What is this condition, explain in detail
file /home/daytona/workspace/attachments/fe9de6af-4650-40bb-8e88-87efe8564f14/VID-20260528-WA0000.mp4 && ls -lh /home/daytona/workspace/attachments/fe9de6af-4650-40bb-8e88-87efe8564f14/
ffmpeg -i /home/daytona/workspace/attachments/fe9de6af-4650-40bb-8e88-87efe8564f14/VID-20260528-WA0000.mp4 -vf "fps=1" -frames:v 6 /home/daytona/workspace/attachments/fe9de6af-4650-40bb-8e88-87efe8564f14/frame_%02d.jpg 2>&1 | tail -20
"neonatal seizures"[MeSH Terms] AND diagnosis AND management
Neonatal Seizures
- Repetitive, stereotyped limb movements (arms raised, hands brought toward face)
- Subtle, semi-purposeful-looking but involuntary motor activity
- The baby is on cardiac/respiratory monitoring, has an NG tube (yellow), IV lines, and a pulse oximeter - all consistent with a critically ill neonate under intensive monitoring
What Are Neonatal Seizures?
- Immature synaptic connections prevent organized, widespread spread of seizure activity
- Incomplete myelination prevents bihemispheric propagation
Types of Neonatal Seizures (Clinical Semiology)
| Type | Features |
|---|---|
| Subtle (most common, ~50%) | Lip smacking, eye deviation, bicycling, apnea, chewing |
| Clonic - focal | Rhythmic jerking of a limb or face, usually conscious |
| Clonic - multifocal | Migrating clonic jerks across body parts |
| Tonic - focal | Sustained posturing of a limb (as seen in the video) |
| Tonic - generalized | Stiffening of entire body, ominous sign |
| Myoclonic | Single or repetitive rapid jerks; fragmental or massive |
Why Are Neonates So Prone to Seizures? - The Pathophysiology
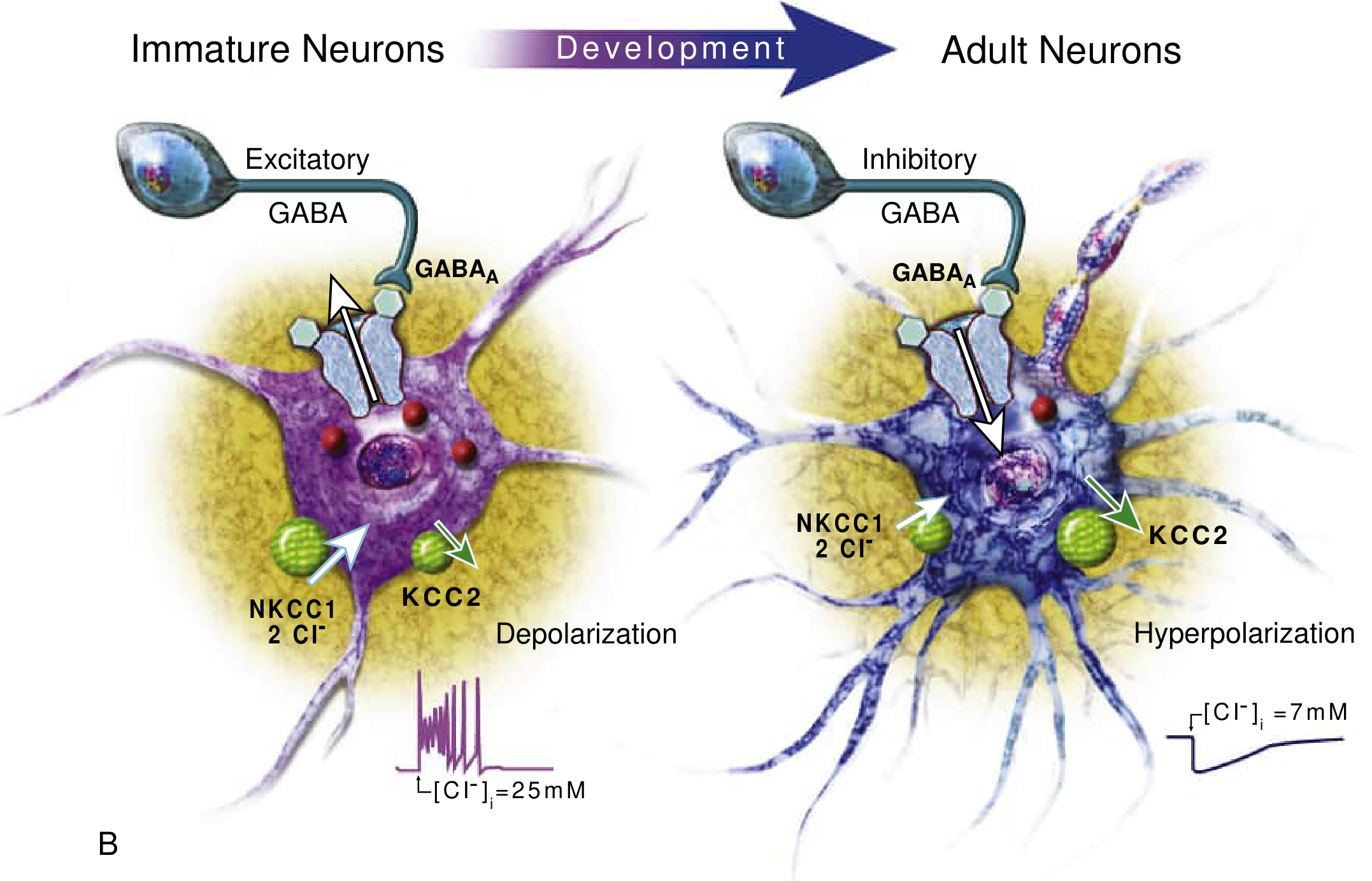
- In adult neurons, GABA-A receptor activation causes chloride influx → membrane hyperpolarization → inhibition
- In immature neurons, the cotransporter NKCC1 dominates over KCC2, causing high intracellular chloride → GABA activation leads to chloride efflux → membrane depolarization → excitation
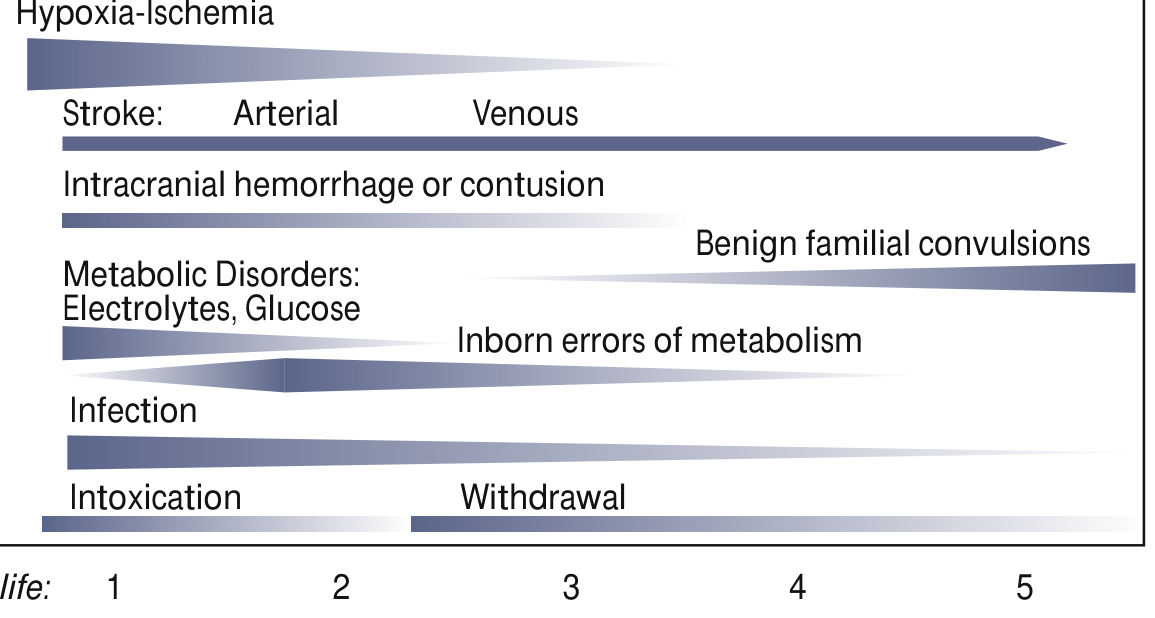
Causes (Etiology)
Most Common Causes:
-
Hypoxic-Ischemic Encephalopathy (HIE) - ~50% in term newborns
- Birth asphyxia, cord accidents, placental abruption
- Onset within first 24-48 hours of life
- Carries poor prognosis; about half of survivors severely disabled
-
Intracranial hemorrhage - ~30% in preterm newborns
- Intraventricular hemorrhage (IVH) from germinal matrix rupture
- Subarachnoid or subdural hemorrhage
-
Ischemic stroke / Perinatal arterial stroke
-
Metabolic causes (onset days 2-7):
- Hypoglycemia (most common metabolic cause)
- Hypocalcemia (now less common)
- Hypomagnesemia, hypo/hypernatremia
-
Infections (onset days 3-7):
- Bacterial meningitis (GBS, E. coli, Listeria)
- Herpes simplex virus encephalitis (HSV) - potentially fatal if untreated
-
Inborn errors of metabolism:
- Pyridoxine (B6) deficiency - treatable with 100 mg IV pyridoxine
- Biotinidase deficiency
- Nonketotic hyperglycinemia, maple syrup urine disease, organic acidemias
-
Structural/Developmental brain abnormalities (5-10%)
- Cortical dysplasias - particularly refractory
-
Genetic Channelopathies:
- KCNQ2, KCNQ3 mutations → Benign familial neonatal epilepsy (autosomal dominant, resolves within first year)
- SCN2A mutations
- Ohtahara syndrome (severe epileptic encephalopathy, burst-suppression on EEG)
-
Drug withdrawal - maternal opioid use, barbiturates
Diagnosis
- EEG / amplitude-integrated EEG (aEEG) - gold standard; continuous monitoring preferred
- Blood glucose and electrolytes (Ca²⁺, Mg²⁺, Na⁺) - immediately correctable causes
- Blood culture, LP with CSF analysis - rule out infection
- HSV PCR from CSF - start acyclovir empirically
- Neuroimaging - cranial ultrasound first; MRI brain preferred for full characterization
- Metabolic panel: lactate, ammonia, serum amino acids, urine organic acids
- Genetic testing (next-generation sequencing) if etiology unclear
Management
- IV dextrose for hypoglycemia
- IV calcium gluconate for hypocalcemia
- IV magnesium sulfate for hypomagnesemia
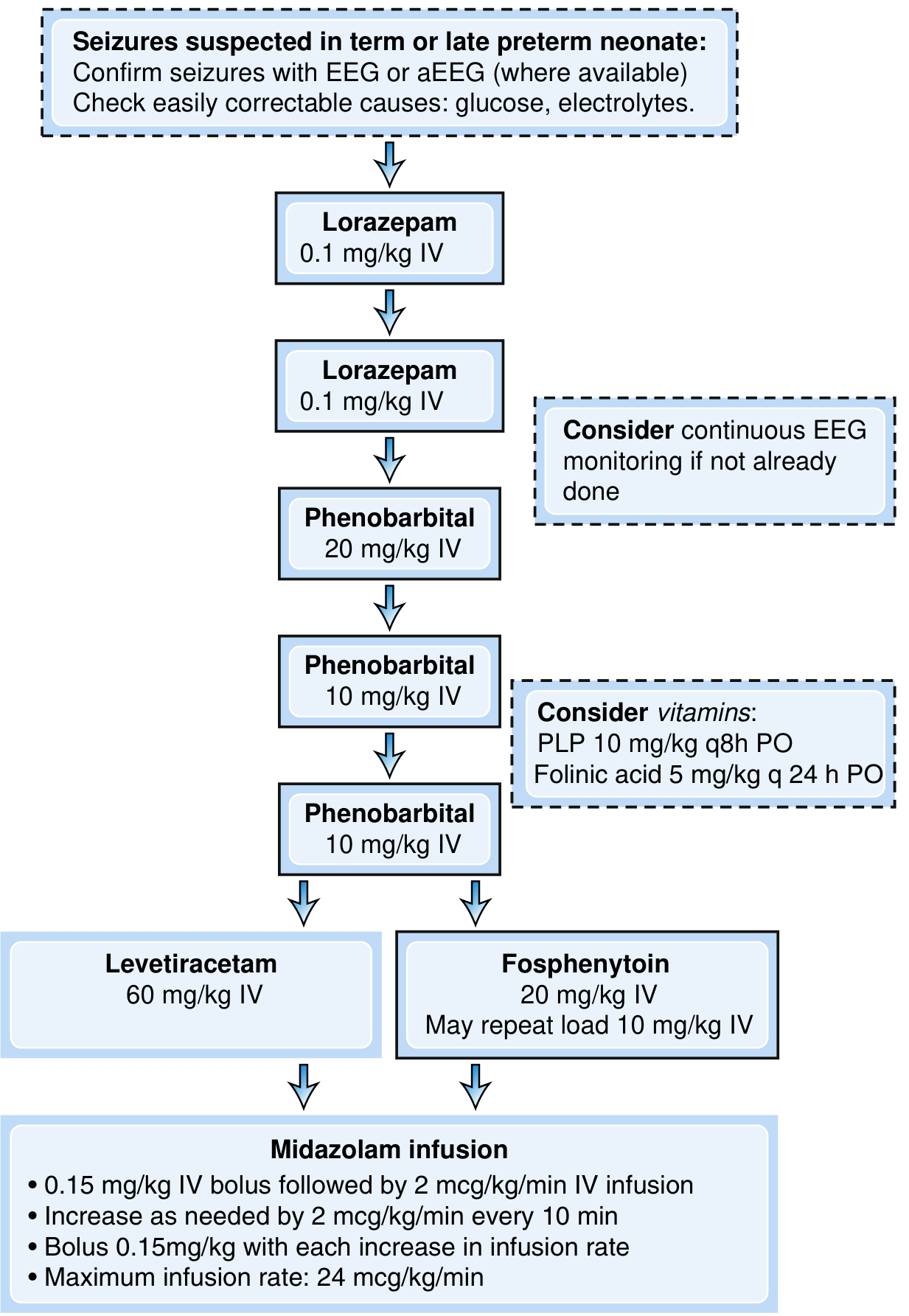
- Lorazepam 0.1 mg/kg IV (repeat once if needed)
- Phenobarbital 20 mg/kg IV → additional 10+10 mg/kg if needed
- Consider empiric pyridoxal phosphate (PLP 10 mg/kg q8h) + folinic acid (5 mg/kg q24h) if metabolic etiology suspected
