cerebral hyperperfusion",
"↑ Cerebral blood flow & ↑ cerebral perfusion pressure",
"Regional cerebral O₂ saturation is increased (usually well-tolerated)",
"Prolonged steep Trendelenburg → acute postoperative cerebral oedema",
"Contraindicated/extreme caution: known intracranial pathology, raised ICP, cerebrovascular disease",
"Catecholamine release adds to systemic haemodynamic effects",
], C.white, C.red);
card(s, 6.55, 4.62, 6.4, 2.3, "Intraocular Pressure (IOP) Effects", [
"IOP ↑ significantly during robotic prostatectomy (steep Trendelenburg)",
"Mechanism: ↑ CVP from Trendelenburg + ↑ choroidal blood volume from hypercarbia",
"Rare: postoperative blindness (ischaemic optic neuropathy) reported",
"Risk factors: glaucoma, diabetes, atherosclerosis, anaemia",
"Keep ETCO₂ within normal range to limit hypercarbia contribution",
"Limit total duration of steep Trendelenburg where possible",
"Ophthalmology review if visual symptoms postoperatively",
], C.white, C.orange);
footer(s);
}
// ═══════════════════════════════════════════════════════════════
// SLIDE 6 — PREOPERATIVE ASSESSMENT
// ═══════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
bg(s, C.offWhite);
headerBar(s, "Preoperative Assessment & Patient Selection", "Identify high-risk patients — comorbidities amplify pneumoperitoneum-related derangements");
card(s, 0.35, 1.28, 5.9, 2.35, "Cardiovascular Assessment", [
"History of IHD, HF, valvular disease — cardiology review",
"Uncontrolled hypertension — optimise before elective surgery",
"Cardiac disease → ECG, ECHO if indicated",
"High risk: may require arterial line, invasive monitoring",
"Poor LV function: pneumoperitoneum may not be tolerated",
"NYHA Class III–IV: discuss risks/benefits; consider open approach",
"Antiplatelet and anticoagulant management plan",
], C.white, C.red);
card(s, 6.55, 1.28, 6.4, 2.35, "Respiratory Assessment", [
"Severe COPD / asthma: may not tolerate CO₂ retention",
"Obesity: ↑ risk of hypoxaemia, atelectasis, difficult airway",
"OSA: CPAP continuation, post-op monitoring required",
"Pulmonary HTN: elevated IAP may critically ↓ RV output",
"Spirometry / ABG if significant respiratory compromise",
"CXR if new or unexplained symptoms",
"Optimise inhalers before elective surgery",
], C.white, C.teal);
card(s, 0.35, 3.75, 3.85, 2.35, "High-Risk Groups", [
"BMI >40 with obesity comorbidities → ↑ perioperative complications",
"Elderly patients: reduced cardiorespiratory reserve",
"Renal impairment: AKI risk with high IAP",
"Diabetes: AKI risk in bariatric surgery",
"Cerebrovascular disease: ICP concerns in Trendelenburg",
"Previous abdominal surgery: adhesions, trocar injury risk",
], C.white, C.orange);
card(s, 4.4, 3.75, 4.15, 2.35, "Airway Assessment", [
"Obesity: predict difficult laryngoscopy",
"Mallampati, thyromental distance, neck mobility",
"Consider awake FOB in difficult airway",
"RSI for high aspiration risk (obese, hiatus hernia)",
"Confirm ETT position after insufflation and positioning",
"Have airway adjuncts immediately available",
], C.white, C.purple);
card(s, 8.75, 3.75, 4.2, 2.35, "Preoperative Preparation", [
"NBM fasting: solids 6h, clear fluids 2h (ERAS protocol)",
"Continue antihypertensives (hold ACEi/ARB morning of surgery per local policy)",
"DVT prophylaxis: TED stockings + LMWH",
"Pre-oxygenation: 3 min tidal breathing or 8 deep breaths in 60s",
"Antacid premedication for aspiration risk",
"Inform patient: shoulder-tip pain from diaphragmatic irritation",
], C.white, C.green);
footer(s);
}
// ═══════════════════════════════════════════════════════════════
// SLIDE 7 — INTRAOPERATIVE MANAGEMENT
