How to read X ray from basics to advance
Reading File
Finding Sources
Finding Sources
Searching the Web
how to read chest X-ray systematic approach basics to advanced radiology
Finding Sources
Reading Web Page
https://radiologyassistant.nl/chest/chest-x-ray/basic-interp…
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have more than enough content to write a comprehensive, well-organized guide. Here is the full answer:
How to Read an X-Ray: A Complete Guide from Basics to Advanced
PART 1 - FUNDAMENTALS
1. What is an X-Ray and How Does It Work?
X-rays are ionizing radiation that passes through the body and is absorbed at different rates depending on tissue density. The result is a 2D grayscale image where tissues appear as:
| Appearance | Color on Film | Examples |
|---|---|---|
| Black (radiolucent) | Dark | Air, lung parenchyma |
| Dark gray | Medium-dark | Fat |
| Gray | Medium | Soft tissue, fluid |
| White (radiodense) | Bright white | Bone, metal, calcium |
The four basic densities you must memorize: Air < Fat < Soft tissue/fluid < Bone/metal
This density scale is the foundation of everything. When two structures of different density are adjacent, you see a visible border (interface). When two structures of the SAME density are adjacent, that border disappears - this is called the silhouette sign, and it is one of the most important diagnostic tools in radiology.
2. Types of Chest X-Ray Views
There are 3 main types of chest films:
PA (Posteroanterior) - Gold standard. X-ray tube is 180 cm behind the patient, film is in front. Taken in full inspiration with the patient erect. Gives the truest cardiac size and lung field assessment.
AP (Anteroposterior) - Portable/bedside view. The heart appears magnified (~15-20%) and the mediastinum wider. ALWAYS noted as AP on the film. Do not diagnose cardiomegaly on an AP film.
Lateral - Taken from the side. Invaluable for localizing lesions (upper vs. lower lobe, anterior vs. posterior mediastinum) and detecting retrocardiac and posterior costophrenic pathology invisible on PA.
3. Assessing Image Quality - "RIPE"
Before interpreting ANY chest X-ray, assess its technical quality:
R - Rotation
Look at the medial ends of the clavicles: they should be equidistant from the spinous process of the vertebra. If one clavicular head is closer, the patient is rotated toward that side. Rotation artificially shifts the mediastinum and can mimic pathology.
I - Inspiration
Count the anterior ribs above the diaphragm. You should see at least 6 anterior rib ends (ideally the 5th-6th rib intersects the mid-diaphragm). Poor inspiration causes the lung bases to look collapsed, the heart to look enlarged, and the mediastinum to appear wide.
P - Projection
Is it PA or AP? Check the label. The scapulae should lie outside the lung fields on a proper PA. On AP, they often overlap the lung.
E - Exposure/Penetration
A correctly exposed film allows you to just barely see the thoracic vertebral bodies through the heart. If overexposed (too dark), small opacities are hidden. If underexposed (too white), fine lung detail is obscured.
PART 2 - THE SYSTEMATIC APPROACH
Never scan randomly. Use a reproducible system every time. Two popular mnemonics are ABCDE and the Inside-Out approach. Both are described below.
The ABCDEF Approach (Best for Emergency Settings)
A - Airway
- Trace the trachea from the cricoid cartilage down to the carina (T4-5 level)
- The trachea should be midline or very slightly deviated to the right below the aortic arch
- Deviation AWAY from a lesion = tension pneumothorax, large effusion (push)
- Deviation TOWARD a lesion = collapse, fibrosis (pull)
- Check the carina angle - normally less than 70°. Widening suggests left atrial enlargement or subcarinal lymphadenopathy
- Identify both main bronchi
B - Breathing (Lungs and Pleura)
Compare lung fields symmetrically, zone by zone:
- Upper zones: above the clavicles to the front of the 2nd rib
- Middle zones: 2nd to 4th anterior ribs
- Lower zones: below the 4th anterior rib
Look for:
- Consolidation - white opacity within the lung that does NOT follow a lobar boundary strictly; air bronchograms may be visible (dark bronchi within the white opacity) - strongly suggests pneumonia, pulmonary edema, or infarction
- Collapse/Atelectasis - lobar collapse shifts the fissures, raises the diaphragm, and shifts the trachea/mediastinum toward the affected side
- Pneumothorax - look for a visible visceral pleural line with absent lung markings BEYOND it. Always check the apex and lung edges. On AP supine films it may appear as a deep sulcus sign
- Pleural effusion - blunting of the costophrenic angle (needs ~200-300 mL on PA erect). A meniscus shape that curves upward laterally is the classic sign. Massive effusion causes opacification of the hemithorax with contralateral mediastinal shift
- Pulmonary edema - bilateral interstitial/alveolar opacities, upper lobe vascular diversion, Kerley B lines (horizontal, peripheral, 1-2 cm long), peribronchial cuffing, bat-wing perihilar opacification
- Nodules/Masses - size, margin characteristics (spiculated vs. smooth), cavitation, calcification