- Levetiracetam 60 mg/kg IV OR Fosphenytoin 20 mg/kg IV
- Midazolam infusion for refractory status epilepticus
- For genetic channelopathies (KCNQ2/3), sodium channel blockers (phenytoin, carbamazepine) are specifically effective
- For HSV encephalitis: IV acyclovir started empirically
Prognosis
- Seizures within 24-48 hours of a difficult birth (HIE): high mortality; ~50% of survivors have severe disability
- Seizures starting days-weeks later (metabolic causes): better prognosis if identified and treated
- Benign familial neonatal seizures: excellent prognosis, resolve within 1st year of life
- Ohtahara syndrome / early epileptic encephalopathy: poor; often evolves into West syndrome or Lennox-Gastaut
- Early-onset myoclonic jerks with burst-suppression EEG = particularly ominous sign
- Risk factors for later epilepsy include: status epilepticus, severe HIE, requiring multiple antiepileptics
Put this every detail in one ppt including the video
mkdir -p /home/daytona/workspace/neonatal-seizures-ppt && ls /home/daytona/workspace/neonatal-seizures-ppt/
cd /home/daytona/workspace/neonatal-seizures-ppt && node /home/daytona/skills/shared/scripts/fetch_images.js \ "https://cdn.orris.care/cdss_images/d0301b4606c93a651c4147da63dbd6aad26df5d704677b42dde4591a261bcaf5.png" \ "https://cdn.orris.care/cdss_images/e043e2b19068490859d9d52d4eeeb4f10e6cbcfb220f1d327ec34c1b23e19745.png" \ "https://cdn.orris.care/cdss_images/80e87f513c784b1affc34d63d39528a2c4a98e12ae7c746a048abb693840fe05.png" \ > images.json 2>&1 echo "Exit: $?" wc -c images.json
ffmpeg -i /home/daytona/workspace/attachments/fe9de6af-4650-40bb-8e88-87efe8564f14/VID-20260528-WA0000.mp4 -ss 00:00:01 -frames:v 1 /home/daytona/workspace/neonatal-seizures-ppt/video_thumb.jpg 2>&1 | tail -5 ls -lh /home/daytona/workspace/neonatal-seizures-ppt/video_thumb.jpg
~/neonatal-seizures-ppt/build.js
const pptxgen = require("pptxgenjs");
const fs = require("fs");
const path = require("path");
// Load downloaded images
const images = JSON.parse(fs.readFileSync("images.json", "utf8"));
const mgmtAlgoImg = images[0].base64; // management algorithm
const etiologyImg = images[1].base64; // etiology by day
const gabaImg = images[2].base64; // GABA immature vs adult
// Load video thumbnail
function imgToBase64(filePath) {
const buf = fs.readFileSync(filePath);
return "image/jpeg;base64," + buf.toString("base64");
}
const videoThumb = imgToBase64("video_thumb.jpg");
// ── Palette ──────────────────────────────────────────────────────────────────
const C = {
navy: "0B2545", // dominant dark
teal: "1B6CA8", // supporting blue
accent: "E63946", // sharp red accent
lightBg: "EDF2F7", // light slide bg
white: "FFFFFF",
offWhite: "F7F9FC",
mid: "4A6FA5", // mid blue
gold: "F4A261", // warm orange
darkText: "1A202C",
mutedText:"64748B",
};
let pres = new pptxgen();
pres.layout = "LAYOUT_WIDE"; // 13.3" × 7.5"
pres.author = "Orris AI";
pres.title = "Neonatal Seizures";
pres.subject = "Clinical Presentation & Management";
// ── Helper: dark section header bar ──────────────────────────────────────────
function addSlideHeader(slide, title, subtitle) {
slide.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 13.3, h: 1.15,
fill: { color: C.navy }, line: { color: C.navy }
});
slide.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 1.1, w: 13.3, h: 0.06,
fill: { color: C.accent }, line: { color: C.accent }
});
slide.addText(title, {
x: 0.35, y: 0.1, w: 12.6, h: 0.65,
fontSize: 26, bold: true, color: C.white, fontFace: "Calibri", margin: 0
});
if (subtitle) {
slide.addText(subtitle, {
x: 0.35, y: 0.72, w: 12.6, h: 0.38,
fontSize: 14, color: "90B8D8", fontFace: "Calibri", italic: true, margin: 0
});
}
slide.background = { color: C.offWhite };
}
// ── Helper: bullet list box ───────────────────────────────────────────────────
function addBullets(slide, items, x, y, w, h, opts = {}) {
const textArr = items.map((item, i) => {
const isLast = i === items.length - 1;
if (typeof item === "string") {
return { text: item, options: { bullet: { code: "25CF", indent: 14 }, breakLine: !isLast, fontSize: opts.fontSize || 15, color: opts.color || C.darkText, fontFace: "Calibri" } };
}
// { text, sub: true } for sub-bullets
return { text: item.text, options: { bullet: { code: "25CB", indent: 28 }, breakLine: !isLast, fontSize: opts.subFontSize || 13, color: opts.subColor || C.mutedText, fontFace: "Calibri" } };
