Explain the ABCDE of trauma
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from the textbooks. Let me compile the full answer.
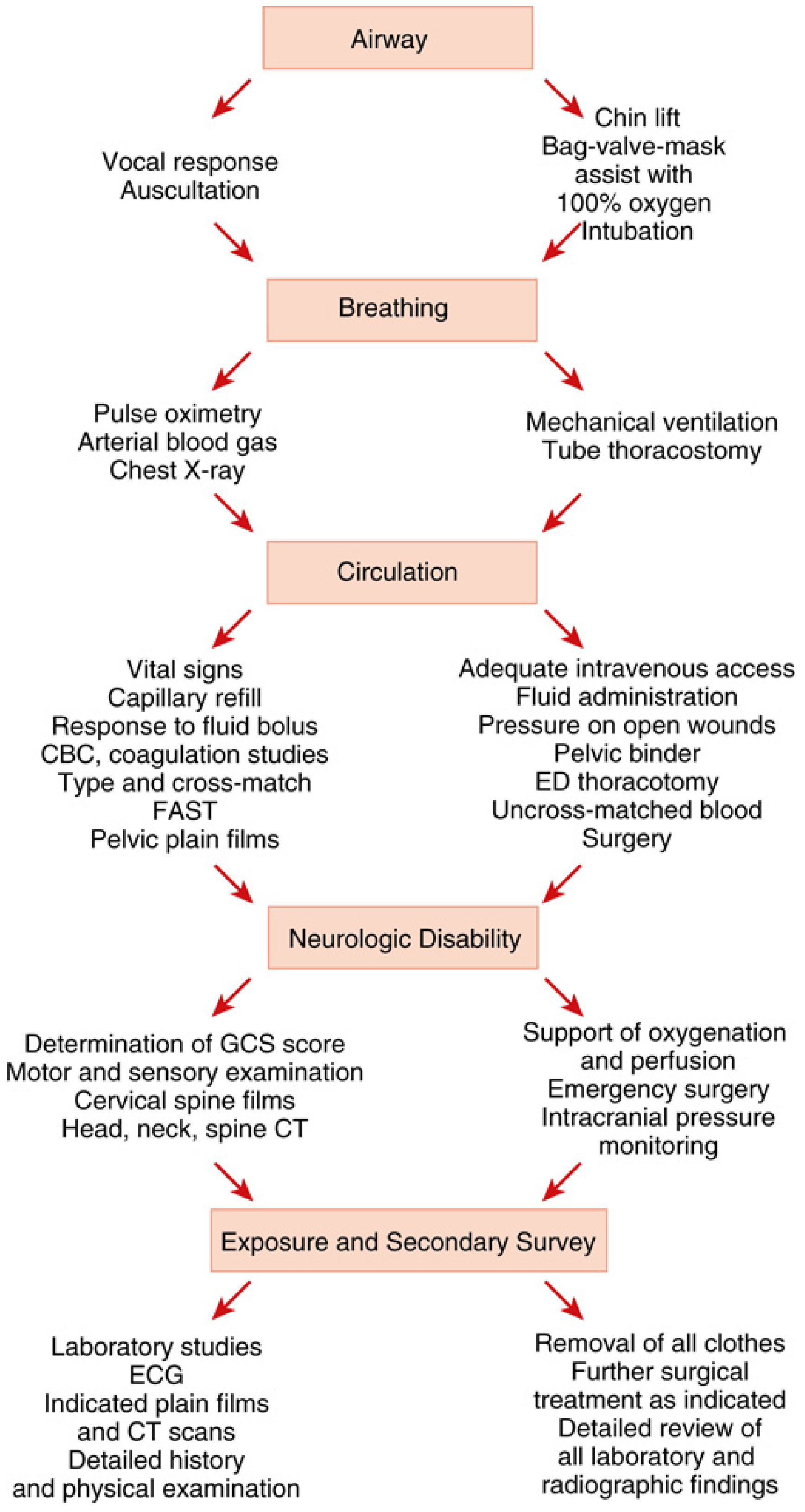
The ABCDE of Trauma - Primary Survey
The ABCDE approach is the systematic framework for the primary survey in trauma, developed by the Advanced Trauma Life Support (ATLS) program of the American College of Surgeons. It prioritizes assessment and treatment of immediately life-threatening conditions in a fixed sequence, ensuring the most lethal problems are addressed first.
The principle is: treat as you find - do not move to the next step until the current threat is managed or excluded.
A - Airway (with Cervical Spine Protection)
Goal: Confirm the airway is open and patent; protect the cervical spine.
Assessment:
- Ask the patient their name and what happened - a clear vocal response confirms the airway is open and gives information about breathing, circulation, and consciousness simultaneously
- Listen for stridor or hoarseness (suggesting partial obstruction or laryngeal injury)
- Inspect for obstruction: blood, vomit, foreign bodies, tongue prolapse, facial/mandibular fractures
- Look for crepitus in the neck, hemoptysis, or cyanosis - these may indicate tracheobronchial injury requiring immediate operative repair
Interventions:
- Suction and clear the oropharynx
- Chin lift / jaw thrust maneuver
- Oropharyngeal or nasopharyngeal airway adjuncts
- Bag-valve-mask ventilation with 100% oxygen
- Definitive airway (intubation) if: GCS <8, combativeness impairing assessment, obtundation from severe shock, or anticipated airway deterioration
- Surgical airway (cricothyroidotomy) if intubation fails
Cervical spine: Apply inline manual immobilization in all blunt trauma until the spine is clinically cleared.