// ═══════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
bg(s, C.offWhite);
headerBar(s, "Intraoperative Anaesthetic Management", "GETA with muscle relaxation and controlled ventilation — standard of care");
sectionPill(s, 0.35, 1.22, "Anaesthetic Technique: General Endotracheal Anaesthesia (GETA) — Preferred Approach", C.tealDk);
card(s, 0.35, 1.68, 3.85, 2.0, "Induction", [
"Standard IV induction: propofol + fentanyl/remifentanil",
"RSI (suxamethonium or high-dose rocuronium) if aspiration risk",
"Cuffed ETT — LMA acceptable only for brief, minor cases",
"Confirm ETT position — bilateral air entry",
"Secure ETT well — position changes may displace tube",
], C.white, C.navy);
card(s, 4.4, 1.68, 4.15, 2.0, "Maintenance", [
"Volatile agent (sevoflurane/desflurane) or TIVA (propofol)",
"TIVA preferred: ↓ PONV, avoids N₂O (distends bowel)",
"Remifentanil infusion for analgesia during laparoscopy",
"Avoid N₂O — increases bowel distension & PONV risk",
"Depth-of-anaesthesia monitoring (BIS) optional",
], C.white, C.navy);
card(s, 8.75, 1.68, 4.2, 2.0, "Muscle Relaxation", [
"Deep NMB improves surgical access",
"Lower IAP required = less physiological derangement",
"Allows ↓ insufflation pressure while maintaining exposure",
"Monitor with TOF or PTC",
"Reverse fully before extubation (sugammadex preferred)",
"Assessment can be highly subjective — use nerve stimulator",
], C.white, C.purple);
sectionPill(s, 0.35, 3.82, "Monitoring — Mandatory & Optional", C.tealDk);
card(s, 0.35, 4.28, 5.9, 2.65, "Mandatory Monitoring", [
"ECG — detect dysrhythmias from hypercarbia/vagal stimulation",
"Non-invasive blood pressure (NIBP) — or arterial line in high-risk",
"Capnography (ETCO₂) — essential: CO₂ absorption monitoring",
"Pulse oximetry (SpO₂)",
"Temperature — gas insufflation causes heat loss",
"Airway pressure monitoring — detect tube migration, bronchospasm",
"Urine output (catheter) — monitor renal perfusion",
], C.white, C.teal);
card(s, 6.55, 4.28, 6.4, 2.65, "Situational / High-Risk Monitoring", [
"Arterial line (A-line): high-risk cardiac/respiratory disease",
"Central venous line: major blood loss risk, vasopressor infusions",
"Cardiac output monitoring: FloTrac, TOE — cardiac surgery risk",
"Neuromuscular blockade monitor (TOF, PTC) — mandatory NMB cases",
"Depth-of-anaesthesia (BIS/entropy) — TIVA cases",
"Near-infrared cerebral oximetry (rSO₂) — prolonged steep Trendelenburg",
"Intraocular pressure monitoring — not routine; at-risk patients",
], C.white, C.purple);
footer(s);
}
// ═══════════════════════════════════════════════════════════════
// SLIDE 8 — VENTILATION & FLUID MANAGEMENT
// ═══════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
bg(s, C.offWhite);
headerBar(s, "Mechanical Ventilation & Fluid Management", "Lung-protective ventilation + goal-directed fluid therapy = key ERAS components");
sectionPill(s, 0.35, 1.22, "Ventilation Strategy: Lung-Protective Approach", C.tealDk);
card(s, 0.35, 1.68, 5.9, 2.4, "Ventilatory Parameters", [
"Tidal volume (TV): 6–8 mL/kg Ideal Body Weight (IBW)",
"PEEP: 5–8 cmH₂O — reduces atelectasis, improves oxygenation",
"Respiratory rate: adjust to maintain ETCO₂ 35–45 mmHg",
"FiO₂: minimum required to maintain SpO₂ >95%",
"Pressure-controlled ventilation (PCV) preferred in obese patients",
"Inspiration:expiration ratio 1:2 — may need adjustment",
"Peak airway pressure target <30 cmH₂O",
], C.white, C.teal);
card(s, 6.55, 1.68, 6.4, 2.4, "Managing CO₂ Accumulation", [
"ETCO₂ rises after insufflation — increase minute ventilation",
"ETCO₂ spike: consider subcutaneous emphysema, gas embolism",
"PaCO₂ / ETCO₂ gradient widens in V/Q mismatch (obesity, COPD)",