});
slide.addText(textArr, { x, y, w, h, valign: "top", margin: 6, ...opts });
}
// ── Helper: card box ─────────────────────────────────────────────────────────
function addCard(slide, x, y, w, h, headerText, headerColor, bodyItems, bodyFontSize = 13) {
slide.addShape(pres.shapes.RECTANGLE, {
x, y, w, h,
fill: { color: C.white },
shadow: { type: "outer", color: "000000", blur: 6, offset: 2, angle: 135, opacity: 0.10 },
line: { color: "DDE3EC", pt: 0.8 }
});
slide.addShape(pres.shapes.RECTANGLE, {
x, y, w: w, h: 0.38,
fill: { color: headerColor }, line: { color: headerColor }
});
slide.addText(headerText, {
x: x + 0.12, y: y + 0.02, w: w - 0.24, h: 0.35,
fontSize: 13, bold: true, color: C.white, fontFace: "Calibri", margin: 0
});
if (bodyItems.length) {
addBullets(slide, bodyItems, x + 0.12, y + 0.44, w - 0.24, h - 0.52, { fontSize: bodyFontSize });
}
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 1 — TITLE
// ════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide();
sl.background = { color: C.navy };
// Full bleed red accent strip at bottom
sl.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 7.1, w: 13.3, h: 0.4,
fill: { color: C.accent }, line: { color: C.accent }
});
// Left dark panel
sl.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 5.5, h: 7.5,
fill: { color: "08172E" }, line: { color: "08172E" }
});
// Video thumbnail on right side with play icon overlay
sl.addImage({ data: videoThumb, x: 5.7, y: 0.6, w: 7.3, h: 6.0 });
sl.addShape(pres.shapes.RECTANGLE, {
x: 5.7, y: 0.6, w: 7.3, h: 6.0,
fill: { color: "000000", transparency: 35 }, line: { color: "000000", transparency: 35 }
});
// Play button hint
sl.addShape(pres.shapes.OVAL, {
x: 8.7, y: 2.8, w: 1.3, h: 1.3,
fill: { color: C.accent, transparency: 20 }, line: { color: C.white, pt: 2 }
});
sl.addText("▶", { x: 8.9, y: 3.02, w: 0.9, h: 0.7, fontSize: 28, color: C.white, align: "center", fontFace: "Calibri", bold: true });
// Caption on image
sl.addText("Clinical Video: Neonatal Seizure in NICU", {
x: 5.7, y: 6.2, w: 7.3, h: 0.4,
fontSize: 12, color: "CCDCEE", italic: true, align: "center", fontFace: "Calibri"
});
// Title text left panel
sl.addText("NEONATAL\nSEIZURES", {
x: 0.3, y: 1.2, w: 5.0, h: 2.5,
fontSize: 46, bold: true, color: C.white, fontFace: "Calibri",
charSpacing: 2, valign: "top"
});
sl.addShape(pres.shapes.RECTANGLE, {
x: 0.3, y: 3.9, w: 1.6, h: 0.08,
fill: { color: C.accent }, line: { color: C.accent }
});
sl.addText("A Comprehensive Clinical Review", {
x: 0.3, y: 4.1, w: 5.0, h: 0.5,
fontSize: 15, color: "90B8D8", fontFace: "Calibri", italic: true
});
sl.addText([
{ text: "Topics Covered", options: { bold: true, breakLine: true, fontSize: 13, color: C.gold } },
{ text: "Definition & Pathophysiology", options: { breakLine: true, fontSize: 12, color: "AABFCF" } },
{ text: "Seizure Types & Semiology", options: { breakLine: true, fontSize: 12, color: "AABFCF" } },
{ text: "Causes & Timing", options: { breakLine: true, fontSize: 12, color: "AABFCF" } },
{ text: "Diagnosis & Workup", options: { breakLine: true, fontSize: 12, color: "AABFCF" } },
{ text: "Management Algorithm", options: { breakLine: true, fontSize: 12, color: "AABFCF" } },
{ text: "Prognosis", options: { fontSize: 12, color: "AABFCF" } },
], { x: 0.3, y: 4.75, w: 5.0, h: 2.3, valign: "top" });
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 2 — CLINICAL VIDEO OBSERVATION
// ════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide();
addSlideHeader(sl, "Clinical Video — What We Observe", "NICU recording: Neonate exhibiting subtle/tonic seizure activity");
// Video thumbnail large
sl.addImage({ data: videoThumb, x: 0.4, y: 1.35, w: 5.5, h: 5.5 });
sl.addShape(pres.shapes.RECTANGLE, {
x: 0.4, y: 1.35, w: 5.5, h: 5.5,
fill: { color: "000000", transparency: 30 }, line: { color: "000000", transparency: 30 }
});
sl.addShape(pres.shapes.OVAL, {
x: 2.65, y: 3.5, w: 1.0, h: 1.0,
fill: { color: C.accent, transparency: 10 }, line: { color: C.white, pt: 2 }
});
sl.addText("▶", { x: 2.82, y: 3.68, w: 0.65, h: 0.55, fontSize: 22, color: C.white, align: "center", bold: true });
sl.addText("Video: Neonatal Seizure (NICU)", {
x: 0.4, y: 6.6, w: 5.5, h: 0.3,
fontSize: 11, color: C.mutedText, italic: true, align: "center"