B - Breathing
Goal: Ensure adequate oxygenation and ventilation.
Assessment:
- Observe for symmetric, non-labored chest wall movement
- Auscultate lung fields bilaterally - absent or unequal breath sounds indicate hemothorax or pneumothorax
- Monitor with pulse oximetry; use end-tidal CO2 (EtCO2 target: 35-40 mmHg) if available
- Percussion: hyper-resonance = pneumothorax; dullness = hemothorax
Key diagnoses and immediate treatment:
| Condition | Findings | Treatment |
|---|---|---|
| Tension pneumothorax | Absent breath sounds, hyper-resonance, absent chest rise, hemodynamic collapse | Immediate needle decompression (14G angiocatheter, 4th-5th ICS, anterior midaxillary line), then tube thoracostomy |
| Open ("sucking") pneumothorax | Large chest wall defect (>3 cm), audible air movement | 3-sided occlusive dressing (flutter valve effect), then tube thoracostomy away from wound |
| Hemothorax | Dullness to percussion, decreased breath sounds | Tube thoracostomy; operative if >1,500 mL initial output or >200 mL/hr for ≥4 hours |
| Flail chest | Paradoxical chest wall movement | Analgesia, supplemental O2, positive pressure ventilation if failing |
C - Circulation (with Hemorrhage Control)
Goal: Identify and control hemorrhage; assess for shock.
Assessment:
- Vital signs: blood pressure, heart rate
- Palpate central and peripheral pulses (including distal to any injured extremity)
- Assess skin color, temperature, capillary refill
- Hard signs of vascular trauma: active arterial bleeding, absent pulse in an injured limb, expanding/pulsatile hematoma, bruit or thrill at injury site - these mandate operative intervention or urgent imaging
Interventions:
- Direct compression or tourniquet for external bleeding (note exact time of tourniquet application)
- Pelvic binder for pelvic fracture with hypotension (closes pelvic ring, tamponades retroperitoneal hemorrhage)
- Splint long-bone fractures to reduce hemorrhage (traction splint for mid-shaft femur)
- Large-bore IV access x2; send blood for CBC, coagulation, type and cross-match
- FAST (Focused Assessment with Sonography for Trauma) to detect hemoperitoneum or pericardial effusion
- Blood product resuscitation (balanced transfusion: packed red cells, FFP, platelets in 1:1:1 ratio for massive hemorrhage)
Important caveat: In a patient in extremis from presumed hemorrhagic shock, hemorrhage control may supersede airway evaluation. Resuscitative ED thoracotomy (EDT) or REBOA (Resuscitative Endovascular Balloon Occlusion of the Aorta) may be required for non-compressible hemorrhage.
D - Disability (Neurological Status)
Goal: Rapidly assess the brain and spinal cord.
Assessment:
- AVPU scale (quick screen): Alert / Verbal / Pain / Unresponsive
- Glasgow Coma Scale (GCS): Eyes (1-4) + Verbal (1-5) + Motor (1-6) = total score 3-15
- GCS <8 = severe TBI; intubation is indicated
- Pupillary response: size, symmetry, reaction to light - unequal pupils suggest uncal herniation
- Motor and sensory examination of all four limbs for spinal cord injury
- Blood glucose to rule out hypoglycemia as a reversible cause of altered mental status
Interventions:
- Optimize oxygenation and perfusion to the brain (hypoxia and hypotension are the primary secondary injury mechanisms)
- Emergency neurosurgical consultation for evidence of herniation
- Cervical spine immobilization continues
- Head/neck/spine CT once stabilized
- Intracranial pressure monitoring when indicated
E - Exposure and Environment
Goal: Fully expose the patient to identify all injuries; prevent hypothermia.
Assessment:
- Remove all clothing (cut away if necessary) to perform a complete head-to-toe inspection
- Log roll the patient to examine the back, spine, and buttocks
- Inspect all skin surfaces for wounds, bruising, deformity, or evidence of penetrating injury
- Perineal and rectal examination when indicated
Environment - prevent hypothermia:
- Hypothermia in trauma is part of the "lethal triad" (hypothermia + acidosis + coagulopathy) which dramatically worsens outcomes
- Use warm IV fluids, warming blankets, and warm environment
- Cover the patient as soon as exposure is complete
The "(C)ABCDE" Extension
Modern trauma protocols, particularly in military and pediatric contexts, add a "C" before the A - making it C-ABCDE:
- C = Catastrophic (external) hemorrhage - massive compressible bleeding (e.g., limb amputation, junctional wounds) that will kill faster than an airway problem must be controlled first with tourniquets or wound packing before anything else
After the Primary Survey
Once ABCDE is complete and the patient is stabilized, the secondary survey begins - a systematic head-to-toe physical examination documenting all injuries. The ABCDE survey should be repeated whenever the patient's status changes, as new threats can emerge at any time.
Sources: Fischer's Mastery of Surgery, 8th ed.; Miller's Anesthesia, 10th ed.; Tintinalli's Emergency Medicine - based on ATLS (American College of Surgeons) curriculum.
This is a shared conversation. Sign in to Orris to start your own chat.