"Consider ABG if ETCO₂ unreliable (severe cardiorespiratory disease)",
"Severe hypercarbia + acidosis → reduce IAP, increase ventilation",
"Recruitment manoeuvres: 30–40 cmH₂O for 30s for refractory hypoxaemia",
"At end of procedure: hand-ventilate to expel residual CO₂",
], C.white, C.orange);
sectionPill(s, 0.35, 4.22, "Fluid Management (ERAS Goal-Directed Approach)", C.tealDk);
card(s, 0.35, 4.68, 3.85, 2.15, "Principles", [
"Avoid over-hydration — worsens airway oedema",
"Goal-directed fluid therapy (GDFT) based on flow parameters",
"Maintain urine output >0.5 mL/kg/hr (target >2 mL/kg/hr reassuring)",
"No evidence for furosemide / mannitol / 'renal-dose' dopamine in AKI prevention",
], C.white, C.teal);
card(s, 4.4, 4.68, 4.15, 2.15, "Warming", [
"CO₂ gas causes significant heat loss",
"Active patient warming (forced-air blanket) mandatory",
"Warm IV fluids and blood products",
"Heated and humidified CO₂ insufflation where available",
"Target normothermia (36–37.5°C) — reduces PONV, infection, coagulopathy",
], C.white, C.purple);
card(s, 8.75, 4.68, 4.2, 2.15, "Vasopressors & Inotropes", [
"Phenylephrine (pure vasoconstrictor) for low SVR",
"Vasopressin: adjunct in refractory hypotension",
"Ephedrine for hypotension with bradycardia",
"Dopamine/noradrenaline: if haemodynamic collapse",
"Inotropes (dobutamine/adrenaline) if cardiac dysfunction",
"Have vasopressors drawn up before insufflation",
], C.white, C.red);
footer(s);
}
// ═══════════════════════════════════════════════════════════════
// SLIDE 9 — COMPLICATIONS
// ═══════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
bg(s, C.offWhite);
headerBar(s, "Intraoperative & Postoperative Complications", "Recognition and management of life-threatening events");
sectionPill(s, 0.35, 1.22, "⚠ Intraoperative Complications", C.red);
const compLeft = [
{title:"Venous Gas Embolism (VGE)", color:C.red, y:1.68, h:1.85, items:[
"CO₂ enters venous system via open vessel during insufflation",
"Signs: ↓ ETCO₂ (large embolus), 'mill-wheel' murmur, ↓ SpO₂, cardiovascular collapse",
"Management: desufflate immediately, left lateral Trendelenburg, 100% O₂, aspirate via CVP line, CPR if arrest",
]},
{title:"Major Vascular Injury", color:C.red, y:3.62, h:1.5, items:[
"Trocar/Veress needle injury — rare (~0.5%) but high mortality",
"Sudden haemodynamic collapse, distended abdomen, visible haematoma",
"Immediate conversion to open; call for help; blood products",
]},
];
compLeft.forEach(c => card(s, 0.35, c.y, 5.9, c.h, c.title, c.items, C.white, c.color));
const compRight = [
{title:"Haemodynamic Instability", color:C.orange, y:1.68, h:1.85, items:[
"Hypotension: reduce IAP, fluid bolus, vasopressor",
"Hypertension: deepen anaesthesia, antihypertensives",
"Dysrhythmias: hypercarbia correction, atropine for bradycardia",
"Severe hypotension = consider desufflation + open conversion",
]},
{title:"Airway Emergencies", color:C.orange, y:3.62, h:1.5, items:[
"ETT migration into bronchus → reconfirm position",
"↑ Airway pressure → check tube, bronchospasm, pneumothorax",
"Tension pneumothorax: immediate chest decompression",
]},
];
compRight.forEach(c => card(s, 6.55, c.y, 6.4, c.h, c.title, c.items, C.white, c.color));
sectionPill(s, 0.35, 5.25, "Postoperative Complications", C.tealDk);
const postops = [
{title:"Respiratory Dysfunction", items:["Atelectasis, pneumonia","Residual diaphragmatic splinting","SpO₂ monitoring in recovery","O₂ supplementation as needed"], color:C.teal},
{title:"PONV", items:["Very common — TIVA + multimodal antiemetics","Ondansetron + dexamethasone + droperidol","Avoid N₂O; minimise opioids","Adequate hydration"], color:C.purple},
