Structure present in ext auditory canal
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here is a thorough breakdown of the structures present in the external auditory canal (EAC):
Structures of the External Auditory Canal
The EAC extends from the concha of the auricle to the tympanic membrane and is approximately 2.4-2.5 cm long. It has two anatomically distinct segments.
1. Overall Framework
| Segment | Location | Length | Support |
|---|---|---|---|
| Cartilaginous (lateral) | Outer 1/3 | ~8 mm | Auricular cartilage |
| Bony (osseous) (medial) | Inner 2/3 | ~16 mm | Tympanic bone (floor/walls) + squamous bone (roof) |
- The isthmus is the narrowest point, located just medial to the cartilaginous-bony junction (about 5 mm from the tympanic membrane)
- The anterior recess (deep to the isthmus) is a wedge-shaped space between the anterior canal wall and tympanic membrane - a surgically difficult area
2. Structures of the Cartilaginous (Lateral) EAC
- Auricular cartilage - forms the skeletal framework; deficient superiorly at the incisura terminalis (used in endaural incisions)
- Fissures of Santorini - 2-3 anteroinferior perforations/fissures in the cartilage; allow passage of infection or tumour into the parotid gland
- Thick skin with well-developed subcutaneous layer containing:
- Hair follicles
- Sebaceous glands
- Ceruminous (cerumen) glands - modified apocrine sweat glands that produce cerumen (earwax)
3. Structures of the Bony (Osseous) EAC
- Tympanic bone - forms the floor and most of the canal wall; also carries the tympanic sulcus
- Squamous bone - forms the roof of the bony canal
- Two suture lines projecting into the canal with closely adherent overlying skin:
- Tympanosquamous suture (anteriorly)
- Tympanomastoid suture (posteriorly) - landmark for "vascular strip" incisions in surgery
- Tympanic sulcus - a groove at the medial end of the bony canal (absent superiorly) that holds the tympanic membrane; the absence superiorly creates the notch of Rivinus
- Thin skin with minimal subcutaneous layer - no hair follicles, sebaceous glands, or ceruminous glands (the absence of hair is what clinically distinguishes the bony from cartilaginous canal)
4. Lining (Entire Canal)
