Clinical examination of ear
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information from the top ENT textbooks. Let me compile the full response.
Clinical Examination of the Ear
Sources: Cummings Otolaryngology Head and Neck Surgery; Bailey & Love's Short Practice of Surgery 28th Ed; Shambaugh Surgery of the Ear
1. Instruments Required
- Fibreoptic otoscope (with pneumatic attachment and assorted specula)
- 512-Hz tuning fork (standard for Rinne and Weber tests; a full complement of 256, 512, and 1024 Hz is ideal)
- Head light or head mirror
- Jobson Horne probe
- Microscope (for detailed middle ear assessment)
2. General Approach
Ear examination is part of the complete ENT assessment. Always examine both ears and compare sides. Begin with inspection before instrumentation. A cranial nerve (CN) survey - particularly CN VII (facial nerve) - is an integral part of the otologic exam.
3. The Pinna (Auricle)
Visual inspection of the pinna and periauricular skin comes first.
Anatomical landmarks to identify:
| Landmark | Notes |
|---|---|
| Tragus / Antitragus | Tenderness suggests OE vs mastoiditis |
| Helix / Antihelix | Loss of fold = "bat ear" deformity |
| Concha cavum & cymba | Common site for seborrheic dermatitis |
| Triangular fossa | - |
| Lobule | - |
| External auditory meatus | Note calibre, discharge, skin quality |
Abnormalities to look for:
- Pre-auricular pits or tags (may drain; associated with branchial anomalies)
- Microtia (spectrum from small pinna to anotia; frequently associated with EAC atresia)
- Cauliflower ear - loss of cartilage structure after trauma/devascularization
- Perichondritis - exquisitely tender erythema and edema of the pinna; infectious forms may involve the lobule; non-infectious (relapsing polychondritis) tends to spare the lobule
- Gout tophi on the helix
