Ivdp and L2-L5- posterior spinal decompression and intrumental fusion steps
Reading File
Finding Sources
Finding Sources
Searching the Web
IVDP L2-L5 posterior spinal decompression instrumented fusion surgical steps technique
Finding Sources
Finding Sources
Reading Web Page
https://www.spinecareofny.com/spine-treatments/fusion-surger…
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
The library FTS isn't matching those specific phrases. I have enough from Campbell's and clinical knowledge to provide a thorough, accurate answer. Let me compile the complete response now.
IVDP (Intervertebral Disc Prolapse) at L2-L5: Posterior Spinal Decompression and Instrumented Fusion
Overview
This is a combined procedure addressing multi-level disc prolapse (L2-3, L3-4, L4-5) with neural compression. The goals are:
- Decompression - relieve pressure on the spinal cord/cauda equina and nerve roots
- Instrumented fusion - stabilize the destabilized segments after decompression
Pre-Operative Planning
- Full-length standing X-rays (AP + lateral); flexion-extension views to assess instability
- MRI lumbar spine: confirm levels of disc prolapse, canal stenosis, foraminal narrowing
- CT lumbar spine: assess pedicle morphology for screw sizing (diameter and length)
- Neuromonitoring plan: SSEP/MEP/EMG
- Blood cross-match; DVT prophylaxis plan
- Bowel prep if needed; urinary catheter placement
Patient Positioning
- General anesthesia, endotracheal intubation
- Prone position on a Wilson frame or Jackson table (allows lumbar flexion - opens laminar spaces)
- Abdomen must hang free (reduces epidural venous engorgement and bleeding)
- Chest rolls placed below shoulders and ASIS bilaterally
- Arms padded and placed at 90° abduction or alongside body
- Eyes, face, genitals, bony prominences well-padded and checked
- Fluoroscopy or O-arm/navigation system positioned and draped
Surgical Steps
Step 1 - Skin Incision and Exposure
- Midline posterior incision from one level above L2 to one level below L5 (approx. L1-S1 spinous processes)
- Incise subcutaneous tissue and thoracolumbar fascia in the midline
- Subperiosteal dissection - elevate erector spinae muscles bilaterally off the spinous processes and laminae using Cobb elevator and electrocautery
- Expose laminae, facet joints, and transverse processes from L2 to L5 (transverse processes needed for posterolateral fusion graft bed)
- Pack with gauze swabs; control bleeding with bipolar cautery and bone wax at bleeding bone edges