The EAC is lined by keratinizing stratified squamous epithelium. A unique property is epithelial migration - keratinocytes migrate outward (centrifugally) from the tympanic membrane toward the meatus, serving as a natural self-cleaning mechanism.
5. Innervation
Multiple nerves contribute sensory supply to the EAC:
- Auriculotemporal nerve (branch of CN V3 / trigeminal) - anterior wall and roof
- Greater auricular nerve (C3) - floor and posterior wall
- Lesser occipital nerve (C2, C3)
- Arnold's nerve (auricular branch of CN X / vagus) - posterior inferior wall; stimulation can trigger cough reflex or even vasovagal syncope
- Twigs from CN VII (facial nerve)
6. Blood Supply
The EAC receives blood from branches of the external carotid artery (posterior auricular and superficial temporal arteries).
Key Clinical Correlations
| Structure | Clinical Significance |
|---|---|
| Fissures of Santorini | Route for spread of EAC infection/cancer into parotid |
| Incisura terminalis | Site for endaural incision in ear surgery |
| Arnold's nerve | Stimulation causes cough ("Arnold's ear-cough reflex") |
| Ceruminous glands | Source of cerumen impaction; can give rise to ceruminous adenoma/adenocarcinoma |
| Isthmus | Narrowest point - cerumen tends to impact here |
| Tympanic sulcus | Holds tympanic membrane annulus in place |
Sources: Shambaugh Surgery of the Ear, pp. 54-55; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2; Cummings Otolaryngology Head and Neck Surgery
Diagramatically
Generating Image
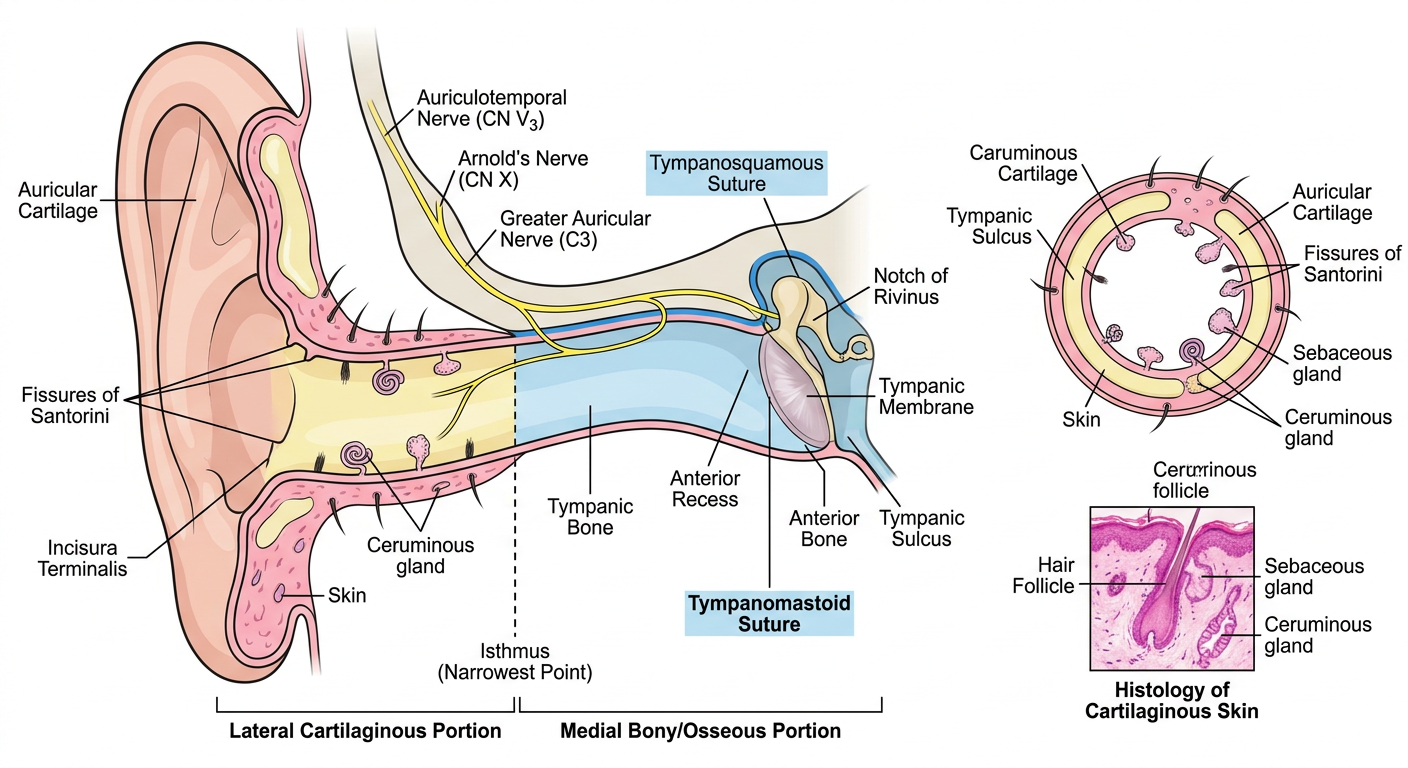
Here is a diagrammatic overview of the key structures:
Lateral (Cartilaginous) 1/3 - yellow zone:
- Auricular cartilage framework
- Incisura terminalis (superior gap)
- Fissures of Santorini (anteroinferior perforations)
- Thick skin with hair follicles, sebaceous glands, and ceruminous glands
Medial (Bony/Osseous) 2/3 - blue zone:
- Tympanic bone (floor/walls) + squamous bone (roof)
- Tympanosquamous suture (anterior) and tympanomastoid suture (posterior)
- Thin skin - no adnexal structures
- Isthmus (narrowest point, ~5 mm from tympanic membrane)
- Anterior recess (wedge-shaped space)
- Tympanic sulcus + notch of Rivinus (holds the tympanic membrane)
Nerve supply: Auriculotemporal (CN V3), Arnold's nerve (CN X), Greater auricular (C3), CN VII twigs
Thanks
You're welcome! Feel free to ask anytime you need more anatomy, clinical correlations, or any other topic. Good luck with your studies!
