Anatomy of breast
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Excellent - I now have rich, comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Anatomy of the Breast
Sources: Sabiston Textbook of Surgery, Fischer's Mastery of Surgery, Mulholland & Greenfield's Surgery, Gray's Anatomy for Students, Thieme Atlas of Anatomy
1. Position and Surface Anatomy
The breast lies on the anterior thoracic wall, between the 2nd rib superiorly and the 6th rib inferiorly, from the sternal edge medially to the midaxillary line laterally. It overlies the pectoralis major, serratus anterior, external abdominal oblique muscles, and the upper extent of the rectus sheath. A tongue of breast tissue extends superlaterally around the lower margin of the pectoralis major into the axilla - this is called the axillary tail (axillary process of Spence).
The average nonlactating breast weighs 150-225 g; the lactating breast may exceed 500 g. The left breast is commonly slightly larger than the right.
- Gray's Anatomy for Students, p. 274 | Fischer's Mastery of Surgery, p. 3866
2. Structural Layers
The breast is composed of three layers:
| Layer | Contents |
|---|---|
| Skin | Hair follicles, sebaceous glands, sweat glands |
| Subcutaneous tissue | Fat, cutaneous blood vessels, lymphatics, nerves |
| Breast parenchyma | Glandular epithelium + fibrous stroma + adipose tissue |
The breast lies between the skin/subdermal adipose tissue anteriorly and the superficial pectoral fascia posteriorly, which overlies the pectoralis major. Behind the breast, a potential space called the retromammary space separates it from the pectoralis fascia, and contains loose connective tissue and lymphatics.
- Sabiston Textbook of Surgery, p. 1369
3. Cutaway Diagram - Internal Structure
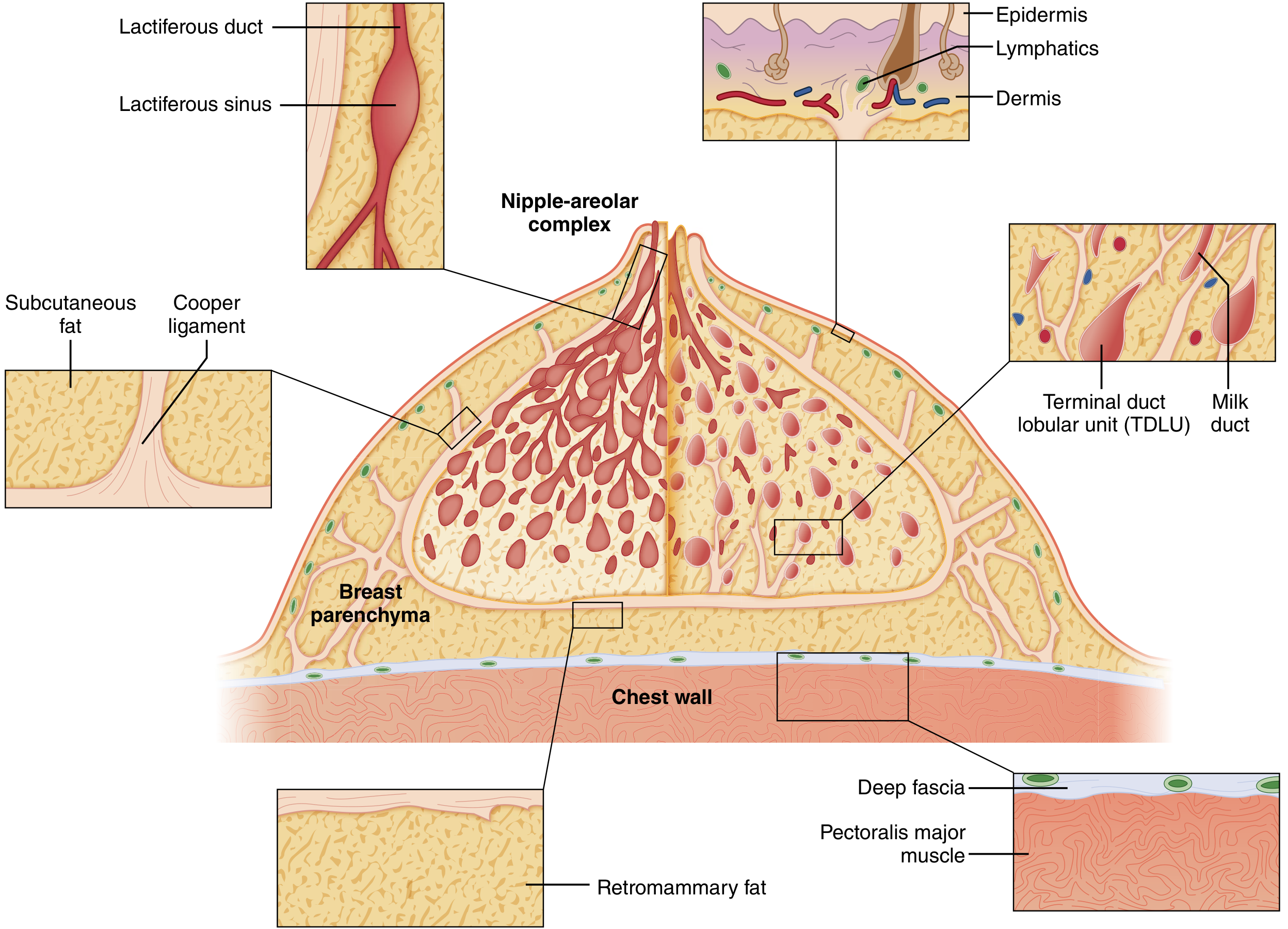
Cutaway diagram of the mature resting breast (Sabiston). Key structures shown: Cooper ligaments, lactiferous duct system, terminal duct lobular units (TDLUs), retromammary fat, and pectoralis major.
4. Glandular Structure (Lobes, Lobules, Ducts)
The glandular apparatus is organized like an inverted tree:
- There are 15-20 lobes, each ending in a lactiferous duct that opens at the nipple
- Each lactiferous duct has a dilated segment beneath the areola - the lactiferous sinus
- Each lobe is divided into 20-40 lobules, which themselves contain 10-100 alveoli (acini)