- Place self-retaining retractors (e.g., Williams or Gelpi retractors)
Step 2 - Intraoperative Level Confirmation
- Lateral fluoroscopic image (C-arm) or O-arm scan to confirm L2-L5 levels
- Mark spinous processes or use spinal needle in disc space
Step 3 - Pedicle Screw Insertion (Instrumentation)
Screws placed at L2, L3, L4, L5 bilaterally (8 screws total) - typically done before decompression to maintain structural reference points.
Technique (Freehand or Fluoroscopy/Navigation-guided):
- Entry point: Junction of the transverse process and lateral border of the superior articular process (Weinstein's entry point at lumbar levels)
- Remove cortical bone at entry point with a high-speed burr or rongeur
- Use a pedicle probe/awl to create a channel through the pedicle into the vertebral body - angled slightly medially (5-10° for L2-L4, ~10-15° medial at L5) and in the sagittal plane following the pedicle axis
- Probe the 4 walls and floor of the track with a ball-tip feeler to confirm intact cortex (no breach)
- Tap the pedicle if using cortical or large screws
- Insert polyaxial pedicle screws of appropriate size (typically 5.5-6.5 mm diameter, 40-50 mm length in lumbar spine)
- Confirm position with AP and lateral fluoroscopy or triggered EMG (threshold >8 mA = intact pedicle wall)
Step 4 - Decompression (Laminectomy/Laminotomy)
Performed at each symptomatic level (L2-3, L3-4, L4-5):
A. Midline Decompression (Central Canal)
- Spinous process resection - nibble spinous processes at affected levels with rongeur or osteotome
- Laminectomy - use Kerrison rongeurs and/or high-speed drill to remove the lamina bilaterally, working from caudal to cranial margin of each lamina
- Identify yellow ligament (ligamentum flavum); excise with Kerrison punch working laterally to the medial facet border
- Expose dural sac; confirm decompression by gentle dural pulsation and free movement
B. Lateral Recess and Foraminal Decompression
- Medial facetectomy - remove medial one-third of inferior and superior facets with Kerrison or burr to decompress lateral recess
- Undercutting of facets laterally to expose the nerve root in the foramen
- Probe the foramen with a nerve hook to confirm root is free
Step 5 - Discectomy (at each IVDP level)
- Identify the affected disc space after retracting the dural sac medially with a nerve root retractor
- Incise the posterior annulus with a #15 blade or annulotomy knife