- Interstitial patterns - reticulation, nodularity, honeycombing
The Silhouette Sign (advanced but essential):
- Right heart border is silhouetted (lost) by right middle lobe consolidation
- Left heart border is silhouetted by lingular consolidation
- Hemidiaphragm is silhouetted by lower lobe consolidation
- If the border is preserved, the opacity is NOT adjacent to that structure
C - Cardiac
- Size: Cardiothoracic ratio (CTR) = widest cardiac diameter / widest thoracic diameter. Normal <0.5 on a PA film. NOT reliable on AP
- Shape: Double density sign (left atrial enlargement), displaced left heart border (LV enlargement), prominent right heart border (RA enlargement)
- Pericardial effusion: globular, flask-shaped heart with clear lung fields
- Check the aortic knuckle - calcification, unfolding, or widening may indicate aortic pathology
- Mediastinal width - on PA, >8 cm is suspicious for widening. Causes: aortic dissection, lymphadenopathy, masses
D - Diaphragm
- The right hemidiaphragm is normally 1.5-2.5 cm HIGHER than the left (the liver elevates it)
- If the left is at the same level or higher than the right, consider:
- Gas under the left hemidiaphragm (normal: stomach bubble)
- Left hemidiaphragm elevation: phrenic nerve palsy, left lower lobe collapse
- Free air under the diaphragm (pneumoperitoneum) = perforated viscus emergency
- Diaphragm inversion = tension pneumothorax, large pleural effusion, large bullae
- The diaphragm outline should be SHARP. Loss of clarity implies adjacent pleural or pulmonary disease
- Costophrenic angles should be sharp and acute
Per Grainger & Allison: "In most people the diaphragm in the midlung field lies at the level of the fifth or sixth anterior rib interspace... In more than 90% of normal people the right hemidiaphragm is higher than the left."
E - Everything Else (Extras)
- Bones: All visible ribs (look for fractures, lytic or sclerotic lesions), clavicles, scapulae, humeri, thoracic spine (alignment, vertebral body height, pedicles)
- Soft tissues: Subcutaneous emphysema (streaky dark lucency in soft tissues), mastectomy absence, breast shadows, pacemakers, central lines, chest drains, foreign bodies
- Lines and tubes: Check every device position
- ET tube: tip should be 3-7 cm above carina
- Central venous line: tip at SVC/RA junction
- Nasogastric tube: below the diaphragm, to the left
- Chest drain: tip in the apex (pneumothorax) or base (effusion)
F - Fields and Fissures
- Look carefully at the lung apices - tuberculosis, Pancoast tumors, and apical bullae live here
- Fissures: The minor (horizontal) fissure runs horizontally at the right 4th rib anteriorly. The major (oblique) fissure runs obliquely and is best seen on the lateral view. Displaced fissures indicate lobar collapse or consolidation
- Kerley B lines: fine horizontal lines at the lung periphery (1-2 cm long) = interstitial edema or lymphangitis
- Assess vascularity: vessels should be barely visible in the outer third of the lung fields
PART 3 - ADVANCED INTERPRETATION
Understanding Lung Opacities
| Pattern | Key Features | Common Causes |
|---|---|---|
| Consolidation | Homogeneous opacity, air bronchograms, lobar/segmental | Pneumonia, pulmonary edema, hemorrhage, infarct |
| Collapse | Volume loss, fissure shift, mediastinal shift toward, diaphragm elevation | Mucus plug, endobronchial tumor, foreign body |
| Interstitial | Reticular (net-like), nodular, or mixed pattern | ILD, sarcoidosis, lymphangitis carcinomatosa |
| Nodule | Rounded opacity <3 cm | Metastasis, primary tumor, granuloma, AVM |
| Cavitation | Opacity with central lucency and thick/thin wall | Abscess, TB, squamous cell carcinoma, Wegener's |
| Pleural effusion | Meniscus, blunted angle, opacification | Heart failure, malignancy, infection, PE |
| Pneumothorax | Visible pleural line, absent markings | Trauma, spontaneous, iatrogenic |
Lobar Collapse Patterns (Advanced)
Each lobe collapses in a predictable direction. Knowing these lets you localize pathology:
- Right upper lobe collapse: Elevated right hilum, opacity in upper right zone, downward shift of minor fissure. "Juxtaphrenic peak" may be seen
- Right middle lobe collapse: Loss of the right heart border (silhouette sign), haziness at right base best seen on lateral
- Right lower lobe collapse: Triangular opacity behind the right heart, diaphragm elevation, downward and medial displacement of right hilum
- Left upper lobe collapse: Veil-like haze over the left upper zone, left hilum elevated, loss of left heart border
- Left lower lobe collapse: Triangular opacity behind the left heart, often missed unless you look hard
Air Bronchograms
Normally, bronchi are invisible on X-ray because the surrounding alveoli are also air-filled. When alveoli fill with fluid or cells (consolidation), the bronchi stand out as dark tubular branching structures within a white opacity. Air bronchograms = alveolar pathology. Their absence within an opacity suggests the opacity is not in the lung parenchyma (it may be pleural, or there is mucus plugging the bronchi too).