- The acini and their small efferent ductules form the Terminal Duct Lobular Unit (TDLU) - the basic secretory unit of the breast, and the site of origin of most breast malignancies
- The ducts are arranged in a radial pattern spreading outward from the nipple-areolar complex (NAC)
- The TDLU is invested in specialized loose intralobular stroma (containing capillaries, lymphocytes, mononuclear cells), distinct from the denser interlobular stroma and adipose tissue
In adolescents, epithelium and stroma predominate. After menopause, glandular structures involute and are largely replaced by adipose tissue.
- Sabiston, p. 1369-1370 | Thieme Atlas, p. 229 | Fischer's, p. 3866
5. Suspensory Ligaments of Cooper
Multiple fibrous bands called Cooper's ligaments (suspensory ligaments of the breast) run from the deep fascia (pectoralis fascia) to the dermis, providing shape, support, and mobility to the breast. Because they anchor into the skin, infiltration by cancer or edema causes dimpling of the skin - the classic "peau d'orange" (orange-skin) appearance.
- Sabiston, p. 1369 | Fischer's, p. 3866
6. Nipple-Areolar Complex (NAC)
- The skin of the nipple and areola is highly pigmented, composed of stratified squamous epithelium
- Deep to the NAC are bundles of smooth muscle arranged radially, circumferentially, and longitudinally - these allow nipple erection
- Along the areola margin are Montgomery glands (accessory glands), with nodular elevations called tubercles of Morgagni
- The nipple contains numerous free sensory nerve endings and Meissner corpuscles; the areola contains Ruffini-like endings and Krause end-bulbs, making both highly innervated
- Fischer's Mastery of Surgery, p. 3867
7. Blood Supply
Arterial Supply
| Artery | Branches to Breast |
|---|---|
| Internal thoracic (internal mammary) artery | Perforating branches (medial mammary branches) from 2nd-4th intercostal spaces - largest contribution |
| Lateral thoracic artery (branch of axillary) | Lateral mammary branches |
| Thoracoacromial artery | Pectoral branches |
| Posterior intercostal arteries (2nd-5th) | Direct mammary branches |
| Superior thoracic artery | Direct branches |
Venous Drainage
The venous system parallels the arterial supply, draining into the internal thoracic veins and lateral thoracic veins. The venous plexus around the nipple (circulus venosus) communicates with the intercostal veins.
