Pedia and adult airway compression - MD anaesthesia PG exam answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material from Miller's Anesthesia (10e), Barash (9e), and Morgan & Mikhail (7e). Let me compose a complete PG exam-style answer.
Airway Compression - Pediatric vs Adult: MD Anaesthesia PG Exam Answer
PART 1: ANATOMICAL DIFFERENCES - PEDIATRIC vs ADULT AIRWAY
This is a high-yield topic because the structural differences directly determine how the airway compresses, collapses, and responds to anesthetic maneuvers.
Shape and Narrowest Point
| Feature | Adult | Neonate/Infant |
|---|---|---|
| Laryngeal shape | Cylindrical | Funnel-shaped (narrowed at cricoid) |
| Narrowest point | Vocal cords (glottis) | Cricoid ring (subglottis) |
| Glottic level | C5-C6 | C3 (premature) - C4 (full term) |
| Epiglottis | Flat, supple | Omega/tubular shaped, stiff, bulky aryepiglottic folds |
| Vocal cords | Perpendicular | Anteriorly slanted (harder to visualize + pass tube) |
| Occiput | Normal | Prominent - causes neck flexion when supine |
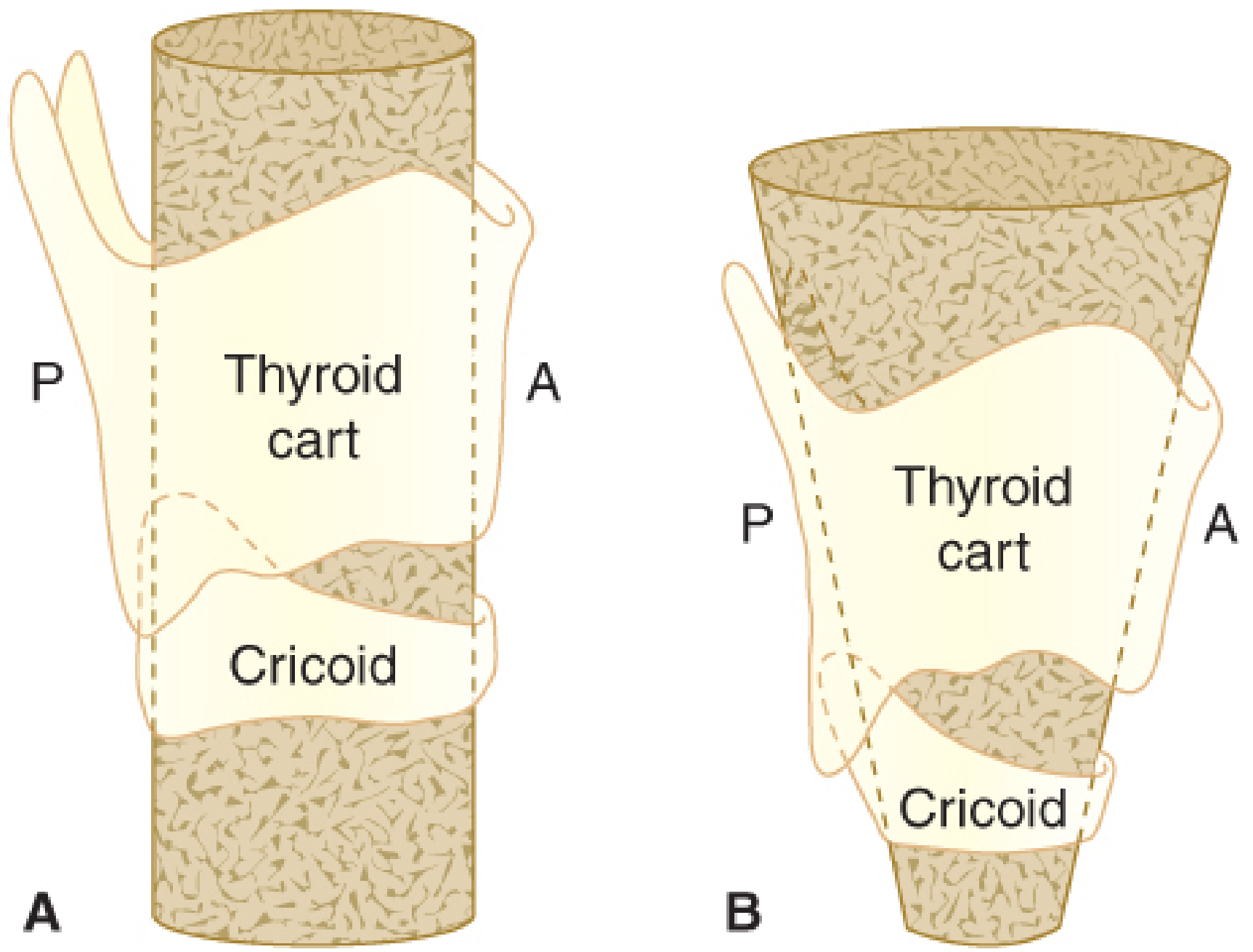
Fig. Adult (A) vs. infant (B) larynx configuration. The adult larynx has a cylindrical shape. The infant larynx is funnel-shaped due to the narrow cricoid ring - this makes the cricoid the functionally smallest cross-section in the pediatric airway. (Barash, Clinical Anesthesia 9e)
Key Implication of Funnel Shape
In the neonate, although the glottic opening may measure smallest anatomically, it is more distensible than the cricoid ring (the first complete cartilaginous ring). Therefore, the cricoid is the functionally narrowest point - an ETT may pass through the glottis easily and then jam at the cricoid. This is why:
- Uncuffed tubes have traditionally been used in neonates (to avoid circumferential mucosal pressure at the cricoid)