Explain structure of typanic membrane imp for neet pg
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete, NEET PG-focused breakdown of the tympanic membrane (TM):
Tympanic Membrane - Structure (NEET PG High Yield)
1. Basic Facts (Frequently Tested)
| Feature | Value |
|---|---|
| Shape | Slightly oval, broader above |
| Longest diameter (posterosuperior to anteroinferior) | 9-10 mm |
| Shortest diameter | 8-9 mm |
| Total area | 70-80 mm² |
| Effective vibrating area | 55 mm² |
| Angle with EAC floor | ~55° (oblique, slopes medially downward and forward) |
2. Layers (Trilaminar / 3 or 4 Layers - Both Correct)
Simple version (3 layers):
- Outer layer - Squamous (keratinizing stratified squamous) epithelium, continuous with skin of EAC
- Middle layer (Pars Propria / Lamina Propria) - Fibrous layer; contains radial fibres (outer) + circular fibres (inner, parabolic/transverse deeper)
- Inner layer - Mucous membrane (mucosal epithelium), continuous with middle ear lining
Detailed version (4 layers per KJ Lee):
- Squamous epithelium (outer)
- Radiating fibrous layer
- Circular fibrous layer
- Mucosal layer (inner)
Key exam point: The pars flaccida lacks proper radial and circular fibres - its lamina propria has randomly oriented collagen. This makes it weak and prone to retraction pockets and cholesteatoma.
3. Two Parts of TM (Most Important!)
| Pars Tensa | Pars Flaccida (Shrapnell's Membrane) | |
|---|---|---|
| Location | Inferior (larger) part | Superior, in notch of Rivinus |
| Borders | Bounded by anterior + posterior malleolar folds | Above anterior and posterior malleolar folds |
| Fibrous layer | Well-developed (radial + circular) | Absent / poorly defined |
| Annulus | Present (fibrocartilaginous ring) | Absent |
| Clinical significance | Central perforations (safe/tubotympanic CSOM) | Attic perforations, cholesteatoma (unsafe/atticoantral CSOM) |
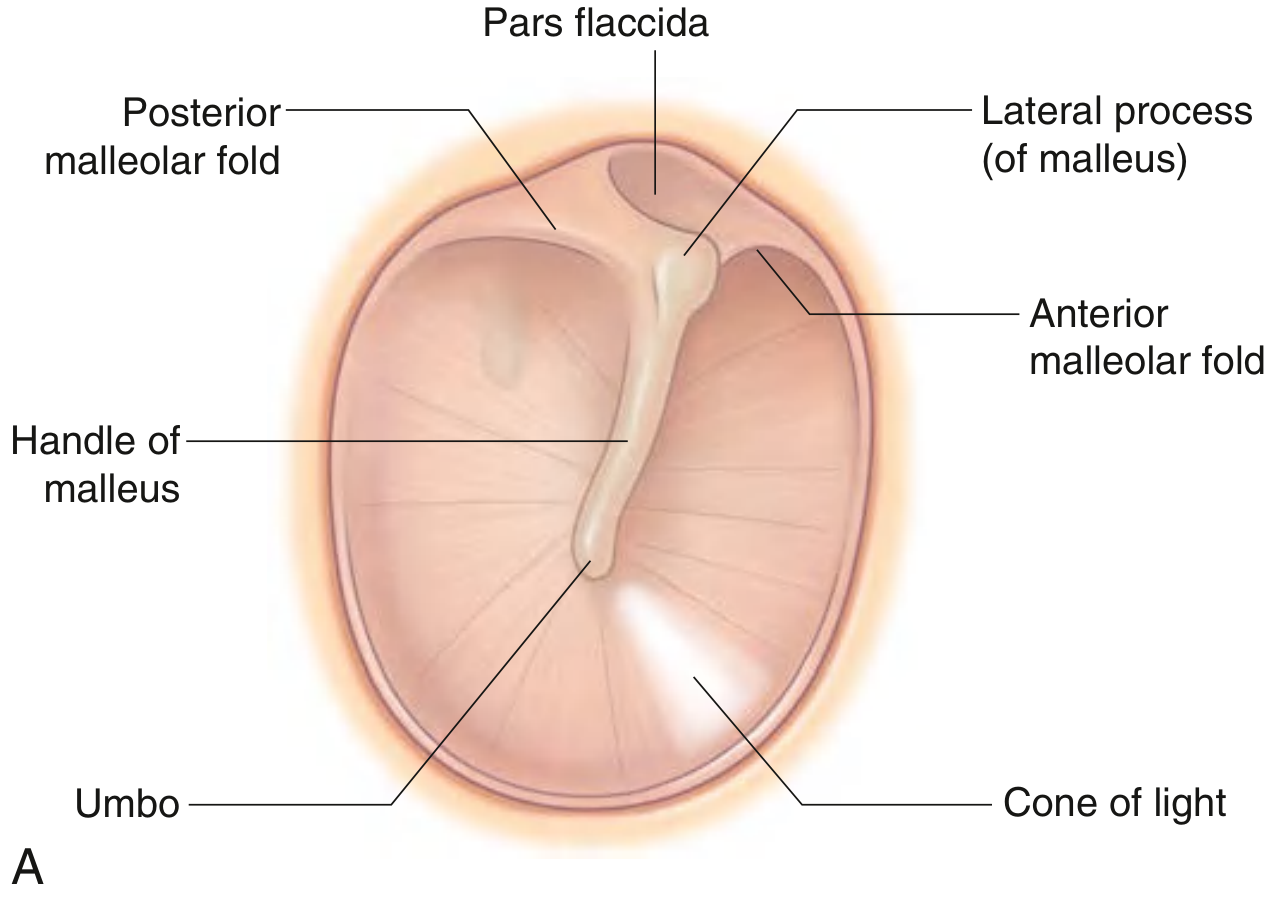
4. Key Landmarks on TM (Otoscopic View)
Pars Flaccida (Shrapnell's)
/\
Post. ---/--\--- Ant. Malleolar fold
mall. fold Lateral process of malleus (bulge)
|
Handle of Malleus (manubrium)
|
UMBO ← apex of cone, tip of manubrium
\
Cone of Light (anteroinferior)
- Umbo - apex of the cone-shaped TM; point of attachment of tip of manubrium of malleus; most concave point
- Cone of Light (Light Reflex) - anteroinferior to umbo; points to 5 o'clock in right ear, 7 o'clock in left ear