- Post-auricular region: erythema, tenderness, and displacement of the pinna anteroinferiorly suggest mastoiditis
4. Otoscopy - Technique
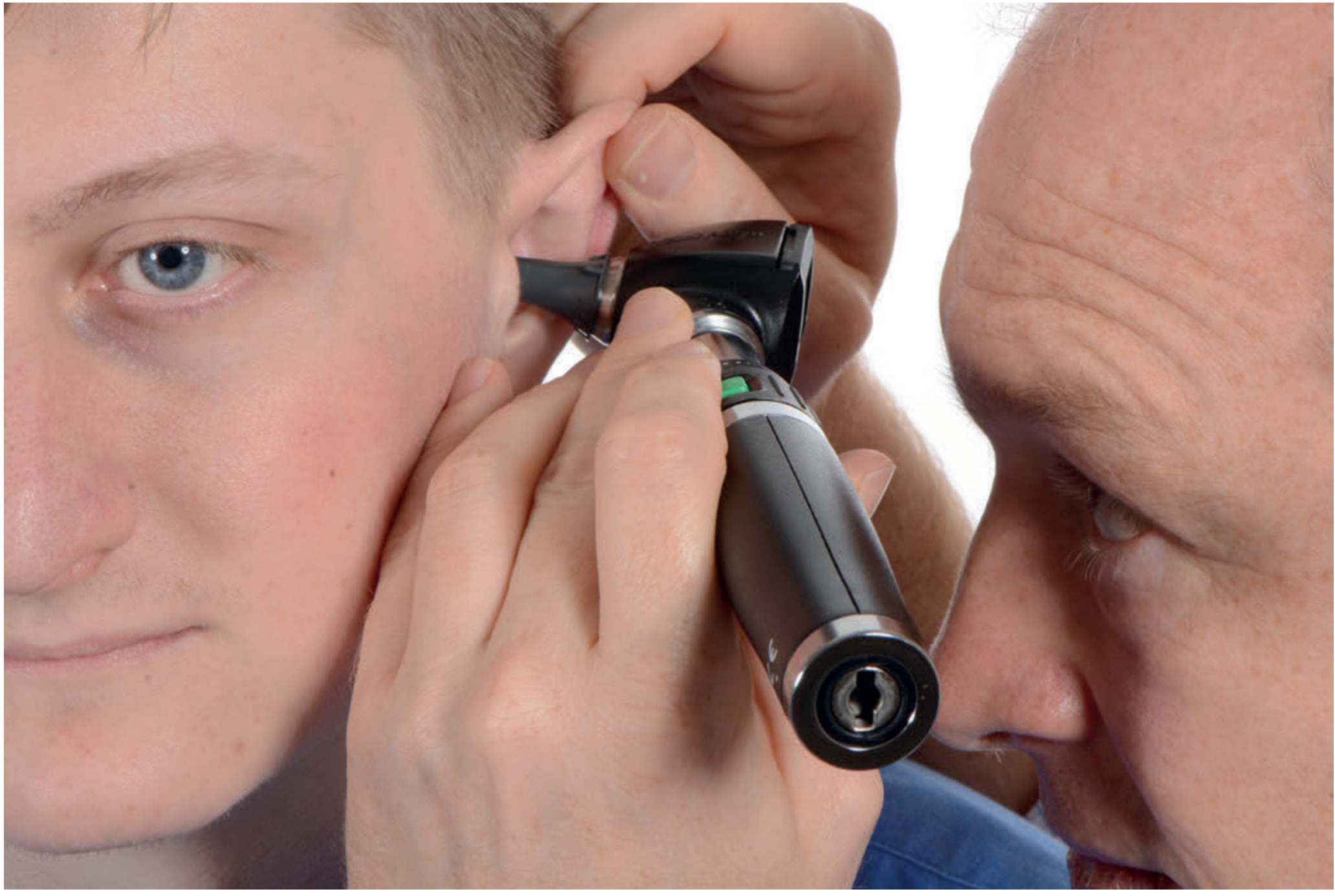
Fig. Correct otoscope technique: pinna is retracted superoposteriorly to straighten the EAC; the examiner's little finger rests on the patient's cheek to prevent sudden impingement on the tympanic membrane.
Technique:
- In adults: retract pinna superiorly and posteriorly to straighten the cartilaginous EAC
- In children: retract pinna inferiorly and posteriorly
- Hold the otoscope barrel so the little finger is braced against the cheek - prevents injury if the patient moves
- Use the largest speculum that fits comfortably
- A pneumatic attachment allows assessment of TM mobility (Siegle's speculum)
5. The External Auditory Canal (EAC)
The EAC has two portions:
| Portion | Characteristics |
|---|---|
| Lateral cartilaginous (1/3) | Thicker skin; hair follicles; cerumen glands |
| Medial bony (2/3) | Thin skin; no adnexal structures; junction = bony-cartilaginous junction |
Findings to document:
- Cerumen - colour, consistency, whether impacting view
- Otitis externa (OE) - edema, erythema, purulent/serous discharge; skin may swell to obliterate the lumen
- Fungal OE (otomycosis): "cottage cheese" discharge; visible fungal spores/fruiting bodies
- Granulation tissue in OE: must biopsy (r/o malignant OE - associated with Pseudomonas, diabetes)
- Osteomas: firm, bony protuberances from the superior/posterior medial EAC; can occlude the canal
- Cholesteatoma eroding into EAC: fullness in the posterior/superior EAC, skin-covered and soft
- Aural atresia: congenital failure to recanalize; short blind-ending canal or absent meatus
- Discharge character: serous (middle ear effusion), mucopurulent (ASOM/CSOM), bloody (trauma, carcinoma), foul-smelling (cholesteatoma)
6. The Tympanic Membrane (TM)