- Cuffed, small-volume, high-compliance tubes are increasingly used now, but uncuffed tubes still remain common in neonates
Other Pediatric Airway Peculiarities
- Obligate/preferential nasal breathing - neonates and young infants; any nasal obstruction (bilateral choanal atresia = life-threatening)
- Large tongue - relatively larger in oropharynx; promotes soft-tissue upper airway obstruction and makes direct laryngoscopy harder
- Cephalad larynx - the larynx appears "anterior" but is actually positioned higher (cephalad); the tip of the epiglottis at C1 allows simultaneous suckling and breathing
- Large occiput - causes spontaneous neck flexion when supine; optimal position is neutral with slight extension (may need a roll under shoulders, not head)
- Submandibular soft tissue - must NOT be compressed during mask ventilation, as this pushes the tongue back and obstructs the airway
(Morgan & Mikhail's Clinical Anesthesiology 7e, Chapter 42; Barash Clinical Anesthesia 9e, Chapter 42)
PART 2: AIRWAY COMPRESSION - ANTERIOR MEDIASTINAL MASS
This is the classic high-yield PG question scenario for "airway compression in anesthesia."
Pathophysiology: Why Does GA Make it Worse?
General anesthesia exacerbates extrinsic intrathoracic airway compression through three distinct mechanisms (Miller's Anesthesia 10e, Chapter 49):
- Reduced lung volume - FRC falls under GA; tracheobronchial diameters decrease proportionally with lung volume
- Bronchial smooth muscle relaxation - GA relaxes bronchial smooth muscle, making large airways more compressible
- Loss of spontaneous ventilation/diaphragmatic tone - Neuromuscular blockade eliminates the caudal diaphragmatic movement of spontaneous breathing; this abolishes the normal transpleural pressure gradient that dilates intrathoracic airways during inspiration
Why Are Children at Higher Risk Than Adults?