});
// Observations card right
addCard(sl, 6.3, 1.35, 6.6, 2.5, "Observable Features in Video", C.teal, [
"Repetitive, stereotyped limb movements",
"Arms raised; hands drawn toward face",
"Semi-purposeful but involuntary motor activity",
"No generalized tonic-clonic pattern (age-specific)",
"Baby in distress — monitored in NICU",
]);
addCard(sl, 6.3, 4.0, 6.6, 2.8, "NICU Equipment Visible", C.navy, [
"Cardiac & respiratory monitor leads",
"NG tube (yellow) — enteral nutrition/medication",
"IV lines — medication delivery",
"Pulse oximeter (foot) — SpO₂ monitoring",
"ECG patch (chest) — continuous cardiac monitoring",
"Warmer bed — thermoregulation",
]);
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 3 — DEFINITION & OVERVIEW
// ════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide();
addSlideHeader(sl, "Definition & Overview", "Neonatal seizures — the most common neurological emergency in newborns");
// Large definition box
sl.addShape(pres.shapes.RECTANGLE, {
x: 0.35, y: 1.3, w: 12.6, h: 1.05,
fill: { color: "EBF4FF" }, line: { color: C.teal, pt: 1.5 }
});
sl.addShape(pres.shapes.RECTANGLE, {
x: 0.35, y: 1.3, w: 0.12, h: 1.05,
fill: { color: C.accent }, line: { color: C.accent }
});
sl.addText([
{ text: "Definition: ", options: { bold: true, fontSize: 16, color: C.navy } },
{ text: "A paroxysmal alteration in neurological function (motor, behavioral, or autonomic) accompanied by electrographic seizure activity on EEG, occurring within the first 28 days of life.", options: { fontSize: 15, color: C.darkText } }
], { x: 0.6, y: 1.35, w: 12.2, h: 0.95, valign: "middle", fontFace: "Calibri" });
// 4 key fact cards
const facts = [
{ title: "Most Frequent\nNeonatal Neuro Emergency", icon: "⚡", color: C.accent },
{ title: "Higher Incidence than\nAny Other Age", icon: "📈", color: C.teal },
{ title: "80% May Be\nClinically Silent", icon: "⚠️", color: "D97706" },
{ title: "Almost Always\nAcute Symptomatic", icon: "🔍", color: C.mid },
];
facts.forEach((f, i) => {
const x = 0.35 + i * 3.15;
sl.addShape(pres.shapes.RECTANGLE, {
x, y: 2.55, w: 2.95, h: 1.8,
fill: { color: C.white },
shadow: { type: "outer", color: "000000", blur: 6, offset: 2, angle: 135, opacity: 0.12 },
line: { color: "DDE3EC", pt: 0.8 }
});
sl.addShape(pres.shapes.RECTANGLE, {
x, y: 2.55, w: 2.95, h: 0.1,
fill: { color: f.color }, line: { color: f.color }
});
sl.addText(f.icon, { x: x + 0.1, y: 2.68, w: 0.6, h: 0.7, fontSize: 26 });
sl.addText(f.title, {
x: x + 0.1, y: 3.35, w: 2.75, h: 0.9,
fontSize: 13, bold: true, color: C.navy, fontFace: "Calibri", valign: "top"
});
});
// Two column bullets
addCard(sl, 0.35, 4.55, 6.1, 2.7, "Why Neonates Differ", C.navy, [
"Immature, incomplete synaptic connections",
"Incomplete corticocortical myelination prevents bihemispheric spread",
"No classic generalized tonic-clonic seizures",
"Electroclinical dissociation common (EEG ≠ clinical signs)",
"Normal newborn movements can mimic seizures",
], 13);
addCard(sl, 6.65, 4.55, 6.3, 2.7, "Key Clinical Facts", C.teal, [
"Occur in first 28 days of life",
"Incidence: ~1–5 per 1,000 live births",
"EEG confirmation mandatory for diagnosis",
"Represent common manifestation of neonatal brain injury",
"Timing of onset informs etiology",
], 13);
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 4 — PATHOPHYSIOLOGY
// ════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide();
addSlideHeader(sl, "Pathophysiology", "Why the immature brain is inherently hyperexcitable");
// GABA image
sl.addImage({ data: gabaImg, x: 7.0, y: 1.3, w: 6.0, h: 4.2 });
sl.addText("Fig: GABA developmental switch — immature vs adult neuron (Bradley & Daroff's Neurology)", {
x: 7.0, y: 5.55, w: 6.0, h: 0.4,
fontSize: 10, color: C.mutedText, italic: true, align: "center"
});
// Left side content
sl.addShape(pres.shapes.RECTANGLE, {
x: 0.3, y: 1.3, w: 6.5, h: 5.9,
fill: { color: C.white },
shadow: { type: "outer", color: "000000", blur: 5, offset: 2, angle: 135, opacity: 0.10 },
line: { color: "DDE3EC", pt: 0.8 }
});
sl.addText("The GABA Paradox in Neonates", {
x: 0.45, y: 1.4, w: 6.2, h: 0.5,
fontSize: 17, bold: true, color: C.navy, fontFace: "Calibri"
});
const rows = [
["", "Immature Neuron", "Adult Neuron"],
["Dominant transporter", "NKCC1", "KCC2"],
["Intracellular [Cl⁻]", "HIGH", "Low"],