{title:"Shoulder-Tip Pain", items:["Referred pain from residual CO₂ irritating diaphragm","NSAIDs + paracetamol effective","Explain to patient pre-operatively","Resolves within 24–48h"], color:C.orange},
{title:"DVT / VTE", items:["↑ Risk from femoral vein stasis","TED stockings + LMWH","Early mobilisation","Hydration"], color:C.red},
];
const pcW = 2.9;
postops.forEach((c, i) => card(s, 0.35 + i*(pcW+0.22), 5.7, pcW, 1.57, c.title, c.items, C.white, c.color));
footer(s);
}
// ═══════════════════════════════════════════════════════════════
// SLIDE 10 — PAIN & PONV / ERAS / SPECIAL GROUPS
// ═══════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
bg(s, C.offWhite);
headerBar(s, "Postoperative Pain, PONV & Special Considerations", "Multimodal analgesia + ERAS protocols + high-risk populations");
sectionPill(s, 0.35, 1.22, "Postoperative Analgesia (Multimodal — Opioid-Sparing)", C.tealDk);
card(s, 0.35, 1.68, 5.9, 2.3, "Multimodal Analgesia Protocol", [
"Regular paracetamol 1g QDS — baseline",
"NSAIDs (ibuprofen/diclofenac/ketorolac) — add unless contraindicated",
"Wound infiltration with LA (bupivacaine/levobupivacaine) at port sites",
"TAP block (Transversus Abdominis Plane) for larger laparoscopic incisions",
"Intraperitoneal LA instillation (controversial but low risk)",
"Low-dose IV ketamine infusion (0.1–0.3 mg/kg/hr) — reduces opioid requirement",
"Minimise systemic opioids — ↑ PONV, ileus, respiratory depression",
"Remifentanil infusion intraoperatively (ultra-short acting)",
], C.white, C.teal);
card(s, 6.55, 1.68, 6.4, 2.3, "PONV Prevention (APFEL Score-Based)", [
"APFEL risk factors: female sex, non-smoker, Hx motion sickness, opioid use",
"≥2 risk factors → dual/triple prophylaxis",
"Ondansetron 4 mg IV at end of surgery",
"Dexamethasone 4–8 mg IV at induction (potent antiemetic + analgesic)",
"Droperidol 0.625–1.25 mg IV",
"Scopolamine transdermal patch for high risk",
"TIVA (propofol) — significantly ↓ PONV vs. volatile agents",
"Minimise opioids; use regional where possible",
], C.white, C.purple);
sectionPill(s, 0.35, 4.12, "Special Considerations", C.tealDk);
card(s, 0.35, 4.58, 3.85, 2.25, "Ambulatory Laparoscopy", [
"Short-acting agents: propofol TIVA, desflurane",
"Multimodal analgesia — avoid opioid-heavy regimens",
"Strict PONV prophylaxis before discharge",
"Discharge criteria: Aldrete score ≥9, VAS pain ≤4",
"Instructions re: CO₂ shoulder-tip pain",
], C.white, C.teal);
card(s, 4.4, 4.58, 4.15, 2.25, "Robotic-Assisted Laparoscopy", [
"Prolonged steep Trendelenburg = ↑ physiological derangement",
"Limited patient access during robotic surgery — EMERGENCY PLAN essential",
"Airway oedema post-long Trendelenburg — consider extubation in theatre",
"Cerebral oedema, ↑ IOP — limit duration where possible",
"Pre-agree undocking protocol for emergencies",
], C.white, C.orange);
card(s, 8.75, 4.58, 4.2, 2.25, "Obese Patients (BMI >40)", [
"↑ Risk of hypoxaemia, atelectasis, difficult airway",
"Ramped position for induction (ear–sternal notch alignment)",
"RSI routine — aspiration risk ↑",
"Pressure-controlled ventilation preferred",
"PEEP 10+ cmH₂O may be needed",
"BMI >40 + comorbidities → ↑ laparoscopic complications",
"Reverse Trendelenburg for upper abdominal work",
], C.white, C.red);
footer(s);
}
// ═══════════════════════════════════════════════════════════════
// SLIDE 11 — SUMMARY TABLE
// ═══════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
bg(s, C.navy);
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:13.3, h:0.9, fill:{color:C.tealDk}, line:{color:C.tealDk} });