Reading the Mediastinum
Divide the mediastinum into compartments to narrow differentials:
Superior mediastinum (above aortic arch): Thyroid mass, thymic lesion, lymphadenopathy, tracheal deviation
Anterior mediastinum (in front of heart, the "4 T's"):
- Thymoma / Thymic carcinoma
- Teratoma / Germ cell tumor
- Thyroid (retrosternal goiter)
- Terrible lymphoma
Middle mediastinum (heart and great vessels): Lymphadenopathy, pericardial cyst, aortic aneurysm
Posterior mediastinum (behind heart): Neurogenic tumor, vertebral lesion, esophageal pathology, descending aortic aneurysm
Key Radiographic Signs to Know
| Sign | Meaning |
|---|---|
| Silhouette sign | Loss of normal border = adjacent pathology of same density |
| Air bronchogram | Alveolar consolidation |
| Deep sulcus sign | Pneumothorax on supine AP film |
| Luftsichel sign | Crescent of air lateral to aortic knuckle = left upper lobe collapse |
| Golden S sign | Right upper lobe collapse with central hilar mass |
| Sail sign | Right middle lobe/lingual collapse |
| Spinaker sail | Thymic shadow in infants |
| Eggshell calcification | Peripheral nodal calcification - silicosis, sarcoidosis |
| Tree-in-bud | Centrilobular nodules in branching pattern - endobronchial spread of infection |
| Westermark sign | Focal oligemia in pulmonary embolism |
| Hampton's hump | Wedge-shaped pleural opacity in PE |
PART 4 - PRACTICAL WORKFLOW
Presenting a Chest X-Ray (Clinical Setting)
Follow this structure every time:
- "This is a PA/AP chest radiograph of [patient ID], taken on [date]"
- "Image quality: [rotation/inspiration/exposure - any issues?]"
- "Airway: trachea is central/deviated [to which side]"
- "Cardiac: CTR is [normal/<0.5] on this PA film, heart borders are [well-defined/obscured]"
- "Mediastinum: [normal contour/widened/abnormal]"
- "Lungs: [clear bilaterally / describe any opacities, zone and side]"
- "Pleura: [no effusion/no pneumothorax / describe findings]"
- "Diaphragm: [normal/elevated/flattened], costophrenic angles [sharp/blunted]"
- "Bones and soft tissues: [no acute bony injury / describe]"
- "Impression: [summary diagnosis] in keeping with [clinical context]"
PART 5 - HOW TO PRACTICE
- Use a systematic method every single time - even on normal films. This builds the habit before you need it on an abnormal one.
- Start with normals - you cannot recognize abnormal if you do not know normal thoroughly.
- Build pattern recognition - look at hundreds of cases. Resources: Radiology Assistant, Radiology Masterclass, and the IEM X-ray guide.
- Practice with a lateral view - Always try to obtain and read the lateral in conjunction with the PA. Posterior costophrenic pathology and retrosternal masses are missed without it.
- Correlate clinically - A radiograph is never read in isolation. Patient age, symptoms, and history narrow differentials dramatically.