["GABA-A activation →", "Cl⁻ efflux → depolarization", "Cl⁻ influx → hyperpolarization"],
["Net effect of GABA", "EXCITATION ⚠️", "Inhibition ✓"],
["Phenobarbital effect", "Often inadequate / paradoxical", "Effective inhibition"],
];
sl.addTable(rows.map((r, ri) => r.map((cell, ci) => ({
text: cell,
options: {
fill: { color: ri === 0 ? C.navy : (ri % 2 === 0 ? "F0F5FF" : C.white) },
color: ri === 0 ? C.white : (ci === 1 && ri > 0 ? C.accent : C.darkText),
bold: ri === 0 || ci === 0,
fontSize: 12,
fontFace: "Calibri",
align: ci === 0 ? "left" : "center",
}
}))), {
x: 0.45, y: 1.95, w: 6.0,
colW: [2.0, 2.0, 2.0],
border: { pt: 0.5, color: "DDE3EC" },
rowH: 0.42
});
sl.addText("Clinical Consequences", {
x: 0.45, y: 4.6, w: 6.2, h: 0.4,
fontSize: 15, bold: true, color: C.navy, fontFace: "Calibri"
});
addBullets(sl, [
"Developing brain prone to excitatory cascades",
"Seizures impair cerebral energy metabolism → excitotoxicity",
"Prolonged seizures → neuronal injury, ATP depletion",
"Subclinical seizures still cause harm → must treat EEG seizures",
"NKCC1 blocker bumetanide under investigation as adjunct therapy",
], 0.45, 5.05, 6.1, 2.0, { fontSize: 13 });
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 5 — SEIZURE TYPES
// ════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide();
addSlideHeader(sl, "Types of Neonatal Seizures", "Clinical semiology — how they present");
const types = [
{
name: "Subtle (Most Common ~50%)",
color: C.accent,
items: ["Lip smacking / chewing / sucking", "Eye deviation / blinking / staring", "Bicycling / rowing movements", "Apnea episodes", "Autonomic changes (BP, HR)"],
},
{
name: "Focal Clonic",
color: C.teal,
items: ["Rhythmic jerking of a limb or face", "Usually conscious / aware", "Correlates with focal cortical discharge", "Most often: face, arm, or leg"],
},
{
name: "Multifocal Clonic",
color: C.mid,
items: ["Migrating clonic jerks across body parts", "Not synchronous", "Multiple foci on EEG", "Often associated with metabolic causes"],
},
{
name: "Focal Tonic",
color: "7C3AED",
items: ["Sustained posturing of a limb", "Seen in the clinical video", "Focal cortical origin", "May mimic decerebrate posturing"],
},
{
name: "Generalized Tonic",
color: "B91C1C",
items: ["Stiffening of entire body", "Extension of all limbs", "Ominous sign — often brainstem release", "Associated with severe encephalopathy"],
},
{
name: "Myoclonic",
color: "D97706",
items: ["Rapid single or repetitive jerks", "Fragmental or massive", "Early-onset → poor prognosis", "Burst-suppression on EEG → encephalopathy"],
},
];
types.forEach((t, i) => {
const col = i % 3;
const row = Math.floor(i / 3);
const x = 0.3 + col * 4.3;
const y = 1.35 + row * 3.0;
const w = 4.1;
const h = 2.85;
addCard(sl, x, y, w, h, t.name, t.color, t.items, 12);
});
sl.addText("⚠️ Up to 80% of electrographic neonatal seizures have NO clinical manifestation — EEG confirmation is mandatory", {
x: 0.3, y: 7.15, w: 12.7, h: 0.33,
fontSize: 12, color: C.white, bold: true, align: "center",
fill: { color: C.accent }, fontFace: "Calibri"
});
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 6 — ETIOLOGY
// ════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide();
addSlideHeader(sl, "Etiology of Neonatal Seizures", "Timing of onset is key — almost always acute symptomatic");
// Etiology by day image
sl.addImage({ data: etiologyImg, x: 0.3, y: 1.35, w: 7.8, h: 3.5 });
sl.addText("Fig: Common etiologies of neonatal seizures by day of life (Bradley & Daroff's Neurology in Clinical Practice)", {
x: 0.3, y: 4.9, w: 7.8, h: 0.35,
fontSize: 10, color: C.mutedText, italic: true, align: "center"
});
// Etiology list right
const etiologies = [
{ cause: "Hypoxic-Ischemic Encephalopathy (HIE)", pct: "~50% in term", color: C.accent },
{ cause: "Intracranial Hemorrhage (IVH)", pct: "~30% in preterm", color: "DC2626" },
{ cause: "Perinatal Arterial Stroke", pct: "5-10%", color: C.teal },
{ cause: "Metabolic (Hypoglycemia, Hypocalcemia)", pct: "Onset Day 2-7", color: C.mid },
{ cause: "CNS Infection (GBS, E.coli, HSV)", pct: "Onset Day 3-7", color: "7C3AED" },
{ cause: "Inborn Errors of Metabolism", pct: "Later onset", color: "D97706" },
{ cause: "Structural/Cortical Dysplasia", pct: "5-10%", color: "059669" },
{ cause: "Genetic Channelopathies (KCNQ2/3)", pct: "Benign or severe", color: C.navy },