- Remove disc material with pituitary rongeurs (straight and angled) and curettes
- Clear the disc space of nuclear material - work anteriorly carefully to avoid anterior great vessel injury
- Prepare the endplates with curettes and shavers (for interbody fusion if PLIF/TLIF planned)
Step 6 - Interbody Fusion (PLIF Technique, if performed)
- Distract the disc space using a distractor between pedicle screws
- Prepare the disc space endplates until bleeding bone exposed
- Pack one side with autologous bone graft (from local laminectomy bone); insert interbody cage (PEEK or titanium, filled with bone graft) on one or both sides
- Alternatively, TLIF approach (unilateral transforaminal route) minimizes nerve root retraction and is preferred for multi-level cases
Step 7 - Posterolateral Fusion Bed Preparation
- Decorticate the transverse processes at L2, L3, L4, L5 bilaterally with a high-speed burr until cancellous bone is exposed
- Decorticate the facet joints (after any facetectomy has been done)
- Lay down autologous bone graft (from local laminectomy bone + iliac crest graft if needed) or bone graft substitutes (allograft, DBM, BMP-2 with appropriate indications) across the transverse processes bilaterally
Step 8 - Rod Placement and Compression/Distraction
- Measure rod length to span L2-L5 bilaterally
- Contour titanium or cobalt-chrome rods to match the lumbar lordosis (approximately 20-40°)
- Insert rods into the screw heads bilaterally
- Apply compression across levels where lordosis is needed; apply distraction where disc height/foraminal height needs to be restored
- Tighten set screws to final torque (usually ~8 Nm)
- Place crosslinks if needed for rotational stability (typically one crosslink per construct)
Step 9 - Final Check
- Final fluoroscopy (AP + lateral): confirm screw positions, rod placement, overall alignment, and appropriate lumbar lordosis
- Palpate/probe each screw head for toggling (suggests loosening)
- Re-inspect neural elements: dural sac pulsating freely, all nerve roots decompressed
- Triggered EMG confirmation of all screw levels
Step 10 - Wound Closure
- Thorough irrigation with normal saline (3-6 litres, antibiotic-added per surgeon preference)
- Place epidural fat graft (from local fat) or absorbable haemostat over exposed dura to prevent adhesions
- Place closed suction drain (one or two drains) deep to fascia
- Close thoracolumbar fascia in layers with No. 1 PDS or Vicryl
