I’m doing a journal club presentation on this article, please explain in detail to present this article
cd /home/daytona/workspace/attachments/feaafa7f-cb65-4a4f-b2ba-34b0daf95c01/ && …
bicarbonate therapy metabolic acidosis diarrhea children
non-anion gap metabolic acidosis acute diarrhea severe dehydration children bicarbonate therapy
Journal Club Presentation Guide
Article Details
1. INTRODUCTION - Setting the Scene
Why this topic matters
- Diarrhea is the 3rd leading cause of infant deaths globally, responsible for 9.9% of under-5 mortality
- India alone accounts for ~20% of diarrhea-related under-5 deaths
- The classical mechanism of harm: diarrhea causes loss of water, bicarbonate, and electrolytes → dehydration, hypovolemic shock, and metabolic acidemia
The clinical problem this paper addresses
- sNAGMA was present in ~13% of critically ill children with acute diarrhea + severe dehydration
- Associated with: shock, acute kidney injury (AKI), coma, need for ventilation, renal replacement therapy, higher ICU use, and death
- Children with pH <7.00 or serum bicarbonate <5 mEq/L took up to 100 hours to resolve acidemia on WHO therapy alone
- Persistence of acidemia >24 h worsens organ dysfunction and increases mortality
The gap in evidence
- Concerns about adverse effects (hypernatremia, hypokalemia, hypocalcemia, paradoxical CSF acidosis, cerebral edema)
- No clinical trial evidence in this specific population
2. STUDY DESIGN
Type
- Open-label Randomized Controlled Trial (RCT)
- Single center: PGIMER, Chandigarh, India (1,950-bed tertiary teaching hospital)
- Conducted in the Pediatric Emergency Room (PER) and PICU
- Study period: April 2019 - March 2020 (12 months; originally planned 18 mo, shortened by COVID-19 lockdown)
Population - Who was included?
- Age: 1 to 144 months (1 month to 12 years)
- Acute diarrhea: >3 loose/watery/semisolid stools per 24h, for <7 days
- Severe dehydration (by WHO criteria)
- sNAGMA: pH ≤7.2 and/or serum bicarbonate ≤15 mEq/L + PaCO2 <45 mmHg + Anion Gap ≤16 mEq/L
Who was excluded?
- Pure high-anion gap metabolic acidemia (HAGMA)
- Extra-intestinal infection, chronic/persistent diarrhea
- Renal tubular acidosis, CKD, DKA, poisoning
- Inborn errors of metabolism
- Diuretic use
- Pre-enrollment IV rehydration therapy
Randomization
- Block randomization (block size 4) via web-based program
- Opaque sealed envelopes (serially numbered)
- Blinding was not possible (open-label) - this is a stated limitation
3. INTERVENTIONS - What exactly was done?
Control Group (n=25): Standard WHO rehydration therapy
- Ringer's Lactate (RL) over 6 hours for age <1 yr or <10 kg; over 3 hours for age >1 yr or >10 kg
- Ongoing diarrheal losses replaced with half-saline
- Maintenance fluids started after dehydration correction
Intervention Group (n=25): WHO therapy + Additional bicarbonate
0.3 × Body Weight × (15 - measured SB) mEq
Key design feature
4. OUTCOMES MEASURED
Primary Outcome
- Time to resolve metabolic acidemia = time to achieve pH ≥7.30 AND/OR serum bicarbonate ≥15 mEq/L
- Blood gases drawn at baseline then every 4 hours until target achieved
Secondary Outcomes
- Adverse outcome: composite of PICU transfer + all-cause in-hospital death/LAMA (Left Against Medical Advice)
- ACAFD5: Acute Care Area Free Days in 5 days (0 if stays >5d or dies; 5-x if discharged within 5d)
- Maximum Vasoactive Inotrope Score (VIS)
- Serum electrolyte changes (sodium, potassium, chloride, calcium)