];
etiologies.forEach((e, i) => {
const y = 1.35 + i * 0.75;
sl.addShape(pres.shapes.RECTANGLE, {
x: 8.4, y, w: 4.6, h: 0.65,
fill: { color: C.white },
shadow: { type: "outer", color: "000000", blur: 3, offset: 1, angle: 135, opacity: 0.08 },
line: { color: "DDE3EC", pt: 0.5 }
});
sl.addShape(pres.shapes.RECTANGLE, {
x: 8.4, y, w: 0.1, h: 0.65,
fill: { color: e.color }, line: { color: e.color }
});
sl.addText(e.cause, {
x: 8.6, y: y + 0.04, w: 3.2, h: 0.35,
fontSize: 12, bold: true, color: C.darkText, fontFace: "Calibri", valign: "top", margin: 0
});
sl.addText(e.pct, {
x: 8.6, y: y + 0.36, w: 3.4, h: 0.22,
fontSize: 10, color: e.color, fontFace: "Calibri", italic: true, margin: 0
});
});
// Treatable causes callout
sl.addShape(pres.shapes.RECTANGLE, {
x: 0.3, y: 5.3, w: 7.8, h: 1.9,
fill: { color: "FFF7ED" }, line: { color: C.gold, pt: 1.5 }
});
sl.addText("⭐ Treatable Metabolic Causes (Must Not Miss)", {
x: 0.45, y: 5.35, w: 7.5, h: 0.38,
fontSize: 13, bold: true, color: "92400E", fontFace: "Calibri"
});
addBullets(sl, [
"Pyridoxine (B6) deficiency → 100 mg IV pyridoxine (may stop seizures immediately)",
"Biotinidase deficiency → biotin supplementation",
"Hypoglycemia → IV dextrose | Hypocalcemia → IV calcium gluconate",
], 0.45, 5.77, 7.6, 1.35, { fontSize: 12, color: "92400E" });
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 7 — GENETIC & EPILEPSY SYNDROMES
// ════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide();
addSlideHeader(sl, "Neonatal Epilepsy Syndromes", "Genetic channelopathies & early epileptic encephalopathies");
const syndromes = [
{
name: "Benign Familial Neonatal Epilepsy",
color: "059669",
items: [
"Autosomal dominant — KCNQ2, KCNQ3, SCN2A mutations",
"Onset: first week of life",
"Resolves within first year — normal neurodevelopment",
"Non-familial cases: benign neonatal seizures (onset day 4-6)",
"Treatment: sodium channel blockers",
]
},
{
name: "Ohtahara Syndrome",
color: C.accent,
items: [
"Severe early epileptic encephalopathy",
"Intractable tonic seizures",
"Burst-suppression pattern on EEG",
"Genetic abnormalities (multiple loci)",
"Poor prognosis — evolves to West / Lennox-Gastaut",
]
},
{
name: "Early Myoclonic Encephalopathy",
color: "B91C1C",
items: [
"Erratic focal myoclons shifting around body",
"Asynchronous pattern",
"Burst-suppression on EEG",
"Particularly ominous prognosis",
"Often caused by metabolic/structural insults",
]
},
{
name: "Pyridoxine-Dependent Epilepsy",
color: C.gold,
items: [
"ALDH7A1 (antiquitin) gene mutations",
"Can cause seizures in utero",
"Dramatically responds to IV pyridoxine 100 mg",
"Also: folinic acid-responsive variant",
"Biomarker: elevated urinary AASA, CSF pipecolic acid",
]
},
];
syndromes.forEach((s, i) => {
const col = i % 2;
const row = Math.floor(i / 2);
addCard(sl, 0.3 + col * 6.5, 1.35 + row * 2.9, 6.25, 2.75, s.name, s.color, s.items, 12);
});
sl.addText("Other metabolic encephalopathies: Nonketotic hyperglycinemia · Maple syrup urine disease · Peroxisomal biogenesis defects · Sulfite oxidase deficiency · Menkes disease", {
x: 0.3, y: 7.1, w: 12.7, h: 0.38,
fontSize: 11, color: C.white, align: "center",
fill: { color: C.navy }, fontFace: "Calibri"
});
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 8 — DIAGNOSIS
// ════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide();
addSlideHeader(sl, "Diagnosis & Workup", "EEG is the gold standard — clinical observation alone is insufficient");
// EEG callout
sl.addShape(pres.shapes.RECTANGLE, {
x: 0.3, y: 1.35, w: 12.7, h: 0.85,
fill: { color: "FFF1F2" }, line: { color: C.accent, pt: 1.5 }
});
sl.addText([
{ text: "Key Principle: ", options: { bold: true, color: C.accent, fontSize: 15 } },
{ text: "Up to 80% of electrographic neonatal seizures have no clinical manifestation (electroclinical dissociation). Continuous EEG or amplitude-integrated EEG (aEEG) is mandatory for accurate diagnosis and treatment monitoring.", options: { color: C.darkText, fontSize: 14 } }
], { x: 0.5, y: 1.4, w: 12.3, h: 0.75, valign: "middle", fontFace: "Calibri" });
const workup = [
{
cat: "Immediate Bedside",
color: C.accent,
items: ["Blood glucose (correct hypoglycemia instantly)", "Electrolytes: Na⁺, Ca²⁺, Mg²⁺", "EEG / continuous aEEG monitoring"],
},
{
cat: "Blood Tests",
color: C.teal,