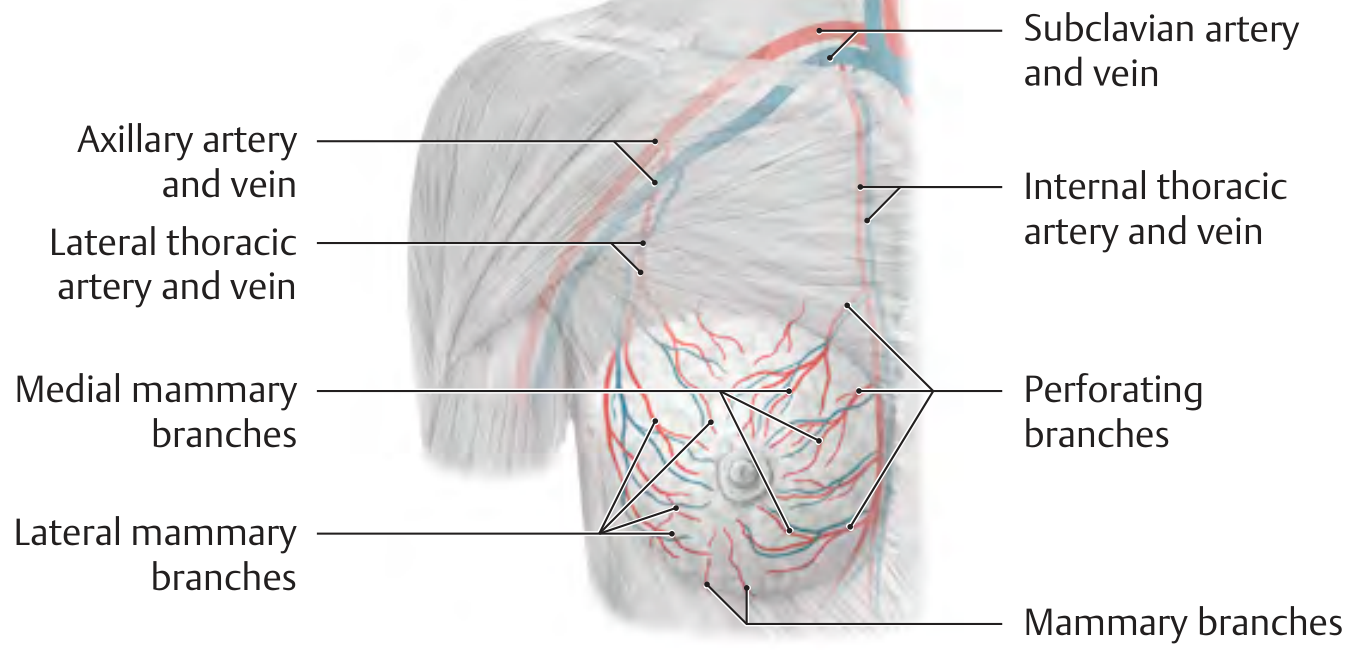
Blood supply to the breast (Thieme Atlas). Red = arteries; Blue = veins.
- Thieme Atlas of Anatomy, p. 229 | Fischer's, p. 3868
8. Nerve Supply
The sensory innervation has a segmental arrangement:
- Lateral and anterior cutaneous branches of intercostal nerves T2-T6 supply the majority of the breast
- Supraclavicular nerves (from the cervical plexus, C3-C4) supply the upper portion of the breast
- The 4th intercostal nerve (lateral branch) provides the primary sensory supply to the nipple
- Thieme Atlas, p. 229 | Fischer's, p. 3867
9. Lymphatic Drainage
The lymphatic flow is unidirectional through thin-walled, valveless vessels organized in three interconnecting plexuses:
- Primary (deep) plexus - within the gland along interlobular spaces and lactiferous ducts
- Subareolar plexus (Sappey's plexus) - drains skin, nipple/areola, and central breast
- Deep posterior plexus - on the deep surface, communicates with fascia
>75% of lymph drains to axillary nodes; the remainder drains to parasternal nodes. Flow to either group is independent of the quadrant of origin.
Axillary Lymph Node Levels (relative to pectoralis minor)
| Level | Location | Groups Included |
|---|---|---|
| Level I | Lateral/inferior to pectoralis minor | External mammary, axillary vein, subscapular (scapular) groups - ~30-60 nodes total |
| Level II | Posterior to (behind) pectoralis minor | Central nodes, some subclavicular nodes |
| Level III | Medial to pectoralis minor | Apical (subclavicular) nodes |
| Interpectoral (Rotter's) | Between pectoralis major and minor | Along the lateral pectoral nerve - part of Level II |
The supraclavicular nodes are contiguous with the apex of the axilla. The internal mammary (parasternal) nodes lie in the first six intercostal spaces within 3 cm of the sternal edge.