- Approximate subcutaneous tissue with 2-0 Vicryl
- Skin closure with staples or 2-0 nylon interrupted sutures or subcuticular monocryl
Immediate Post-Operative Care
| Parameter | Details |
|---|---|
| Monitoring | ICU/HDU; neuro checks every 1-2 hrs |
| Drain | Remove at 24-48 hrs when output <50 ml/shift |
| Mobilization | Sit up on day 1; stand/walk with physio on day 2 with LSO brace |
| DVT prophylaxis | LMWH from day 1; compression stockings |
| Antibiotics | IV for 24-48 hrs (Cefazolin or equivalent) |
| Imaging | Post-op X-ray AP+lateral before discharge |
| Discharge | Day 3-5 for uncomplicated cases |
Potential Complications
| Intra-operative | Post-operative |
|---|---|
| Dural tear / CSF leak | Wound infection / epidural abscess |
| Nerve root injury | Radiculopathy (new or persistent) |
| Pedicle screw malposition | Hardware failure / screw breakage |
| Vascular injury (anterior) | Adjacent segment disease |
| Excessive blood loss | Pseudarthrosis (failed fusion) |
| Flatback deformity if lordosis not restored |
Key Technical Points for L2-L5 Multi-level Cases
- Preserve at least one facet joint complex per level where possible to reduce instability, but complete facetectomy may be needed if severely arthritic or if PLIF is planned
- Always restore lumbar lordosis in the rod contour - failure leads to flatback syndrome and adjacent segment overload
- At L4-5, the iliac crest can partially obstruct rod passage - plan screw trajectory accordingly
- Multi-level PLIF carries higher risk of nerve root retraction injury; TLIF (unilateral transforaminal approach) is often preferred
- Consider iliac crest bone graft for 3-level fusions to supplement local bone, especially in osteoporotic patients
- Neuromonitoring (SSEP + EMG) throughout is strongly recommended for L2-L5 multi-level cases
- Campbell's Operative Orthopaedics 15th Ed 2026, Chapter on Spondylolisthesis & Posterior Lumbar Instrumented Fusion techniques
Scarpas triangle
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have excellent, comprehensive material from three authoritative textbooks plus detailed diagrams. Here is the full answer:
Scarpa's Triangle (Femoral Triangle)
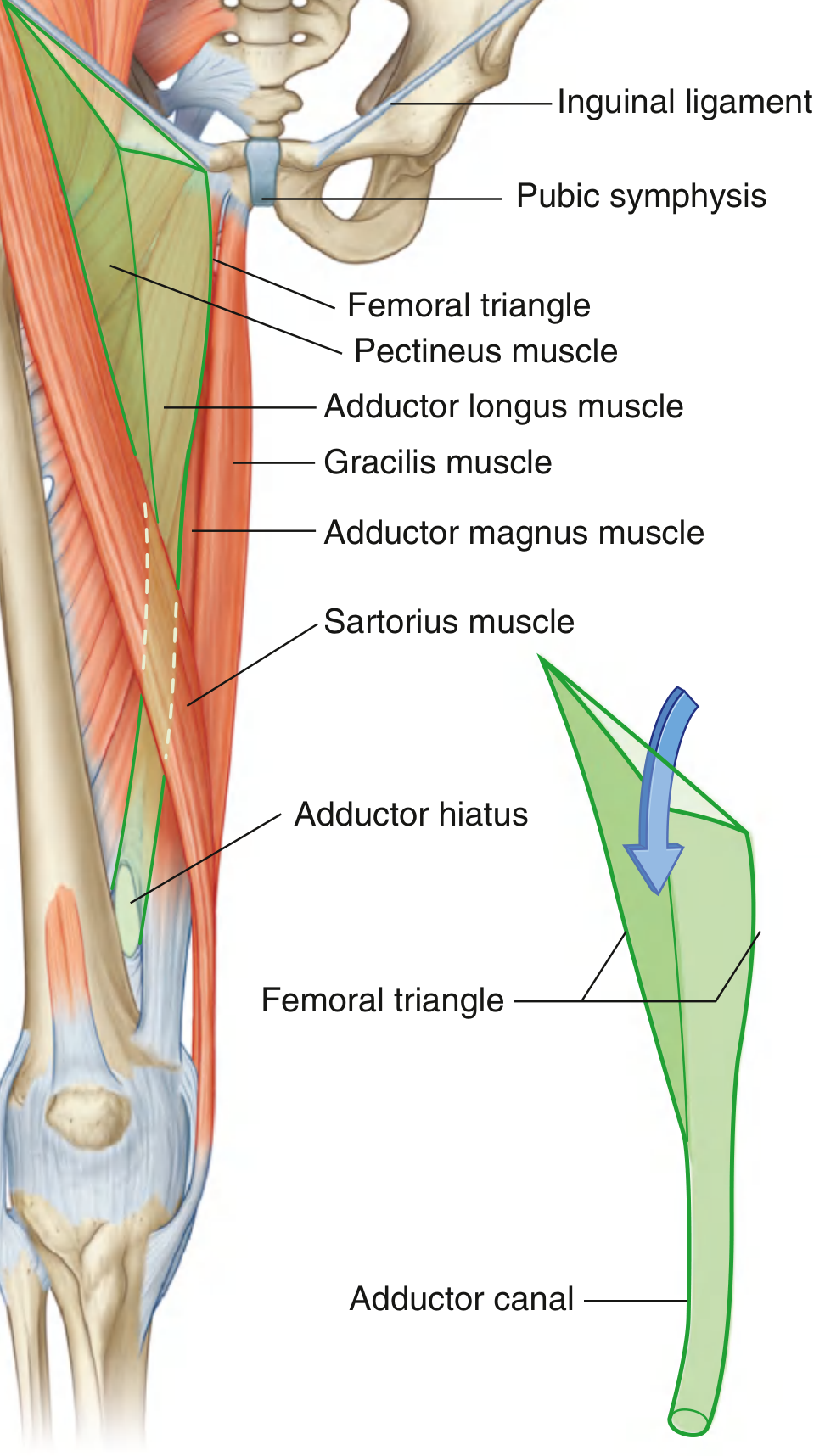
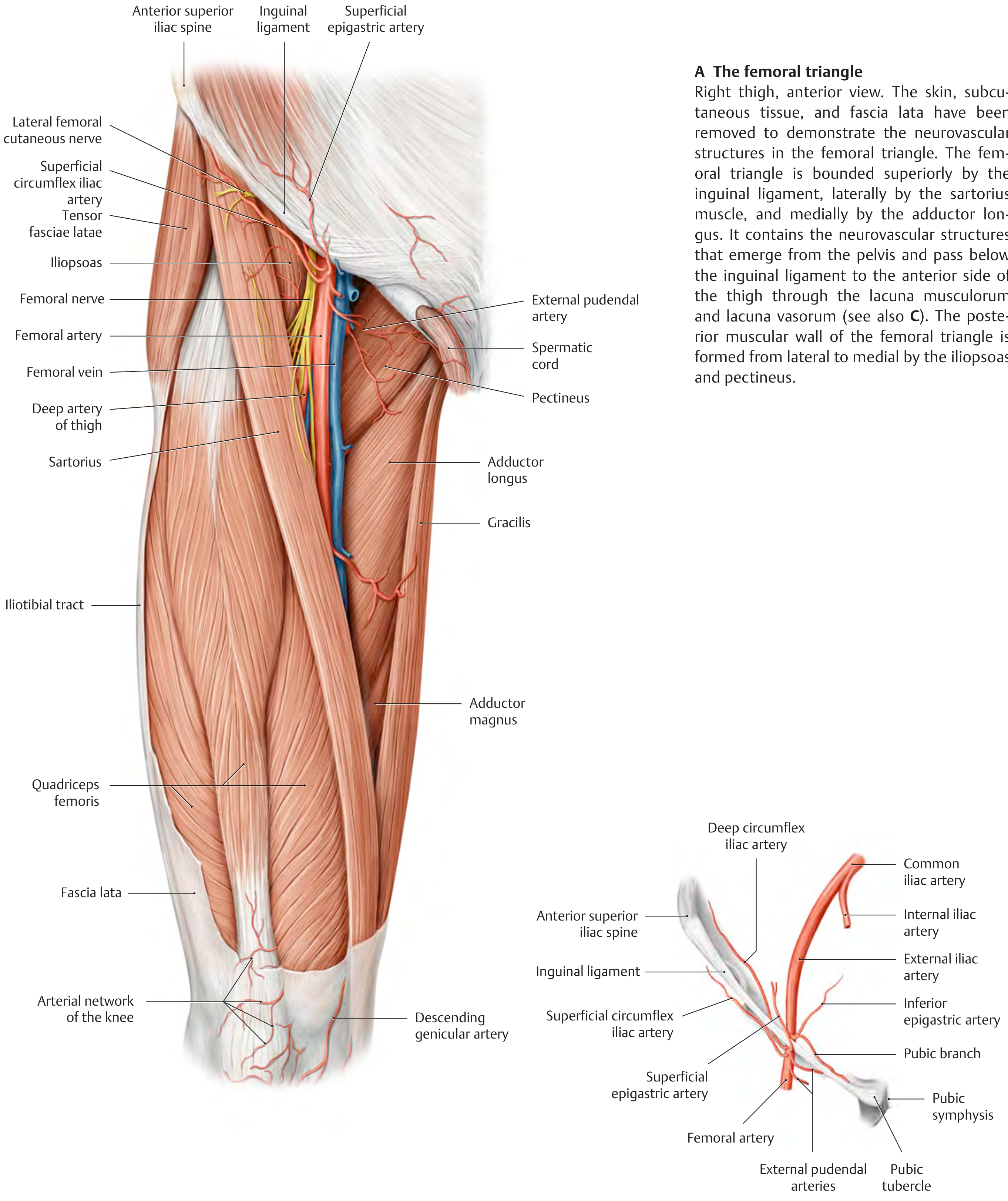
Scarpa's triangle is also known as the femoral triangle - a wedge-shaped depression at the upper anterior thigh, at the junction between the anterior abdominal wall and the lower limb.