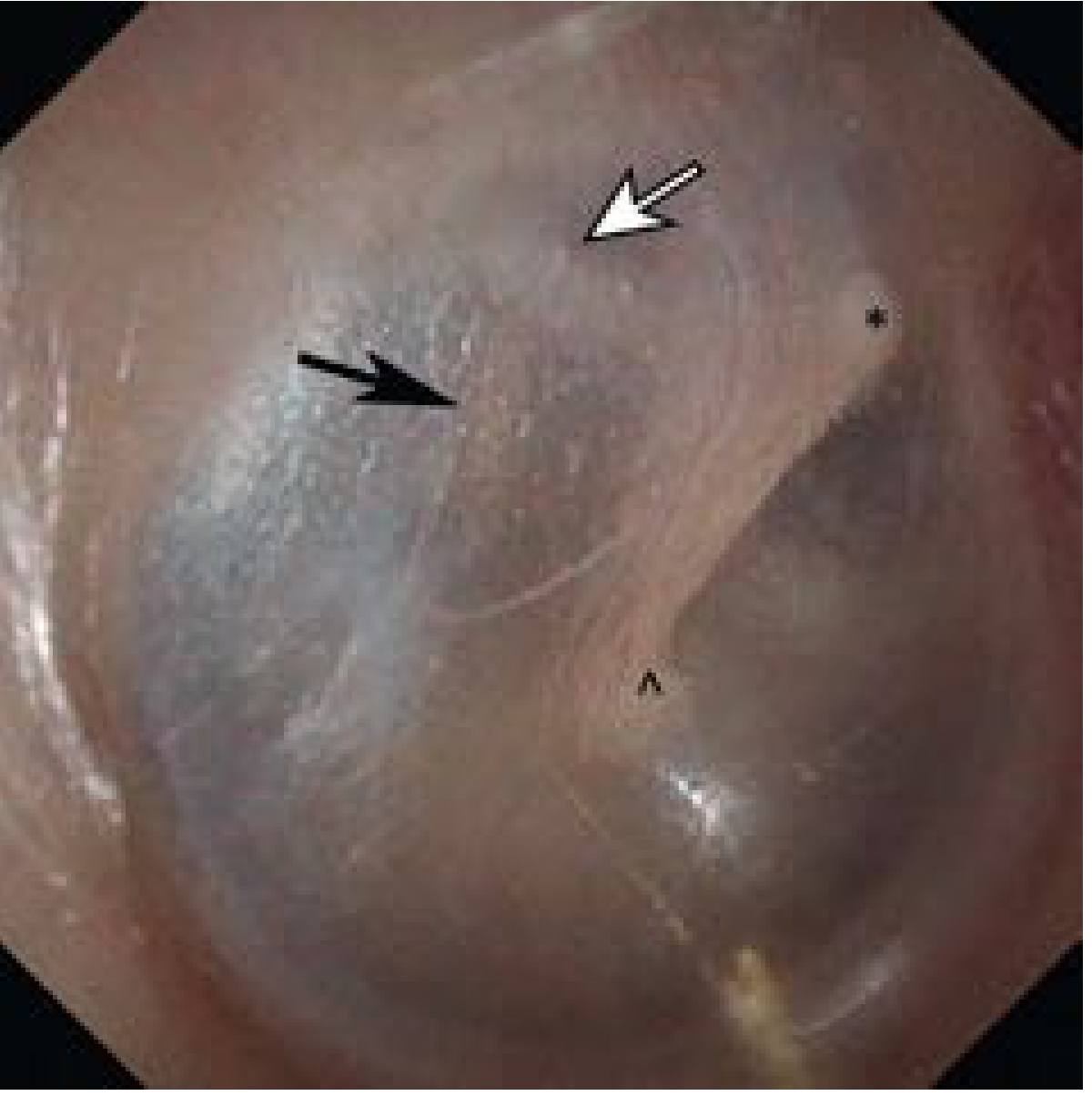
Fig. Normal tympanic membrane: (°) short process of malleus, (^) umbo, (white arrow) chorda tympani, (black arrow) long process of incus.
Normal TM: translucent to pearly gray; bipartite structure:
| Part | Location | Properties |
|---|---|---|
| Pars tensa | Majority of TM | Attached via tympanic annular ligament; taut |
| Pars flaccida | Superior, above notch of Rivinus | Lax; prone to retraction pockets |
Key TM landmarks:
- Handle (manubrium) of malleus - runs from the short process superiorly to the umbo centrally
- Light reflex (cone of light) - anteroinferior, from umbo
- Short process of malleus - most anterior-superior landmark
- Umbo - most inferior point of malleus handle
- Pars flaccida (Shrapnell's membrane) - superior
Abnormalities to assess:
- Perforations: Describe by location (clock-face quadrant) and whether central or marginal. Marginal perforations (involving the annulus) risk cholesteatoma formation.
- Retraction pockets: Negative pressure drawing TM into middle ear; pars flaccida retracts around the scutum - primary acquired cholesteatoma; pars tensa retracts posterosuperiorly
- Middle ear effusion (glue ear): Amber or yellow discolouration; air-fluid level or bubbles may be seen
- Acute suppurative OM: Red, bulging TM; loss of landmarks
- Tympanosclerosis: White chalky patches on TM (calcium deposits)
- Myringitis: Hemorrhagic blebs on TM (viral/Mycoplasma)
- Atelectasis: Generalized retraction of the TM against middle ear structures
TM mobility is tested with the pneumatic otoscope (Siegle's speculum) - reduced in middle ear effusion and negative middle ear pressure.
7. Tuning Fork Tests
A 512-Hz fork is standard. The complement 256, 512, and 1024 Hz gives the most complete assessment. Crucially, do not overstrike the fork - this generates resonant overtones that invalidate the test.