The sentinel lymph node (the first node in the axillary chain to receive drainage from the primary tumor) is most commonly found in the Level I external mammary group.
- Mulholland & Greenfield's Surgery, p. 3869-3870 | Sabiston, p. 1371
10. Upper Outer Quadrant - Clinical Significance
The upper outer quadrant of the breast contains the most parenchymal tissue (including the axillary tail) and is the most frequent site of both benign and malignant breast disease (~60% of all breast malignancies).
- Fischer's Mastery of Surgery, p. 3867
Summary Table
| Feature | Detail |
|---|---|
| Position | Ribs 2-6, sternal edge to midaxillary line |
| Overlying muscles | Pectoralis major (mainly), serratus anterior, ext. oblique |
| Lobes | 15-20 per breast |
| Lobules per lobe | 20-40 |
| Alveoli per lobule | 10-100 |
| Key functional unit | Terminal duct lobular unit (TDLU) |
| Main arterial supply | Internal thoracic artery (perforating branches) |
| Lymphatic drainage | >75% to axillary nodes |
| Sensory nerves | Intercostal T2-T6, supraclavicular (C3-C4) |
| Structural support | Cooper's ligaments (deep fascia to dermis) |
Anatomy of breast
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content needed from four authoritative textbooks. Here is the comprehensive answer:
Anatomy of the Breast
Sources: Sabiston Textbook of Surgery | Fischer's Mastery of Surgery (8th ed.) | Mulholland & Greenfield's Surgery (7th ed.) | Gray's Anatomy for Students | Thieme Atlas of Anatomy
1. Position and Surface Boundaries
The breast is located on the anterior thoracic wall, positioned between:
- Superior: 2nd rib
- Inferior: 6th rib
- Medial: Lateral border of the sternum
- Lateral: Midaxillary line
Posteriorly, it overlies the pectoralis major (upper and medial portions), serratus anterior (inferolateral portion), external abdominal oblique, and upper rectus sheath. A tongue of glandular tissue extends superlaterally around the lower border of the pectoralis major into the axilla - this is the axillary tail (process of Spence).
The average nonlactating breast weighs 150-225 g; the lactating breast may exceed 500 g. The left breast is commonly slightly larger than the right.
- Fischer's Mastery of Surgery, p. 3866 | Gray's Anatomy for Students, p. 274
2. Internal Structure - Cutaway View
Cutaway diagram of the mature resting breast (Sabiston Textbook of Surgery). The duct system is configured like an inverted tree, with larger ducts below the nipple branching into successively smaller peripheral ducts that terminate in lobules.
3. Structural Layers
The breast is composed of three layers from superficial to deep:
| Layer | Components |
|---|---|
| Skin | Thin, contains hair follicles, sebaceous glands, sweat glands |
| Subcutaneous tissue | Fat, cutaneous vessels, lymphatics, nerves |
| Breast parenchyma | Glandular epithelium + fibrous stroma + adipose tissue |
The breast lies between the subdermal adipose tissue anteriorly and the superficial pectoral fascia posteriorly. Behind it, a potential space called the retromammary space separates the breast from the deep pectoral fascia over the pectoralis major - this space is rich in lymphatics.
- Sabiston Textbook of Surgery, p. 1369
4. Glandular Architecture
The glandular apparatus is arranged like an inverted tree in a radial pattern spreading outward from the nipple-areolar complex (NAC):
Nipple (15-20 openings)
└── Lactiferous sinus (dilated segment below areola)
└── Lactiferous duct (one per lobe)
└── 15-20 Lobes
└── 20-40 Lobules per lobe
└── 10-100 Alveoli (acini) per lobule
└── Terminal Duct Lobular Unit (TDLU)
Key Points:
- 15-20 lobes per breast, each drained by a single lactiferous duct opening at the nipple
- Each duct has a dilated segment beneath the areola - the lactiferous sinus
- Each lobe divides into 20-40 lobules, each containing 10-100 acini
- The Terminal Duct Lobular Unit (TDLU) = one lobule + its terminal duct = the basic functional and secretory unit of the breast
- The TDLU is the site of origin of most malignant breast tumors (both ductal carcinoma in situ and invasive carcinoma)
- Intralobular stroma is loose connective tissue with capillaries and lymphocytes; interlobular stroma is denser and less cellular
- The duct wall has an inner epithelial layer and outer myoepithelial layer (contractile, propels milk toward nipple), surrounded by a continuous basement membrane (type IV collagen, laminin, proteoglycans)
- Breach of the basement membrane = invasive cancer
- Sabiston, p. 1369-1370 | Thieme Atlas, p. 229 | Fischer's, p. 3866
5. Cooper's Ligaments (Suspensory Ligaments)
Cooper's ligaments are fibrous connective tissue bands that run from the deep pectoral fascia through the breast parenchyma to the dermis, providing shape, support, and mobility to the breast.