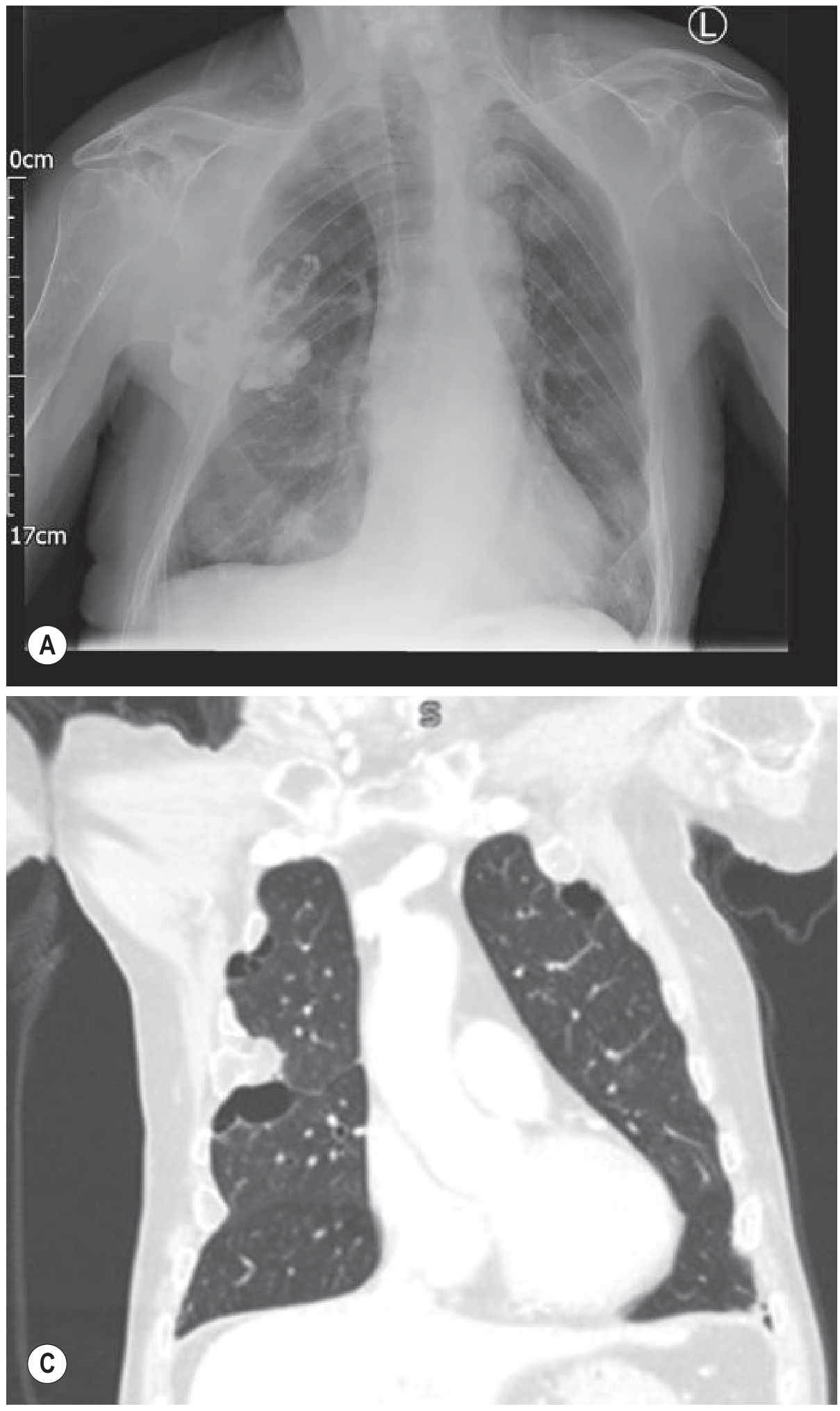
Here is an example of a normal PA chest X-ray alongside a CT coronal comparison for reference:
This video by Geeky Medics provides an excellent structured walkthrough of the ABCDE approach with live case examples:
Quick Reference Summary
| Step | What to Assess | Key Points |
|---|---|---|
| RIPE | Image quality | Rotation, Inspiration, Projection, Exposure |
| A | Airway | Trachea midline, carina angle, bronchi |
| B | Breathing | Opacities, PTX, effusion, lung markings |
| C | Cardiac | CTR <0.5, borders, mediastinum |
| D | Diaphragm | Height, angles, free air |
| E | Everything else | Bones, lines, devices, soft tissue |
| F | Fields/Fissures | Apices, fissures, Kerley B lines |
Sources used: Grainger & Allison's Diagnostic Radiology, Roberts and Hedges' Clinical Procedures in Emergency Medicine, Radiology Assistant, IEM-student.org
This is a shared conversation. Sign in to Orris to start your own chat.