- Renal function
- Hospital/PICU stay duration
Safety Monitoring
5. BASELINE CHARACTERISTICS - Were the groups comparable?
| Parameter | Control | Intervention | p-value |
|---|---|---|---|
| Age (months) | 4 (2, 9) | 4 (3, 9) | 0.73 |
| Males | 68% | 48% | 0.15 |
| Malnutrition (wt/age ≤-2z) | 72% | 72% | 1.0 |
| Shock at presentation | 16% | 20% | 1.0 |
| Median pH | 7.1 | 7.1 | 0.77 |
| Median Serum Bicarbonate | 7.8 mEq/L | 8.9 mEq/L | 0.55 |
| Acute Kidney Injury | 68% | 76% | 0.52 |
| pSOFA score | 4 (2,5) | 5 (3,5) | 0.24 |
- Median pH 7.09 - these are very sick children
- 36% had pH ≤7.00 (profound acidemia)
- 72% were malnourished; 42% had severe acute malnutrition (SAM)
- 70% had AKI, 18% had shock at presentation
- 7 had fluid-refractory shock requiring inotropes
6. RESULTS
Primary Outcome - Time to resolve acidemia
| Control | Intervention | p-value | |
|---|---|---|---|
| Median time (IQR) | 12 h (8, 24) | 8 h (4, 12) | 0.007 |
- 33% faster resolution with bicarbonate
- Kaplan-Meier log-rank test p = 0.005 (Fig. 1)
- By 8h: 17/25 (68%) vs. 9/25 (36%) - p = 0.035
- By 16h: 23/25 (92%) vs. 17/24 (71%) - p = 0.018
- SB >15 by 8h: 14/25 (56%) vs. 5/25 (20%) - p = 0.012
- pH >7.30 by 8h: 17/25 (68%) vs. 9/25 (36%) - p = 0.025
Secondary Outcomes
- Intervention: 0/25 (0%)
- Control: 5/25 (20%)
- p = 0.049 - statistically significant
- Intervention: 0
- Control: 2 (8%) - p = 0.25 (not significant individually, but the trend is clear)
- Intervention: 2 days (IQR 1,2)
- Control: 1 day (IQR 1,2)
- p = 0.12 (not significant, but clinically meaningful doubling)
- Intervention: max VIS = 10.5
- Control: max VIS = 34
- p = 0.62 (small numbers, n=2 vs n=4; clinically important difference)
- New hypernatremia: 16% vs 20% (p=0.50) - no increase
- New hypokalemia: 64% vs 64% (p=1.0) - same in both
- Hypocalcemia: none in either group
- Deterioration in sensorium: none in intervention group
7. SUBGROUP ANALYSIS
| Subgroup | Intervention (median time) | Control (median time) | Difference |
|---|---|---|---|
| SB ≤5 mEq/L (most severe) | 8 h (4, 12) | 12 h (8, 48) | 4 h faster |
| SB >10 mEq/L (less severe) | 4 h (4, 8) | 6 h (4, 10) | 2 h faster |
8. THE BICARBONATE FORMULA - Practical Teaching Point
| SB level | Formula |
|---|---|
| SB >10 mEq/L | 0.6 × BW × (15 - SB) × 0.5 |
| SB 5-10 mEq/L | 0.6 × BW × (15 - SB) × 0.75 |
| SB ≤5 mEq/L | 0.6 × BW × (15 - SB) × 1.0 |
9. DISCUSSION POINTS FOR YOUR PRESENTATION
Strengths
- First RCT to specifically test bicarbonate in ADSD with sNAGMA against WHO-RT
- Carefully controlled design - same total fluid volume, rate, and sodium in both arms
- Monitored and quantified safety outcomes rigorously
- Clinically relevant primary outcome (time to acidemia resolution) with hard secondary outcomes (death, ICU transfer)
- Practical formula and dilution protocol immediately applicable in resource-limited settings
Limitations (be prepared to discuss)
- Small sample size (n=50) - underpowered for mortality outcomes individually
- Open-label design - blinding impossible; assessment bias possible
- Single center - tertiary referral center in India; may not generalize to community hospitals
- COVID-19 shortened recruitment period (12 months instead of 18)
- PICU bed unavailability may have influenced "adverse outcome" composite (if a child needed PICU but no bed was available, this could alter the composite measure)
- Small subgroup numbers limit conclusions from subgroup analyses
Clinical Context
- In LMICs (lower-middle-income countries), this is especially important: late referrals mean sicker children, scarce PICU beds, and limited resources
- Sodium bicarbonate is an extremely cheap intervention
- The WHO protocol alone is insufficient for this subset
What this paper does NOT address
- Long-term outcomes (neurodevelopment, renal function after AKI)
- Oral rehydration therapy patients (all enrolled needed IV therapy)
- Children >12 years
10. CONCLUSIONS (from the authors)
- Additional bicarbonate infusion significantly reduced time to resolve sNAGMA by 33% (8h vs 12h)
- Significantly reduced adverse outcomes (PICU transfer + death) - 0% vs 20%
- No increase in hypernatremia, hypokalemia, hypocalcemia, or sensorium deterioration
- Provides simplified dosing formulas for busy pediatric emergency settings
- Calls for a large multicentric, stratified, blinded RCT to confirm findings