Clinical significance: When infiltrated by cancer or stretched by edema, they produce skin dimpling and the classic "peau d'orange" (orange-skin) appearance of the breast surface.
- Sabiston, p. 1369 | Fischer's, p. 3866
6. Nipple-Areolar Complex (NAC)
- Skin is highly pigmented, composed of stratified squamous epithelium
- Deep to the NAC are smooth muscle bundles arranged radially, circumferentially, and longitudinally - these allow nipple erection
- Along the areolar margin: Montgomery glands (sebaceous/accessory glands) with nodular surface elevations called tubercles of Morgagni - these lubricate the nipple during lactation
- Nipple contains: free sensory nerve endings + Meissner corpuscles
- Areola contains: Ruffini-like endings + Krause end-bulbs
- Fischer's Mastery of Surgery, p. 3867
7. Blood Supply
Arterial Supply
| Artery | Contribution |
|---|---|
| Internal thoracic (mammary) artery | Perforating branches (medial mammary branches) from 2nd-4th intercostal spaces - the largest contributor |
| Lateral thoracic artery (branch of axillary) | Lateral mammary branches |
| Thoracoacromial artery (branch of axillary) | Pectoral branches |
| Posterior intercostal arteries 2nd-5th | Direct mammary branches |
| Superior thoracic artery | Direct branches |
Venous Drainage
Parallels the arterial supply - drains into the internal thoracic veins and lateral thoracic veins. The venous plexus around the nipple (circulus venosus) communicates with the intercostal veins and ultimately the vertebral plexus (Batson's plexus) - the latter is a route for hematogenous metastasis to the spine.
Blood supply to the breast (Thieme Atlas of Anatomy). Red = arteries; Blue = veins.
- Thieme Atlas, p. 229 | Fischer's, p. 3868
8. Nerve Supply
Sensory innervation has a segmental arrangement:
| Nerve | Area Supplied |
|---|---|
| Lateral cutaneous branches of T2-T6 intercostal nerves | Main supply to the lateral and central breast |
| Anterior cutaneous branches of T2-T6 intercostal nerves | Medial breast |
| Supraclavicular nerves (C3-C4) (from cervical plexus) | Upper portion of breast |
| 4th intercostal nerve (lateral branch) | Primary nipple sensation |
- Thieme Atlas, p. 229 | Fischer's, p. 3867
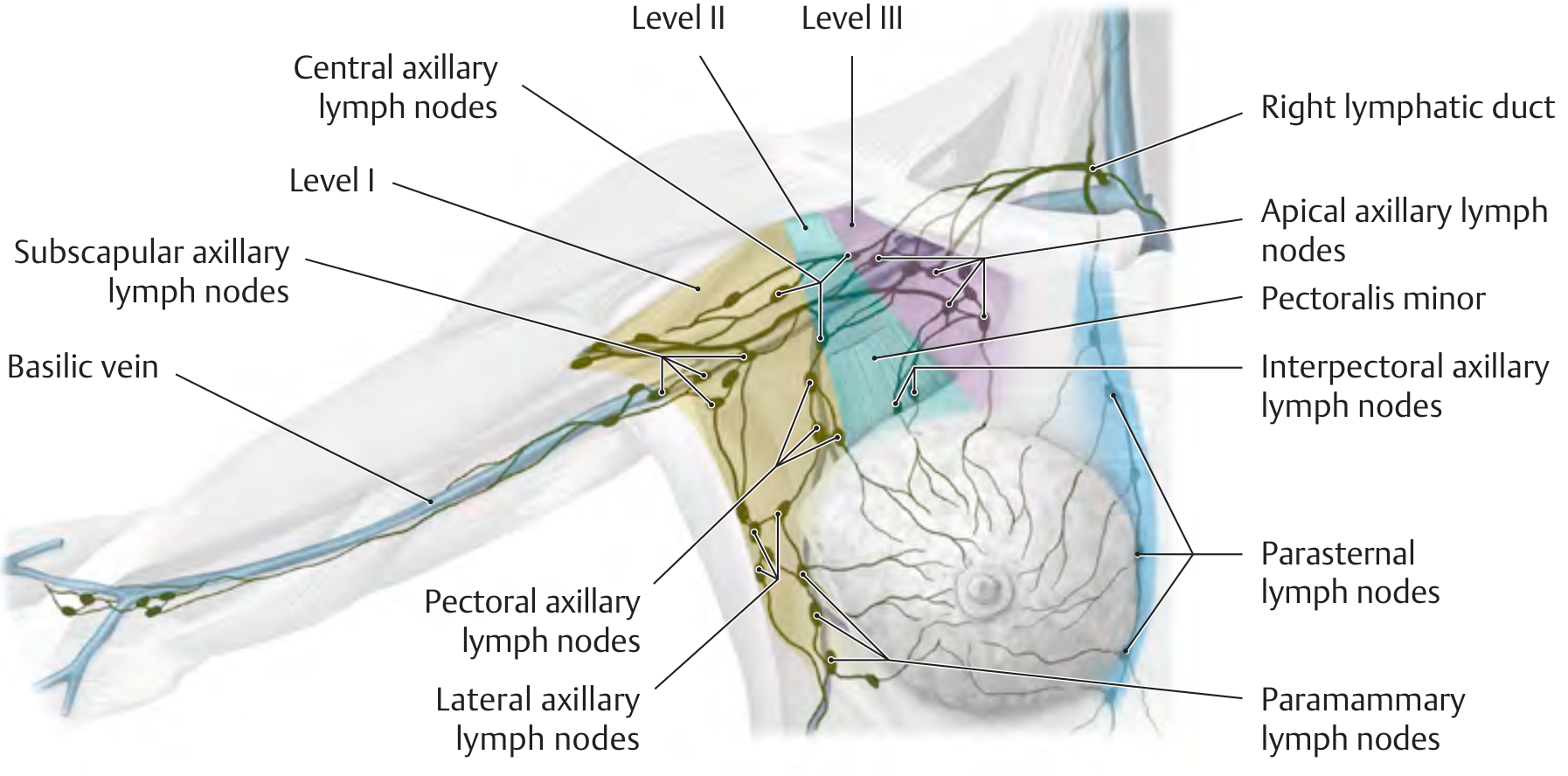
9. Lymphatic Drainage