s.addText("Summary: Physiologic Effects of CO₂ Pneumoperitoneum — At a Glance", {
x:0.3, y:0.07, w:12.7, h:0.76, fontSize:16, bold:true, color:C.white, valign:"middle",
});
const rows = [
["System","Effect","Clinical Implication","Management Strategy"],
["Cardiovascular","↑ SVR, ↑ MAP, ↓ venous return (IVC compression), dysrhythmias","↓ Cardiac output; ischaemia in at-risk patients","Limit IAP ≤15 mmHg; vasopressors available; A-line in high-risk"],
["Respiratory","↓ FRC/VC, ↓ compliance, ↑ peak airway pressure, hypercarbia","Atelectasis, V/Q mismatch, respiratory acidosis, ETT migration","↑ Minute ventilation, PEEP 5–8, TV 6–8 mL/kg, lung-protective"],
["Renal","↓ RBF, ↓ GFR, ↑ vasopressin, renin–angiotensin activation","Oliguria; AKI risk especially IAP >15 mmHg","Hydration, limit IAP, avoid nephrotoxins"],
["Splanchnic","↓ Hepatic and intestinal flow (compression)","Bowel ischaemia risk in prolonged cases; ↓ drug clearance","Minimise IAP; avoid excessive Trendelenburg duration"],
["CNS","↑ ICP, ↑ CBF (Trendelenburg + hypercarbia)","Cerebral oedema; risk in cerebrovascular disease","Avoid prolonged steep Trendelenburg; normocapnia"],
["Ocular","↑ IOP (Trendelenburg + hypercarbia)","Rare: ischaemic optic neuropathy, postoperative blindness","Normocapnia; limit Trendelenburg time; ophthalmology if visual Sx"],
["Endocrine","Renin–angiotensin activation, vasopressin release","Fluid/electrolyte disturbance; oliguria","Monitor urine output; goal-directed fluid therapy"],
["Temperature","Heat loss from CO₂ gas","Hypothermia → ↑ coagulopathy, PONV, infection","Active warming, heated CO₂ where available"],
];
const colW = [1.6, 3.2, 3.85, 4.25];
const colX = [0.2, 1.8, 5.0, 8.85];
const rowH = 0.58;
const startY = 1.05;
rows.forEach((row, ri) => {
const isH = ri === 0;
const fill = isH ? C.teal : (ri % 2 === 0 ? "112340" : "0D1F3C");
row.forEach((cell, ci) => {
s.addShape(pres.ShapeType.rect, { x:colX[ci], y:startY+ri*rowH, w:colW[ci], h:rowH, fill:{color:fill}, line:{color:"1A3A5C", width:0.4} });
s.addText(cell, { x:colX[ci]+0.06, y:startY+ri*rowH, w:colW[ci]-0.1, h:rowH, fontSize:isH?9.5:8.2, bold:isH, color:isH?C.white:C.offWhite, valign:"middle", align:"left", margin:2 });
});
});
s.addText("⚠ Severe hypotension during pneumoperitoneum: DESUFFLATE immediately. Consider open conversion. | CO₂ gas embolism: left lateral Trendelenburg + 100% O₂ + aspirate CVP.", {
x:0.2, y:6.3, w:12.9, h:0.38, fontSize:9, bold:true, color:C.amberLt, align:"center",
});
footer(s, "Source: Barash, Cullen & Stoelting's Clinical Anesthesia 9e (Ch.44) | Miller's Anesthesia 10e (Ch.50) | Bailey & Love's Surgery 28e");
}
// ─── Write file ───────────────────────────────────────────────
const outPath = "/home/daytona/workspace/laparoscopic-anaesthesia-ppt/Anaesthetic_Management_Laparoscopic_Surgery.pptx";
pres.writeFile({ fileName: outPath })
.then(() => console.log("SUCCESS: " + outPath))
.catch(err => { console.error("ERROR:", err); process.exit(1); });
cd /home/daytona/workspace/laparoscopic-anaesthesia-ppt && node build.js 2>&1
ls -lh /home/daytona/workspace/laparoscopic-anaesthesia-ppt/Anaesthetic_Management_Laparoscopic_Surgery.pptx
Anaesthetic Management Laparoscopic Surgery
Presentation · PPTX
What's inside — 11 slides
| Slide | Topic |
|---|---|
| 1 | Title slide with topic overview pills |
| 2 | Overview — advantages vs. open surgery, how pneumoperitoneum works, why CO₂ is used, patient positions |
| 3 | Cardiovascular physiology — SVR, MAP, cardiac output, IAP effects, hypercarbia-related dysrhythmias, clinical pearls |
| 4 | Respiratory physiology — ↓FRC, ↓compliance, ETT migration risk, CO₂ absorption, ventilatory strategy with PEEP targets |