11. TAKE-HOME MESSAGE FOR YOUR AUDIENCE
In children with acute diarrhea + severe dehydration who develop severe non-anion gap metabolic acidemia (pH ≤7.2 or serum bicarbonate ≤15 mEq/L), adding calculated-dose IV bicarbonate to standard WHO rehydration therapy:
- Corrects the acidemia one-third faster
- Significantly reduces the need for ICU care and deaths
- Does so safely, without worsening electrolyte disturbances
Suggested Questions to Anticipate at Journal Club
- Why was open-label design used? - Blinding was practically impossible since the bicarbonate solution looks different from RL; the study design otherwise controlled for confounders well
- Why target SB of 15 mEq/L and not 24? - Partial correction avoids overcorrection/alkalemia risk; once the underlying diarrhea is treated, the kidneys can restore the remainder
- How significant is the composite outcome with only 5 vs 0 PICU transfers? - Small numbers, but the Fisher's exact p=0.049 is valid; the trend is clinically compelling
- Can this be applied to adults or other causes of NAGMA? - This trial was specifically designed for diarrhea-associated bicarbonate loss; extrapolation to other causes (e.g., RTA) requires separate evidence
- Why was the BICAR-ICU trial (Jaber et al., Lancet 2018) result different? - BICAR-ICU included mostly HAGMA patients (sepsis, lactic acidosis); this study specifically selected NAGMA from GI bicarbonate loss - fundamentally different pathophysiology
Find recent clinical guidelines on bicarbonate therapy in pediatric acidosis
bicarbonate therapy pediatric metabolic acidosis guidelines
clinical guidelines bicarbonate therapy pediatric metabolic acidosis 2023 2024 2025
sodium bicarbonate metabolic acidosis treatment children pediatric
bicarbonate diarrhea dehydration rehydration acidosis children
PMID: 37442665
PMID: 39533025
PMID: 39325135
PMID: 37196992
https://pmc.ncbi.nlm.nih.gov/articles/PMC10688456
Recent Clinical Guidelines & Evidence: Bicarbonate Therapy in Pediatric Acidosis
1. Overarching Principle (Current Consensus)
"Empiric use of sodium bicarbonate in patients with nontoxicologic causes of metabolic acidosis is not warranted... Emergency physicians should reserve use of this medication to conditions with clear benefit."
2. By Clinical Scenario
A. Diarrhea-Associated Non-Anion Gap Metabolic Acidosis (NAGMA)
- WHO rehydration guidelines (2005, still in force) recommend Ringer's Lactate as standard IV therapy but do not specifically address sNAGMA management
- Kraut & Kurtz (Clin Kidney J 2015, PMID 25699164) - a key reference cited in the Takia paper - recommend bicarbonate supplementation for non-anion gap acidosis from GI bicarbonate loss, but without pediatric RCT evidence at the time
- The Takia et al. 2025 RCT (your journal club article) provides the first RCT evidence supporting additional calculated-dose bicarbonate in children with ADSD + sNAGMA (pH ≤7.2 or SB ≤15 mEq/L)
- No major society has yet updated guidelines to formally incorporate this finding; a large multicentric RCT is still needed
- Balanced solutions likely shorten hospital stay (MD -0.35 days; moderate certainty)
- Higher final pH (MD +0.06) and bicarbonate (MD +2.44 mEq/L) with balanced solutions
- Lower risk of hypokalemia with balanced solutions
- Implication: Even the choice of base rehydration fluid (RL vs. normal saline) matters for acid-base outcomes
B. Diabetic Ketoacidosis (DKA)
- ISPAD (International Society for Pediatric and Adolescent Diabetes) Guidelines 2022: Do not use sodium bicarbonate in pediatric DKA. Evidence suggests it may worsen outcomes and is associated with increased risk of cerebral edema in children
- ADA/AAP consensus: Bicarbonate therapy in pediatric DKA is contraindicated except in life-threatening hyperkalemia with cardiac arrhythmia
- The 2025 Springer review on DKA in pediatric emergency medicine cites the 2023 Wardi review, confirming bicarbonate does not improve outcomes and may cause harm in pediatric DKA
- Wardi et al. (2023) explicitly state: "Recent data suggest that the use of sodium bicarbonate in diabetic ketoacidosis does not confer improved patient outcomes and may cause harm in pediatric patients"
C. Lactic Acidosis / Sepsis-Associated Acidosis