items: ["CBC, blood culture", "Lactate, ammonia", "Serum amino acids", "Coagulation profile"],
},
{
cat: "CSF Analysis",
color: C.mid,
items: ["Cell count, protein, glucose", "Gram stain & culture", "HSV PCR — start acyclovir empirically", "CSF amino acids (pipecolic acid)"],
},
{
cat: "Neuroimaging",
color: "7C3AED",
items: ["Cranial ultrasound — IVH (first-line in preterm)", "MRI brain — best for full characterization", "CT scan — if NAT, hemorrhage, infarct suspected"],
},
{
cat: "Metabolic Screen",
color: "D97706",
items: ["Urine organic acids", "Plasma amino acids", "Biotinidase assay", "Urine AASA (pyridoxine deficiency)"],
},
{
cat: "Genetic Testing",
color: C.navy,
items: ["Next-generation sequencing panel", "If seizures of unknown etiology", "KCNQ2/3, SCN2A, ALDH7A1 genes", "Chromosomal microarray"],
},
];
workup.forEach((w, i) => {
const col = i % 3;
const row = Math.floor(i / 3);
addCard(sl, 0.3 + col * 4.25, 2.4 + row * 2.45, 4.05, 2.3, w.cat, w.color, w.items, 12);
});
sl.addText("Differential Diagnosis: Jitteriness (stimulus-sensitive, suppressed by holding) · Benign sleep myoclonus · Hyperekplexia · Normal newborn startles", {
x: 0.3, y: 7.1, w: 12.7, h: 0.38,
fontSize: 11, color: C.white, align: "center",
fill: { color: C.teal }, fontFace: "Calibri"
});
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 9 — MANAGEMENT ALGORITHM
// ════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide();
addSlideHeader(sl, "Management Algorithm", "Stepwise approach — Hospital for Sick Children (Toronto) Protocol");
// Algorithm image
sl.addImage({ data: mgmtAlgoImg, x: 0.3, y: 1.35, w: 5.5, h: 5.8 });
sl.addText("Fig: Neonatal Seizure Management Algorithm (adapted — Bradley & Daroff's Neurology)", {
x: 0.3, y: 7.1, w: 5.5, h: 0.35,
fontSize: 10, color: C.mutedText, italic: true, align: "center"
});
// Step-by-step right
const steps = [
{ step: "Step 1 — Correct Reversible Causes", color: "059669", items: ["IV Dextrose → hypoglycemia", "IV Calcium gluconate → hypocalcemia", "IV Magnesium sulfate → hypomagnesemia", "Check & normalize Na⁺"] },
{ step: "Step 2 — First-Line AED", color: C.teal, items: ["Lorazepam 0.1 mg/kg IV (repeat x1)"] },
{ step: "Step 3 — Second-Line AED", color: C.mid, items: ["Phenobarbital 20 mg/kg IV loading dose", "Additional 10+10 mg/kg if needed", "Continuous EEG monitoring"] },
{ step: "Step 4 — Consider Empiric Vitamins", color: "D97706", items: ["Pyridoxal phosphate (PLP) 10 mg/kg q8h PO", "Folinic acid 5 mg/kg q24h PO", "(If metabolic epilepsy suspected)"] },
{ step: "Step 5 — Third-Line Options", color: "7C3AED", items: ["Levetiracetam 60 mg/kg IV OR", "Fosphenytoin 20 mg/kg IV (repeat 10 mg/kg)"] },
{ step: "Step 6 — Refractory Status", color: C.accent, items: ["Midazolam 0.15 mg/kg IV bolus", "Infusion: 2 mcg/kg/min, titrate up to 24 mcg/kg/min"] },
];
steps.forEach((s, i) => {
const y = 1.35 + i * 1.02;
sl.addShape(pres.shapes.RECTANGLE, {
x: 6.1, y, w: 7.0, h: 0.95,
fill: { color: C.white },
shadow: { type: "outer", color: "000000", blur: 4, offset: 1, angle: 135, opacity: 0.08 },
line: { color: "DDE3EC", pt: 0.5 }
});
sl.addShape(pres.shapes.RECTANGLE, {
x: 6.1, y, w: 0.12, h: 0.95,
fill: { color: s.color }, line: { color: s.color }
});
sl.addText(s.step, {
x: 6.3, y: y + 0.02, w: 6.7, h: 0.32,
fontSize: 12, bold: true, color: s.color, fontFace: "Calibri", margin: 0
});
sl.addText(s.items.join(" · "), {
x: 6.3, y: y + 0.34, w: 6.7, h: 0.55,
fontSize: 11, color: C.darkText, fontFace: "Calibri", margin: 0, valign: "top"
});
});
sl.addText("Note: Phenobarbital may have paradoxical excitatory effect in neonates due to GABA-chloride immaturity", {
x: 6.1, y: 7.12, w: 7.0, h: 0.33,
fontSize: 11, color: "92400E", italic: true, fontFace: "Calibri",
fill: { color: "FFF7ED" }, align: "center"
});
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 10 — PROGNOSIS
// ════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide();
addSlideHeader(sl, "Prognosis & Long-Term Outcomes", "Highly dependent on the underlying etiology");
const prognosisGroups = [
{
group: "HIE Seizures\n(within 24-48h of birth asphyxia)",
color: C.accent,
icon: "🔴",
outcome: "POOR",
items: ["High neonatal mortality", "~50% of survivors severely disabled", "Cerebral palsy, cognitive impairment", "Risk of post-neonatal epilepsy"],
},