| 5 | Regional perfusion & CNS/ocular effects — renal AKI risk, splanchnic flow, IVC stasis/DVT, ICP, intraocular pressure, risk of postoperative blindness |
| 6 | Preoperative assessment — cardiovascular, respiratory, airway, high-risk groups (obesity, elderly), preparation checklist |
| 7 | Intraoperative management — induction, TIVA vs. volatile, muscle relaxation (deep NMB), mandatory vs. situational monitoring |
| 8 | Mechanical ventilation + fluid management — lung-protective parameters, CO₂ management, warming, vasopressor guide |
| 9 | Complications — VGE (gas embolism), major vascular injury, haemodynamic instability, airway emergencies, postoperative VTE, shoulder-tip pain, PONV |
| 10 | Pain management, PONV (APFEL score), ambulatory cases, robotic surgery, obese patients |
| 11 | Master summary table — all 8 organ systems, effects, clinical implications, and management strategies |
anaesthetic management in laproscopic surgery
Anaesthetic Management in Laparoscopic Surgery
1. Key Principle
2. Pneumoperitoneum — The Core Challenge
Why CO₂?
- Highly soluble in blood - rapidly cleared by the lungs even if accidentally injected intravascularly
- Non-flammable and non-oxidising - safe with electrocautery
- Rapidly metabolised and excreted
3. Physiologic Effects (The Anaesthetic Core Knowledge)
A. Cardiovascular Effects
| Parameter | Effect | Mechanism |
|---|---|---|
| SVR | ↑↑ | Catecholamine release, IAP-mediated vasoconstriction |
| MAP | ↑ | ↑ SVR |
| Cardiac Output | ↓ (at high IAP) | IVC compression → ↓ venous return → ↓ cardiac filling |
| Renal/Splanchnic flow | ↓ | Direct visceral compression + vasoconstriction |
| Femoral venous flow | ↓ | IVC/femoral compression → DVT risk |
| Myocardial O₂ demand | ↑ | ↑ afterload (SVR) + ↑ heart rate |
"Severe hypotension during pneumoperitoneum should be treated with desufflation and may require conversion to an open procedure." - Barash Clinical Anesthesia 9e
B. Respiratory Effects
| Parameter | Effect | Clinical Consequence |
|---|---|---|
| FRC / Vital Capacity | ↓↓ | Diaphragm displaced cephalad by IAP |
| Pulmonary compliance | ↓ | ↑ Peak airway pressure needed |
| V/Q mismatch | ↑ | Hypoxaemia - worsened by obesity |
| ETCO₂ / PaCO₂ | ↑ | CO₂ absorbed from peritoneum |
| ETT position | Risk of migration | Diaphragm displacement advances ETT → right main bronchus |
C. Regional Perfusion Effects
- Renal: ↓ RBF, ↓ GFR, ↑ vasopressin, renin-angiotensin activation → oliguria. IAP >15 mmHg associated with postoperative AKI
- Splanchnic/Hepatic: ↓ intestinal and hepatic flow from compression. Bowel ischaemia risk in prolonged cases
- CNS: ↑ ICP and ↑ cerebral blood flow from Trendelenburg + hypercarbia. Extreme caution in patients with cerebrovascular disease
- Ocular: ↑ IOP in steep Trendelenburg - rare risk of postoperative ischaemic optic neuropathy/blindness
4. Preoperative Assessment
Cardiovascular
- History of IHD, heart failure, valvular disease → cardiology review
- Uncontrolled hypertension → optimise before elective surgery
- Poor LV function: pneumoperitoneum may not be tolerated - consider open approach
- ECG, ECHO as indicated. Arterial line for high-risk patients
Respiratory
- Severe COPD/asthma: may not tolerate CO₂ retention and increased airway pressures
- Obesity (BMI >40): highest risk group - difficult airway + hypoxaemia + atelectasis + ↑ complications
- Pulmonary hypertension: elevated IAP may critically reduce RV output
- OSA: CPAP continuation; post-op monitoring essential
Airway
- Obesity and anatomical factors → full airway assessment (Mallampati, thyromental distance, neck mobility)