- BICAR-ICU Trial (Jaber et al., Lancet 2018): IV bicarbonate did not improve 28-day mortality overall in ICU patients with severe metabolic acidemia (pH ≤7.20). However, pre-specified subgroup with AKI (AKIN stage 2-3) showed significant reduction in 28-day mortality and need for renal replacement therapy
- This was an adult trial but informs pediatric PICU practice
- Surviving Sepsis Campaign (2020 Pediatric guidelines): Do not suggest bicarbonate for hemodynamic improvement in pediatric septic shock with lactic acidemia - treat the underlying sepsis and improve perfusion
- A 2025 target trial emulation study (Blank et al., Intensive Care Med 2025) found no mortality benefit from bicarbonate in ICU metabolic acidosis overall
D. Renal Tubular Acidosis (RTA)
- Distal RTA (dRTA): Lifelong alkali supplementation (sodium/potassium bicarbonate or citrate) is mandatory to prevent nephrocalcinosis, nephrolithiasis, reduced GFR, bone demineralization, and growth failure
- Target: maintain serum bicarbonate in the normal range (22-26 mEq/L)
- Novel drug approved (2024 - Europe): ADV7103 (potassium citrate + potassium bicarbonate extended-release) - approved by EMA for pediatric dRTA as first-line therapy, with better adherence than traditional formulations
- Proximal RTA: Higher doses required due to renal wasting; combined with potassium supplementation
E. Neonatal Metabolic Acidosis
- Concerns specific to neonates: Rapid bicarbonate infusion → rapid CO2 generation → intracellular acidosis, cerebral blood flow fluctuations, intraventricular hemorrhage risk (especially in preterm), osmolar load
- Current neonatal guidelines recommend:
- Address the underlying cause first
- Use Ringer's Lactate (instead of saline) for volume boluses
- Add acetate to parenteral nutrition for gradual correction
- Use oral citrate for slow, stable correction
- Reserve IV NaHCO3 for severe acute acidosis requiring immediate correction
- BASE Trial (UK, 2024 protocol): An ongoing RCT (Bicarbonate for AcidosiS in very prEterm babies) testing IV bicarbonate vs. control in preterm infants with metabolic acidosis - results awaited
- If bicarbonate is used: use diluted 4.2% solution (not 8.4%); infuse slowly; avoid bolus dosing
F. Hyperchloremic Metabolic Acidosis in PICU (Chloride-Guided Approach)
| Chloride level | Bicarbonate therapy effect |
|---|---|
| Hyperchloremia (Cl ≥113 mmol/L) | Associated with reduced mortality |
| Hypochloremia (Cl <107 mmol/L) | Associated with increased mortality |
| Normal chloride (Cl 107-112) | No clear mortality benefit |
G. Cardiac Arrest / Sodium Channel Blockade / Severe Hyperkalemia
- Tricyclic antidepressant overdose → sodium channel blockade → IV NaHCO3 (bolus to raise pH >7.45) is standard
- Severe hyperkalemia with ECG changes → IV NaHCO3 as temporizing measure
- Cardiac arrest associated with above → NaHCO3 indicated
- These indications remain consistent across pediatric emergency guidelines
3. Practical Summary Table
| Condition | Guideline Recommendation | Strength |
|---|---|---|
| Diarrhea + sNAGMA in children | Consider bicarbonate if pH ≤7.2/SB ≤15; no formal guideline yet | Emerging RCT evidence |
| Pediatric DKA | Contraindicated (except life-threatening hyperkalemia) | Strong (ISPAD 2022) |
| Sepsis/lactic acidosis | No routine use; consider if AKI stage 2-3 | Moderate (BICAR-ICU, SSC) |
| Distal RTA | Lifelong bicarbonate/citrate mandatory | Strong (expert consensus) |
| Neonatal acidosis | Cautious use; prefer RL/acetate/citrate; reserve NaHCO3 for severe acute cases | Moderate (expert review 2025) |
| Hyperchloremic NAGMA in PICU | Beneficial if Cl ≥113 mmol/L; harmful if Cl <107 mmol/L | Moderate (retrospective data) |
| TCA overdose, severe hyperkalemia | Clearly indicated | Strong |
4. Adverse Effects to Monitor (Across All Scenarios)
- Hypernatremia - from sodium load (use diluted solutions or isonatremic preparations as in the Takia protocol)
- Hypokalemia - intracellular K+ shift with alkalinization; slow infusion mitigates this
- Hypocalcemia - alkalosis lowers ionized calcium; can precipitate tetany, seizures
- Paradoxical CSF acidosis - CO2 crosses blood-brain barrier faster than bicarbonate; transient intracellular acidosis
- Cerebral edema - especially in DKA; drives the strong contraindication
- Metabolic alkalosis overshoot - avoid targeting full normal bicarbonate in acute settings; target partial correction (SB 15 mEq/L as a safe endpoint, per Takia et al.)