- More compressible cartilage - the cartilaginous airway structure is more pliable in children
- Inability to report positional symptoms - adults can describe orthopnea or supine cough; young children cannot, so warning signs are missed
- Life-threatening complications can occur even in asymptomatic children with anterior mediastinal masses
Critical Threshold
- CT scan: >50% tracheal or tracheobronchial compression = unsafe for routine general anesthesia in children
- In the absence of this threshold, tracheal cross-sectional area and peak expiratory flow rates at least 50% of predicted have been used as a guide for safer induction
Anesthetic Management of Airway Compression
Preoperative Assessment
- CT chest (most important test): defines location, extent, degree of compression
- Flow-volume loops (upright + supine): variable intrathoracic obstructive pattern (expiratory plateau) when supine
- Transthoracic echocardiography: if vascular compression symptoms present
- Ask specifically: Can the patient lie flat? Supine dyspnea or cough = high risk
- Seek extrathoracic biopsy source first (pleural fluid, supraclavicular node)
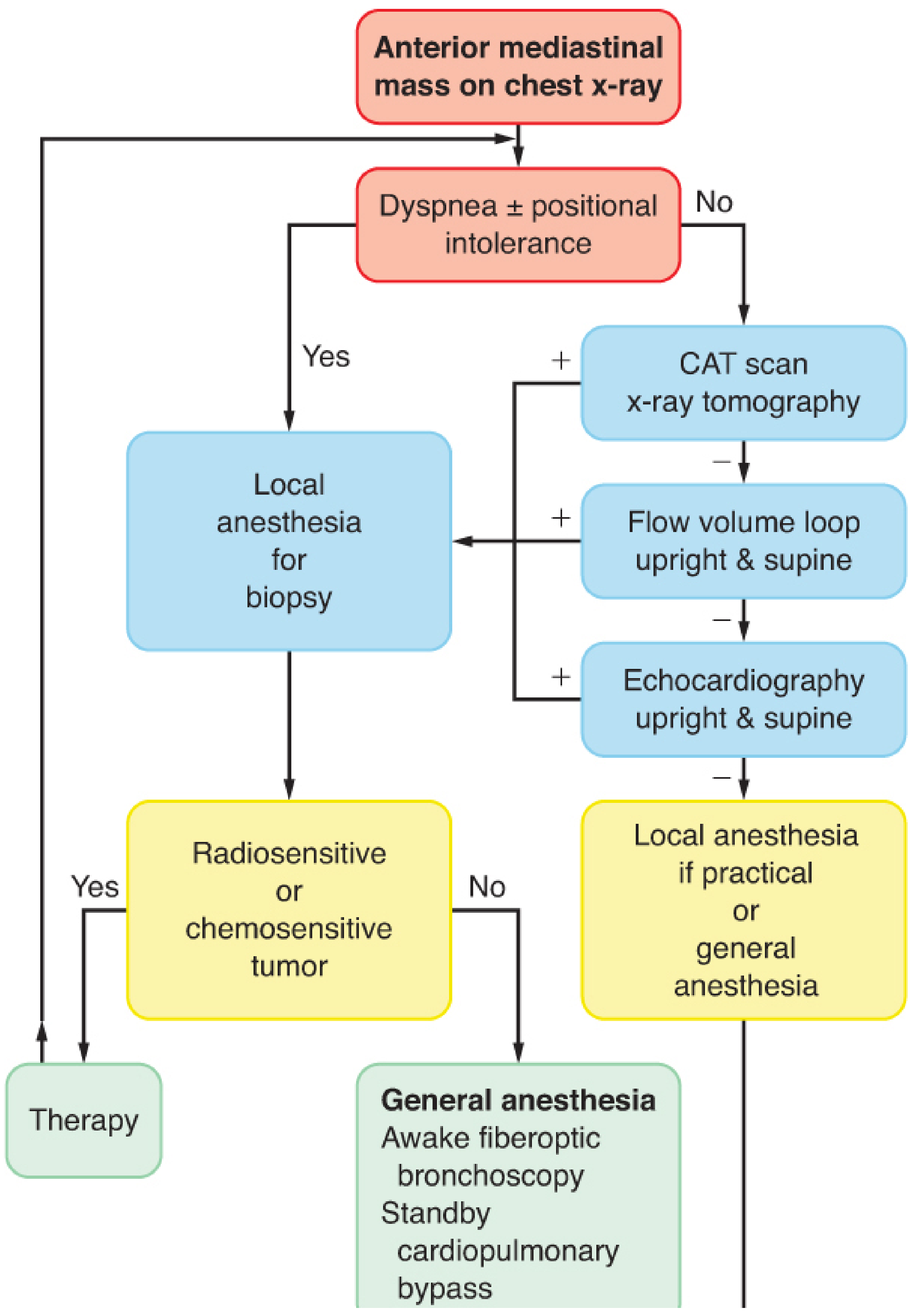
Preoperative Evaluation Flow Chart (Barash 9e):
Induction Principles (High-Risk/Symptomatic Patient)
| Principle | Rationale |
|---|---|
| Avoid neuromuscular blockade if possible | Paralysis removes the last mechanism maintaining airway patency |
| Maintain spontaneous ventilation | Preserved transpulmonary pressure gradient dilates compressed airways |
| Sevoflurane inhalational induction preferred | For uncooperative patients; maintains spontaneous ventilation |
| Awake fiberoptic intubation | For cooperative adults/older children; secure airway beyond the stenosis before GA |
| Armored (reinforced/anode) ETT | Passes through and maintains airway patency past compression |
| Semi-upright (reverse Trendelenburg) position | Gravity reduces mass compression on trachea |
| Pass ETT beyond the compression | Coughing/straining can cause complete obstruction from positive pleural pressure increase; passing the tube distally avoids this |
| Avoid ketamine-associated airway tone changes | Ketamine preferred for hemodynamic stability if cardiac compression |
Specific Drug Choices for Induction (Morgan & Mikhail 7e)
- IV ketamine - greater hemodynamic stability in patients with reduced cardiac output from vascular compression
- Inhalational sevoflurane - maintains spontaneous ventilation
- Small incremental propofol or etomidate - carefully titrated
Anticholinergic only as premedication (no sedatives); transport in semi-upright position with supplemental O2.
Intraoperative Airway Collapse - Rescue
If intraoperative airway collapse occurs:
- Reposition the patient (must have determined safest position preoperatively)
- Rigid bronchoscopy - pass distal to obstruction; can oxygenate even if into one main bronchus only
- Mount an ETT over a small rigid bronchoscope (e.g. 6 mm) and deliver it distal to the obstruction
- Femoro-femoral ECMO instituted beforehand for "unsafe" adult patients - CPB "standby" alone is inadequate because there is not enough time after sudden collapse to establish bypass before hypoxic brain injury
Extubation
- Keep intubated until airway obstruction has resolved
- Confirm by flexible bronchoscopy or presence of an air leak around the cuff when it is deflated
PART 3: MASK VENTILATION COMPRESSION POINTS
Specific to pediatric mask ventilation:
- Submandibular soft-tissue compression must be avoided - pressing the mask firmly against the face pushes the soft tissue under the mandible into the oropharynx, causing upper airway obstruction
- Oral airways displace the oversized tongue; nasal airways used with caution in children (can traumatize small nares or adenoids)
- In the neonate: slight neck extension in neutral position is optimal; avoid both flexion (large occiput causes this spontaneously) and hyperextension
SUMMARY TABLE: PEDIATRIC vs ADULT AIRWAY COMPRESSION
| Parameter | Adult | Pediatric/Neonate |
|---|---|---|
| Narrowest point | Vocal cords | Cricoid ring (functionally) |
| Laryngeal shape | Cylindrical | Funnel-shaped |
| Airway cartilage | Firm | Compressible/pliable |
| Risk from mediastinal mass | Lower | Higher (even asymptomatic) |
| Symptomatic reporting | Reliable | Unreliable |
| ETT choice | Cuffed | Uncuffed traditionally; cuffed increasingly used |
| Position for mask ventilation | Standard sniffing position | Neutral + slight extension; roll under shoulders if needed |
| Main mask ventilation hazard | Edentulous collapse | Submandibular soft-tissue compression |
| Safe tracheal compression threshold | Variable | >50% = unsafe for GA |
Key Exam Points:
- Functionally narrowest point in neonate = cricoid ring (not vocal cords as in adults)
- GA worsens airway compression by 3 mechanisms: reduced lung volume + bronchial relaxation + loss of diaphragmatic traction
- Children are at higher risk from anterior mediastinal masses due to more compressible cartilage AND inability to report symptoms
- Management priority: maintain spontaneous ventilation, secure airway beyond stenosis, rigid bronchoscope available
- Point of tracheobronchial compression from a mass may be distal to the ETT tip - always consider this
(Sources: Miller's Anesthesia 10e, Chapter 49; Barash Clinical Anesthesia 9e, Chapters 38 & 42; Morgan & Mikhail Clinical Anesthesiology 7e, Chapter 42)
This is a shared conversation. Sign in to Orris to start your own chat.