- RSI for high aspiration risk (obese, hiatus hernia, full stomach)
- Consider awake fibreoptic bronchoscopy if predicted difficult airway
Patient Preparation
- NBM: solids 6h, clear fluids 2h (ERAS)
- DVT prophylaxis: TED stockings + LMWH
- Pre-oxygenation: 3 min tidal breathing or 8 vital capacity breaths
- Antacid premedication where indicated
- Inform patient about shoulder-tip pain from diaphragmatic CO₂ irritation
5. Intraoperative Anaesthetic Management
Induction
- Standard IV induction: propofol + fentanyl/remifentanil
- RSI (suxamethonium or high-dose rocuronium) for aspiration risk
- Cuffed ETT mandatory for pneumoperitoneum cases
- Confirm position - bilateral air entry - recheck after insufflation and positioning
Maintenance
- TIVA (propofol infusion) preferred over volatile agents - significantly reduces PONV, avoids N₂O
- Avoid N₂O - causes bowel distension and worsens PONV
- Remifentanil infusion for intraoperative analgesia
- Sevoflurane acceptable where TIVA not available
Muscle Relaxation - Critical for Laparoscopy
- Improves surgical access and visualisation
- Allows lower insufflation pressures → less physiological derangement
- Monitor with TOF (train-of-four) or PTC (post-tetanic count)
- Reverse fully before extubation - sugammadex preferred for rocuronium reversal
- NMB assessment can be highly subjective - always use nerve stimulator
Monitoring — Mandatory
| Monitor | Purpose |
|---|---|
| ECG | Dysrhythmias from hypercarbia, vagal stimulation |
| ETCO₂ (capnography) | Essential - CO₂ absorption monitoring; gas embolism detection |
| SpO₂ | Hypoxaemia detection |
| NIBP (or A-line) | Haemodynamic instability |
| Airway pressure | ETT migration, bronchospasm, pneumothorax |
| Temperature | Heat loss from CO₂ gas |
| Urine output | Renal perfusion surrogate |
6. Mechanical Ventilation Strategy
| Parameter | Target |
|---|---|
| Tidal Volume | 6-8 mL/kg Ideal Body Weight |
| PEEP | 5-8 cmH₂O (up to 10+ in obese patients) |
| Respiratory Rate | Adjusted to maintain ETCO₂ 35-45 mmHg |
| FiO₂ | Minimum to maintain SpO₂ >95% |
| Peak airway pressure | Target <30 cmH₂O |
| Mode | Pressure-controlled preferred in obese patients |
- Increase minute ventilation after insufflation to compensate for CO₂ absorption
- Sudden ETCO₂ spike → suspect subcutaneous emphysema or gas embolism
- Recruitment manoeuvres (30-40 cmH₂O for 30s) for refractory hypoxaemia
- At end of procedure: hand ventilate to expel residual peritoneal CO₂
7. Fluid Management & Temperature
- Goal-directed fluid therapy (GDFT) based on dynamic flow parameters
- Avoid over-hydration - worsens airway oedema (critical in prolonged Trendelenburg)
- Target urine output >0.5 mL/kg/hr (>2 mL/kg/hr reassuring)
- No evidence for furosemide, mannitol, or "renal-dose" dopamine in AKI prevention
- Active patient warming mandatory - CO₂ gas causes significant heat loss
- Forced-air warming blanket
- Warm IV fluids and blood products
- Heated and humidified CO₂ insufflation where available
- Target normothermia 36-37.5°C
8. Complications — Recognition and Management
Intraoperative
- CO₂ enters venous system via open vessel during insufflation
- Signs: sudden ↓ ETCO₂ (large embolus), "mill-wheel" murmur, ↓ SpO₂, cardiovascular collapse
- Management: desufflate immediately, left lateral Trendelenburg, 100% O₂, aspirate via CVP line, CPR if arrest
- Trocar or Veress needle injury - rare (~0.5%) but high mortality
- Sudden haemodynamic collapse, distending abdomen
- Immediate call for help, open conversion, blood products
- Hypotension: reduce IAP, fluid bolus, vasopressor (phenylephrine, vasopressin, ephedrine)