5. Bottom Line for Your Journal Club Context
Explain kaplan Meier graph in the article
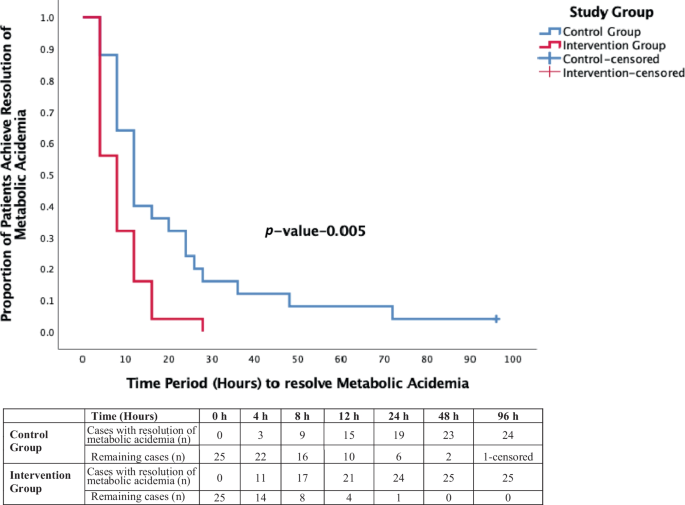
Explaining the Kaplan-Meier Graph (Figure 1)
What Is a Kaplan-Meier Curve? (Background for your audience)
- The Y-axis (vertical) shows the proportion of patients who have NOT yet had the event (i.e., still unresolved acidemia). It starts at 1.0 (100% of patients unresolved) and falls toward 0 as patients achieve resolution.
- The X-axis (horizontal) shows time in hours.
- Each step downward in the curve represents one or more patients achieving the event (acidemia resolved).
- A tick mark (+) on a curve indicates a censored observation - a patient who left the study (e.g., died) before achieving the event. Their data is still used up to the point they were censored, then excluded.
Reading This Specific Graph
The Two Curves
| Control Group (Blue) | Intervention Group (Red) | |
|---|---|---|
| Treatment | WHO Ringer's Lactate only | WHO RL + bicarbonate infusion |
| Starting n | 25 | 25 |
| Curve behavior | Falls slowly, stretches to 96 hours | Falls steeply, reaches zero by ~28 hours |
Walking Through the Data Table (Step by Step)
| Time | Intervention: resolved | Intervention: remaining | Control: resolved | Control: remaining |
|---|---|---|---|---|
| 0 h | 0 | 25 | 0 | 25 |
| 4 h | 11 | 14 | 3 | 22 |
| 8 h | 17 | 8 | 9 | 16 |
| 12 h | 21 | 4 | 15 | 10 |
| 24 h | 24 | 1 | 19 | 6 |
| 48 h | 25 | 0 | 23 | 2 |
| 96 h | 25 | 0 | 24 | 1-censored |
What does this tell us?
- Intervention: 11 of 25 (44%) already resolved - nearly half the group corrected in just 4 hours
- Control: only 3 of 25 (12%) resolved - the vast majority are still acidemic
- This early divergence shows bicarbonate acts quickly
- Intervention: 17/25 (68%) resolved - the curve has crossed the 50% mark (this is the median time = 8 hours)
- Control: only 9/25 (36%) resolved - the median hasn't been reached yet
- Control: 15/25 (60%) resolved - curve finally crosses 50% (median = 12 hours)
- Intervention: 21/25 (84%) already resolved
- Intervention: All 25 patients resolved - the red curve hits zero
- Control: Still 2 patients unresolved
- One patient in the control group died before resolving acidemia
- On the graph, this appears as the small blue "+" tick at 96 hours
- KM methodology correctly excludes them from the denominator after the point of censoring, so the curve reflects the true event rate among those still being followed
The Statistical Test: Log-Rank p = 0.005
- The log-rank test compares the entire shape of both curves, not just two time points
- It asks: "Is the difference in time-to-event between the two groups larger than what we'd expect by chance?"
- p = 0.005 means there is only a 0.5% probability this difference occurred by chance
- This is highly statistically significant (well below the 5% threshold)
- The Mann-Whitney U test on the median times independently gave p = 0.0067 - consistent
The Key Takeaway in Plain Language
At every single time point measured - 4h, 8h, 12h, 24h, 48h - more children in the bicarbonate group had resolved their acidemia than in the control group. The gap opened up early and never closed. By 48 hours, every child in the bicarbonate group was corrected, while 2 in the control group were still acidemic (and one of those eventually died before correcting). The log-rank test confirms this was not a chance finding.