Weber Test
- Strike the fork; place on the nasofrontal suture or mid-forehead hairline
- Ask the patient which ear hears the tone louder, or if it is midline
| Result | Interpretation |
|---|---|
| Midline (not lateralized) | Normal hearing bilaterally, or symmetric loss |
| Lateralizes to the worse ear | Conductive hearing loss (CHL) on that side |
| Lateralizes to the better ear | Sensorineural hearing loss (SNHL) on the other side |
Rinne Test
- Strike the fork; place on the mastoid tip (bone conduction, BC)
- When the patient can no longer hear it, move in front of the meatus (air conduction, AC)
- Ask if the tone is audible at the meatus
| Result | Interpretation |
|---|---|
| AC > BC ("Positive Rinne") | Normal hearing or SNHL |
| BC > AC ("Negative Rinne") | Conductive hearing loss ≥20 dB in that ear |
Important: A "positive Rinne" is a normal result - the terminology is counterintuitive. The authors of Shambaugh prefer "AC > BC / BC > AC" to avoid confusion.
Combined Interpretation (Table from Cummings)
| Weber to Left | Weber to Right | |
|---|---|---|
| Rinne + bilaterally | SNHL right (or mild CHL left) | SNHL left (or mild CHL right) |
| Rinne - left only | CHL left | Mixed HL left |
| Rinne - right only | Mixed HL right | CHL right |
| Rinne - bilaterally | CHL left + Mixed HL right | CHL right + Mixed HL left |
Note: A false-negative Rinne can occur in profound SNHL when BC sound is heard by the contralateral normal ear (transcranial transmission).
8. Facial Nerve Assessment (CN VII)
This is integral to the otologic exam - the facial nerve runs through the temporal bone.
- Forehead wrinkling - upper face (bilateral cortical representation; spared in UMN lesions)
- Eye closure (orbicularis oculi) and Bell's phenomenon
- Nasolabial fold symmetry
- Mouth angle at rest and during movement
- House-Brackmann grading scale (I-VI) used to document degree of paresis
9. Lower Cranial Nerves
In skull base pathology the lower CNs must also be examined:
| CN | Test |
|---|---|
| CN IX (Glossopharyngeal) | Touch soft palate bilaterally; compare sensation |
| CN X (Vagal) | Laryngoscopy - vocal cord mobility; sensation |
| CN XI (Spinal accessory) | SCM strength; shoulder shrug; arm elevation above 90° |
| CN XII (Hypoglossal) | Tongue protrusion - deviation toward weak side; look for fasciculation/wasting |
10. Hearing Assessment Beyond Tuning Forks
Conversational testing gives a rough guide, but formal tests are required:
| Test | What it assesses |
|---|---|
| Pure-tone audiometry (PTA) | Air and bone conduction thresholds across frequencies; gold standard |
| Speech audiometry | Discrimination ability |
| Tympanometry | Middle ear pressure and TM compliance |
| Stapedial reflexes | Stapedius muscle contraction threshold |
| Otoacoustic emissions (OAEs) | Cochlear (outer hair cell) function |
| Electric response audiometry (ERA/ABR) | Neural integrity; used in threshold estimation and vestibular schwannoma workup |
11. Vestibular Bedside Examination
- Romberg test: Feet together, eyes closed, arms across chest. Sway/fall indicates postural control deficit.
- Dix-Hallpike maneuver: For posterior canal BPPV - rapidly recline patient with head turned 45°; look for latent-onset, fatigable geotrophic nystagmus
- Frenzel lenses: Used during positional testing to prevent fixation-suppression of nystagmus
- Head impulse test (HIT): Tests VOR integrity - a corrective saccade after a rapid head thrust toward the affected side indicates peripheral hypofunction
- Nystagmus evaluation: Direction (right-beating, left-beating), plane, position-dependence; peripheral nystagmus is horizontal/torsional, inhibited by fixation, never changes direction; central nystagmus changes direction, not inhibited by fixation
12. Radiological Investigations
- High-resolution CT temporal bones: Pre-operative anatomy, mastoid air cells, ossicular chain, bone erosion, facial canal, pus vs. air
- MRI: Soft-tissue detail, labyrinthine/retrocochlear pathology, vestibular schwannoma, cholesteatoma recurrence
References: Cummings Otolaryngology Head and Neck Surgery (9780323612173), Chapter 137; Bailey & Love's Short Practice of Surgery 28th Ed (9780367548117), Chapter 51; Shambaugh Surgery of the Ear (9781607950264), Chapter on Tuning Fork Tests.
This is a shared conversation. Sign in to Orris to start your own chat.