Lymph flows unidirectionally through thin-walled, valveless vessels organized in three interconnecting plexuses:
- Deep (primary) plexus - within the gland along interlobular spaces and lactiferous ducts
- Subareolar plexus (Sappey's plexus) - drains skin, nipple, areola, and central breast; described by anatomist Sappey in 1885
- Deep posterior plexus - on the deep surface, communicates with vessels in the deep fascia
Distribution of drainage:
- 70-80% drains to axillary lymph nodes (primary route)
- ~20% drains to internal mammary (parasternal) nodes
- Flow to either group is independent of the quadrant of origin
Lymphatic drainage of the breast (Thieme Atlas). The axillary nodes are divided into three levels relative to pectoralis minor.
Axillary Lymph Node Levels (Berg's classification, relative to pectoralis minor)
| Level | Location | Groups Included |
|---|---|---|
| Level I | Lateral/inferior to pectoralis minor | External mammary, axillary vein, subscapular (scapular) groups |
| Level II | Posterior to pectoralis minor | Central nodes + interpectoral (Rotter's) nodes (between pectoralis major and minor) |
| Level III | Medial to pectoralis minor | Apical/infraclavicular nodes |
- The axilla contains ~30-60 nodes total
- Sentinel lymph node (SLN) = the first node in the axillary chain to receive drainage from a breast tumor - anatomically found most often in the Level I external mammary group
- Supraclavicular nodes are contiguous with the Level III apex and considered outside the formal axillary boundary
- Internal mammary nodes lie in intercostal spaces 1-6 within 3 cm of the sternal edge
- Mulholland & Greenfield's Surgery, p. 3869-3870 | Sabiston, p. 1371
10. Axillary Anatomy (Surgical Relevance)
The axilla is a pyramidal space with:
- Anterior wall: Pectoralis major + minor and associated fasciae
- Posterior wall: Subscapularis, teres major, latissimus dorsi
- Medial wall: Serratus anterior + upper 4-5 intercostal muscles
- Lateral wall: Bicipital groove of humerus
- Apex: Cervicoaxillary canal (bounded by clavicle, scapula, 1st rib)
- Base: Axillary fascia and skin
Key nerves preserved during axillary dissection: long thoracic nerve (serratus anterior - injury = winged scapula), thoracodorsal nerve (latissimus dorsi), medial pectoral nerve.