- Lateral process of malleus - small projection superiorly, above which pars flaccida sits
- Anterior malleolar fold - runs from lateral process to anterior tympanic spine
- Posterior malleolar fold - runs from lateral process to posterior tympanic spine
5. Prussak's Space (Lateral Epitympanic Recess) ★★ NEET Favorite
- Bounded laterally by pars flaccida (Shrapnell's membrane)
- Medially by neck of malleus + lateral malleal ligament
- Anterosuperiorly by anterior malleal fold
- Inferiorly by posterior malleal fold / lateral process of malleus
- Clinical importance: Primary site for pars flaccida cholesteatoma formation
6. Attachment
- Tympanic annulus (fibrocartilaginous ring) sits in the tympanic sulcus of the tympanic bone
- Sulcus is absent superiorly = notch of Rivinus (where pars flaccida sits, with no annulus)
- TM is firmly attached to malleus at:
- Lateral process (superiorly)
- Umbo (at tip of manubrium)
- Between these two points = only a flimsy plica mallearis connects them
7. Blood Supply
| Surface | Supply |
|---|---|
| Outer (epidermal) | Deep auricular branch of maxillary artery |
| Inner (mucosal) | Anterior tympanic branch of maxillary artery + stylomastoid branch of posterior auricular artery + middle meningeal artery |
8. Nerve Supply
| Nerve | Area |
|---|---|
| Auriculotemporal nerve (CN V3) | Outer surface (primary) |
| Arnold's nerve (auricular branch of CN X) | Outer surface (posteroinferior) |
| Tympanic branch of CN IX (Jacobson's nerve) | Inner (mucosal) surface |
| Facial nerve (VII) twigs | Small contribution |
Exam tip: CN IX (Jacobson's nerve) supplies the inner surface; stimulation can refer pain to the throat/tongue base.
9. Clinical Correlates (High Yield)
| Point | Significance |
|---|---|
| Pars flaccida = no fibrous layer | Site of attic (unsafe) cholesteatoma |
| Cone of light absent/displaced | Sign of middle ear effusion or retraction |
| Central perforation in pars tensa | Tubotympanic (safe) CSOM |
| Attic/posterosuperior perforation | Atticoantral (unsafe) CSOM - cholesteatoma |
| TM angle 55° to EAC | Must pull pinna up and back in adults to straighten canal for visualization |
| Effective vibrating area (55 mm²) vs stapes footplate (~3.2 mm²) | Creates ~17:1 hydraulic ratio for sound amplification |
Sources: KJ Lee's Essential Otolaryngology; Shambaugh Surgery of the Ear; Scott-Brown's Otorhinolaryngology Vol 2; Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.