- Hypertension: deepen anaesthesia, antihypertensives
- Dysrhythmias: correct hypercarbia; atropine for bradycardia (vagal from peritoneal stretch)
- ETT migration into right main bronchus → reconfirm position after any position change
- ↑ Airway pressure → check tube, consider bronchospasm or pneumothorax
- Tension pneumothorax: immediate needle decompression
- CO₂ tracking into subcutaneous tissue
- Manifests as crepitus, ↑ ETCO₂ unresponsive to ↑ ventilation
- Reduce IAP; usually resolves spontaneously
Postoperative
| Complication | Management |
|---|---|
| Atelectasis / respiratory dysfunction | SpO₂ monitoring, O₂ supplementation, incentive spirometry |
| PONV | Multimodal antiemetics (ondansetron + dexamethasone + droperidol); TIVA intraoperatively |
| Shoulder-tip pain | Diaphragmatic CO₂ irritation; NSAIDs + paracetamol; warn patient pre-op |
| DVT/VTE | TED stockings + LMWH; early mobilisation |
| AKI | Monitor urine output; hydration; avoid nephrotoxins |
| Airway oedema | After prolonged Trendelenburg - consider delayed extubation in theatre |
9. Postoperative Analgesia — Multimodal (Opioid-Sparing)
- Paracetamol 1g QDS — regular, baseline
- NSAIDs (ketorolac, ibuprofen, diclofenac) — unless contraindicated
- Port-site local anaesthetic infiltration - bupivacaine/levobupivacaine at all incision sites
- TAP block (Transversus Abdominis Plane block) - for larger/more painful laparoscopic procedures
- Low-dose IV ketamine (0.1-0.3 mg/kg/hr) - reduces opioid consumption
- Intraperitoneal LA instillation - low risk, some evidence for benefit
- Minimise systemic opioids - drives PONV, ileus, respiratory depression
10. PONV Prevention (APFEL Score)
- Female sex
- Non-smoker
- History of motion sickness or previous PONV
- Postoperative opioid use
- Ondansetron 4 mg IV at end of surgery
- Dexamethasone 4-8 mg IV at induction
- Droperidol 0.625-1.25 mg IV
- Scopolamine patch for high-risk
- TIVA (propofol) significantly reduces baseline PONV risk vs. volatiles
11. Special Groups
Obese Patients (BMI >40)
- Ramped position at induction (ear-sternal notch alignment)
- RSI routine - aspiration risk
- Pressure-controlled ventilation preferred
- Higher PEEP (up to 10-12 cmH₂O)
- Reverse Trendelenburg for upper abdominal surgery (improves FRC)
- BMI >40 + comorbidities = significantly ↑ laparoscopic complications
Robotic-Assisted Laparoscopy
- Prolonged steep Trendelenburg = magnified physiological derangement
- Limited patient access during surgery - pre-agree emergency undocking protocol with surgeon
- Risk of airway oedema and cerebral oedema - consider extubation in theatre
- Postoperative visual loss risk - limit total steep Trendelenburg duration
Ambulatory Laparoscopy
- Short-acting agents: propofol TIVA, desflurane
- Multimodal analgesia to avoid opioid-heavy regimens
- Strict PONV prophylaxis before discharge
- Aldrete score ≥9 + VAS pain ≤4 for discharge criteria
Quick Reference Summary
| Issue | Key Action |
|---|---|
| Desufflation threshold | Severe hypotension → desufflate immediately |
| Max IAP | ≤15 mmHg; target 12 mmHg in high-risk |
| ETT migration check | After insufflation AND after every position change |
| ETCO₂ target | 35-45 mmHg; increase MV after insufflation |
| Best anaesthetic agent | TIVA (propofol) - ↓ PONV, avoids N₂O |
| NMB reversal | Sugammadex (full reversal mandatory) |
| Gas embolism | Desufflate + left lateral Trendelenburg + 100% O₂ |
| PONV prevention | Ondansetron + dexamethasone + TIVA |
If you want the PowerPoint version I generated earlier, you can download it here:Anaesthetic Management Laparoscopic Surgery
Presentation · PPTX