- Fischer's, p. 3869-3870
11. Clinical Notes - Upper Outer Quadrant
The upper outer quadrant contains the most breast parenchyma (including the axillary tail) and is the most frequent site of both benign disease and breast malignancies (~60% of all breast cancers arise here).
Summary Table
| Feature | Detail |
|---|---|
| Position | Ribs 2-6, sternum to midaxillary line |
| Axillary extension | Axillary tail (process of Spence) |
| Posterior relations | Pectoralis major, serratus anterior, ext. oblique |
| Lobes | 15-20 |
| Lobules per lobe | 20-40 |
| Acini per lobule | 10-100 |
| Basic functional unit | Terminal Duct Lobular Unit (TDLU) |
| Support ligaments | Cooper's ligaments (deep fascia to dermis) |
| Main arterial supply | Internal thoracic artery (perforating branches) |
| Venous drainage | Internal thoracic + lateral thoracic veins |
| Sensory nerves | Intercostal T2-T6 + supraclavicular C3-C4 |
| Primary lymph drainage | Axillary nodes (70-80%) |
| Secondary lymph drainage | Internal mammary nodes (~20%) |
| Cancer origin site | TDLU (terminal duct lobular unit) |
| Most common cancer quadrant | Upper outer quadrant (~60%) |
Lump vs swelling
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
lump vs swelling surgical clinical difference definition
Finding Sources
Searching the Web
lump vs swelling surgery clinical features differences pitting non-pitting
Reading Web Page
lump vs swelling definition difference clinical examination features
Now I have comprehensive information to deliver a thorough, well-structured answer.
Lump vs Swelling
This is a foundational concept in surgical clinical examination. The two terms are often used interchangeably in everyday language but have distinct meanings in surgery and clinical medicine.
Definitions
| Term | Definition |
|---|---|
| Lump | A discrete, palpable mass of body tissue - a localized, circumscribed abnormality that can be felt as a distinct entity with defined edges |
| Swelling | A vague, broader term denoting any enlargement or protuberance in the body due to any cause - includes edema (fluid accumulation in tissues), inflammation, or a localized mass |
| Tumour / Neoplasm | A growth of new cells that proliferate independent of the body's needs (either benign or malignant) |
In simple terms:
- All lumps are swellings, but not all swellings are lumps
- A lump implies a localized, distinct, usually solid or cystic mass
- A swelling can be diffuse, pitting (fluid-filled tissue spaces), or a discrete mass
Key Differences at a Glance
| Feature | Lump | Swelling |
|---|---|---|
| Definition | Discrete, circumscribed mass | Any enlargement/protuberance from any cause |
| Edges | Usually well-defined | May be ill-defined or diffuse |
| Nature | Solid, cystic, or mixed | Can be edematous (fluid in tissue), gaseous, or a mass |
| Pitting | Does not pit on pressure | Edematous swelling (e.g., pitting edema) pits on pressure |
| Examples | Lipoma, cyst, lymph node, abscess, tumour | Edema from heart failure, lymphedema, inflammatory swelling, a lipoma |
| Cause | Tissue proliferation, cyst, infection | Fluid accumulation, inflammation, tissue growth, trauma |
Types of Swelling
1. Edematous Swelling (fluid in interstitial tissue)
- Pitting edema - press with a finger for 5-10 seconds; a pit (indentation) remains
- Causes: congestive heart failure, nephrotic syndrome, hepatic cirrhosis, venous insufficiency, hypoalbuminemia
- Non-pitting edema - no pit on pressure; tissue feels firm/rubbery
- Causes: lymphedema (blockage of lymphatics), myxedema (hypothyroidism), lipedema
2. Inflammatory Swelling
- Hot, red, tender, with loss of function (the cardinal signs of inflammation - rubor, calor, dolor, tumor, functio laesa)
- Examples: abscess, cellulitis, acute lymphadenitis
3. Traumatic Swelling
- Hematoma, seroma, edema from injury
4. Neoplastic / True Lump
- Benign or malignant growth
- Usually discrete, firm-to-hard, with defined or irregular borders
Clinical Examination of a Lump/Swelling
A systematic approach ("the Ss") is used:
History
| Feature | Significance |
|---|---|
| Short duration + pain | Suggests acute inflammatory/infective cause |
| Long duration + no pain | Suggests benign neoplasm |