Boundaries
| Boundary | Structure |
|---|---|
| Superior (base) | Inguinal ligament (from ASIS to pubic tubercle) |
| Lateral | Medial margin of sartorius muscle |
| Medial | Medial margin of adductor longus muscle |
| Apex | Points inferiorly - where sartorius and adductor longus meet; continues as the adductor canal |
Mnemonic for boundaries: "SAIL" - Sartorius, Adductor longus, Inguinal Ligament
Roof
Formed by:
- Skin and superficial fascia (containing superficial inguinal lymph nodes, great saphenous vein, and cutaneous nerves)
- Fascia lata (deep fascia of thigh)
- The cribriform fascia (perforated part of fascia lata) over the femoral canal area
Floor (from lateral to medial)
| Structure | Position |
|---|---|
| Iliopsoas (iliacus + psoas) | Lateral portion |
| Pectineus | Medial portion |
| Adductor longus | Most medial |
Miller's Review of Orthopaedics: "Floor (lateral to medial): iliacus, psoas, pectineus, adductor longus"
Contents (from lateral to medial)
Mnemonic: "NAVeL" or "NAVY" (lateral → medial)
| Order (Lateral → Medial) | Structure |
|---|---|
| 1 | N - Femoral Nerve (outside femoral sheath) |
| 2 | A - Femoral Artery |
| 3 | V - Femoral Vein |
| 4 | L - Lymphatics (femoral canal - most medial compartment) |
Gray's Anatomy: "From lateral to medial: femoral nerve, femoral artery, femoral vein, and lymphatic vessels"
Femoral Sheath
A funnel-shaped sleeve of fascia enclosing the artery, vein, and lymphatics (NOT the nerve - the femoral nerve lies outside the sheath, lateral to it):
| Compartment | Contents |
|---|---|
| Lateral | Femoral artery |
| Middle | Femoral vein |
| Medial (femoral canal) | Lymphatics + Cloquet's/Rosenmüller node; potential site of femoral hernia |
Surface Anatomy / Clinical Palpation
- Femoral artery pulse is felt just inferior to the inguinal ligament, at the midpoint between ASIS and pubic symphysis (mid-inguinal point)
- Adductor longus tendon is palpable as a cord just below the pubic tubercle
- Sartorius crosses obliquely from ASIS to the medial tibia
Apex and Continuation
The apex of the femoral triangle points inferiorly and is continuous with the adductor canal (Hunter's canal), which:
- Runs down the medial thigh under sartorius
- Passes through the adductor hiatus in adductor magnus
- Becomes the popliteal fossa behind the knee
Key Branches of the Femoral Artery Within the Triangle
| Branch | Origin |
|---|---|
| Superficial epigastric artery | Just below inguinal ligament |
| Superficial circumflex iliac artery | Just below inguinal ligament |
| External pudendal artery | Medially |
| Profunda femoris (deep artery of thigh) | Posterior, ~4 cm below inguinal ligament - largest branch |
Clinical Relevance
| Application | Details |
|---|---|
| Femoral pulse | First site for ABCDE assessment; used for cardiac catheterization, femoral arterial line |
| Femoral hernia | Through femoral ring (medial to femoral vein); more common in women; enters femoral canal |
| Femoral nerve block | Anaesthetic infiltration at the femoral triangle for lower limb surgery |
| Femoral vein cannulation | Emergency IV access; vein lies medial to artery |
| Lymph node dissection | Inguinal/femoral LN clearance for melanoma or penile/vulvar carcinoma |
| THA risk | Retractors placed inferiorly/medially along acetabulum risk femoral nerve injury |
| Femoral pseudoaneurysm | Complication of femoral arterial puncture (catheterization) |
Sources: Gray's Anatomy for Students (p. 675), Thieme Atlas of Anatomy - General Anatomy & Musculoskeletal System (p. 573), Miller's Review of Orthopaedics 9th Ed
This is a shared conversation. Sign in to Orris to start your own chat.