| Long duration + mild pain | Suggests chronic inflammatory swelling |
| Short duration + no pain | May suggest malignancy (rapid growth) |
| Mode of onset | Spontaneous, post-trauma, from existing lesion |
Inspection
- Site - anatomical location (quadrant, surface marking)
- Size - measured in cm (two dimensions)
- Shape - spherical, ovoid, irregular
- Surface - smooth, lobulated, irregular, nodular
- Skin over swelling - color, redness, dilated veins, punctum, scar, ulceration
- Edge / Margin - regular/irregular, well-defined/ill-defined
Palpation
| Feature | Method | Significance |
|---|---|---|
| Temperature | Dorsum of hand | Warm = inflammation/vascular |
| Tenderness | Gentle pressure | Acute inflammation, infection |
| Consistency | Squeeze/press | Soft, firm, hard, stony hard |
| Fluctuation | Two-finger test in two planes | Positive = fluid-filled (cyst, abscess) |
| Fluid thrill | Tap one side, feel the other | Large fluid swellings |
| Reducibility | Gentle pressure | Hernia reduces into body cavity |
| Compressibility | Press and release | Empties then refills (hemangioma, varicocele) |
| Pulsatility | Both hands | True pulsatile = aneurysm; transmitted = solid mass on vessel |
| Impulse on coughing | Ask to cough | Hernia; also varicocele impulse test |
| Fixity to skin | Pinch skin over lump | Fixed = cancer infiltrating skin |
| Fixity to deep structures | Move lump with muscle contracted vs. relaxed | Fixed to muscle = in/deep to it |
| Regional lymph nodes | Examine draining nodes | Infection, metastasis |
Percussion
- Resonant = gas-containing (bowel in hernia)
- Dull = solid or fluid-filled
Auscultation
- Bowel sounds over hernia = bowel within
- Bruit over swelling = arteriovenous malformation or vascular tumour
Transillumination
- Performed in a darkened room with a bright pencil torch
- Place torch behind the swelling, observe from the front
- Transilluminates (glows red) = clear fluid inside (hydrocele, cystic hygroma, epididymal cyst)
- Does not transilluminate = solid, blood-filled, or turbid fluid (abscess)
Distinguishing Solid vs. Cystic Lump
| Feature | Solid | Cystic (Fluid-filled) |
|---|---|---|
| Consistency | Firm / hard | Soft / fluctuant |
| Fluctuation | Negative | Positive (displacement in 2 planes) |
| Transillumination | Negative | Positive (if clear fluid) |
| Compression | Does not reduce | May reduce (compressible) |
Distinguishing Benign vs. Malignant Lump
| Feature | Benign | Malignant |
|---|---|---|
| Age | Any (usually younger) | Usually >40 years |
| Growth | Slow | Rapid |
| Pain | Usually painless | May be painful at late stage (osteosarcoma: painful from start) |
| Surface | Smooth | Irregular, nodular |
| Margin | Well-defined, smooth | Ill-defined, irregular |
| Consistency | Usually firm | Hard, stony hard |
| Mobility | Freely mobile | Fixed (to skin or deep structures) |
| Skin over lump | Normal | Tethered, dimpled, ulcerated, peau d'orange |
| Regional lymph nodes | Not enlarged | Enlarged, hard, matted |
| Metastasis | Absent | Present (distant spread) |
| Cachexia/weight loss | Absent | Present in advanced disease |
| Recurrence after removal | Rare | Common if incompletely excised |
Common Causes of a Lump by Content
| Type | Content | Examples |
|---|---|---|
| Solid | Tissue cells | Lipoma, fibroma, lymph node, carcinoma |
| Cystic | Clear serous fluid | Sebaceous cyst, ganglion, ovarian cyst, hydrocele |
| Abscess | Pus | Pyogenic abscess, collar stud abscess |
| Hematoma | Blood | Post-traumatic hematoma |
| Vascular | Blood under pressure | Aneurysm, hemangioma, AVM |
| Gaseous | Air/gas | Surgical emphysema, hernia with bowel |
Summary
A lump is a discrete, circumscribed mass of tissue. A swelling is any enlargement from any cause - it is a broader term encompassing both localized lumps and diffuse fluid accumulation (edema).
The clinical examination of any lump/swelling follows a systematic protocol: history (duration, pain, growth rate) → inspection (site, size, shape, skin) → palpation (consistency, fluctuation, reducibility, fixity, nodes) → special tests (transillumination, auscultation, percussion) → investigations (ultrasound, FNAC, biopsy).
This is a shared conversation. Sign in to Orris to start your own chat.