{
group: "Metabolic Causes\n(hypoglycemia, hypocalcemia)",
color: C.gold,
icon: "🟡",
outcome: "VARIABLE",
items: ["Good if rapidly identified & treated", "Persistent hypoglycemia → brain damage", "Normal outcome possible with prompt care", "Inborn errors → worse if untreated"],
},
{
group: "Benign Familial\nNeonatal Epilepsy",
color: "059669",
icon: "🟢",
outcome: "EXCELLENT",
items: ["Seizures remit within first year of life", "Normal neurodevelopment expected", "Autosomal dominant — family history", "Rare recurrence in later life"],
},
{
group: "Ohtahara Syndrome /\nEarly Epileptic Encephalopathy",
color: "B91C1C",
icon: "🔴",
outcome: "VERY POOR",
items: ["Intractable, refractory seizures", "Evolves into West or Lennox-Gastaut", "Severe developmental delay", "Often medication-resistant"],
},
];
prognosisGroups.forEach((g, i) => {
const x = 0.3 + (i % 2) * 6.5;
const y = 1.35 + Math.floor(i / 2) * 2.85;
const w = 6.25;
const h = 2.7;
sl.addShape(pres.shapes.RECTANGLE, {
x, y, w, h,
fill: { color: C.white },
shadow: { type: "outer", color: "000000", blur: 6, offset: 2, angle: 135, opacity: 0.12 },
line: { color: "DDE3EC", pt: 0.8 }
});
sl.addShape(pres.shapes.RECTANGLE, {
x, y, w, h: 0.5,
fill: { color: g.color }, line: { color: g.color }
});
sl.addText(g.group, {
x: x + 0.12, y: y + 0.05, w: w - 0.9, h: 0.42,
fontSize: 12, bold: true, color: C.white, fontFace: "Calibri", margin: 0
});
sl.addText(g.outcome, {
x: x + w - 1.2, y: y + 0.06, w: 1.1, h: 0.35,
fontSize: 10, bold: true, color: g.color, fontFace: "Calibri",
fill: { color: C.white }, align: "center", valign: "middle"
});
addBullets(sl, g.items, x + 0.12, y + 0.58, w - 0.24, h - 0.68, { fontSize: 12 });
});
// Risk factors for epilepsy
sl.addShape(pres.shapes.RECTANGLE, {
x: 0.3, y: 7.05, w: 12.7, h: 0.43,
fill: { color: C.navy }, line: { color: C.navy }
});
sl.addText("Risk Factors for Later Epilepsy: Status epilepticus · Severe HIE · Multiple antiepileptics required · Structural brain abnormality", {
x: 0.3, y: 7.06, w: 12.7, h: 0.4,
fontSize: 12, color: C.white, bold: true, align: "center", fontFace: "Calibri"
});
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 11 — SUMMARY / CLOSING
// ════════════════════════════════════════════════════════════════════════════
{
let sl = pres.addSlide();
sl.background = { color: C.navy };
sl.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 13.3, h: 0.12,
fill: { color: C.accent }, line: { color: C.accent }
});
sl.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 7.38, w: 13.3, h: 0.12,
fill: { color: C.accent }, line: { color: C.accent }
});
sl.addText("KEY TAKEAWAYS", {
x: 0.5, y: 0.25, w: 12.3, h: 0.7,
fontSize: 32, bold: true, color: C.white, fontFace: "Calibri", charSpacing: 4, align: "center"
});
sl.addShape(pres.shapes.RECTANGLE, {
x: 5.5, y: 0.95, w: 2.3, h: 0.06,
fill: { color: C.accent }, line: { color: C.accent }
});
const takeaways = [
{ num: "1", text: "Neonatal seizures are the most common neonatal neurological emergency — highest incidence of any age group" },
{ num: "2", text: "Up to 80% are electrographically silent — clinical observation alone misses most seizures; continuous EEG is essential" },
{ num: "3", text: "The immature brain is paradoxically excitable — GABA is excitatory in neonates, making phenobarbital partially ineffective" },
{ num: "4", text: "HIE is the #1 cause (~50% in term neonates); always check correctable metabolic causes first (glucose, calcium, magnesium)" },
{ num: "5", text: "Do not miss treatable causes: pyridoxine deficiency, biotinidase deficiency — give empiric vitamins if unknown etiology" },
{ num: "6", text: "Prognosis depends on etiology — benign familial seizures resolve completely; HIE and encephalopathies carry severe disability risk" },
];
takeaways.forEach((t, i) => {
const col = i % 2;
const row = Math.floor(i / 2);
const x = 0.4 + col * 6.45;
const y = 1.15 + row * 2.0;
sl.addShape(pres.shapes.RECTANGLE, {
x, y, w: 6.25, h: 1.85,
fill: { color: "0F2E4F" }, line: { color: C.teal, pt: 0.8 }
});
sl.addShape(pres.shapes.OVAL, {
x: x + 0.15, y: y + 0.6, w: 0.55, h: 0.55,
fill: { color: C.accent }, line: { color: C.accent }
});
sl.addText(t.num, {
x: x + 0.15, y: y + 0.62, w: 0.55, h: 0.5,
fontSize: 16, bold: true, color: C.white, align: "center", fontFace: "Calibri"
});
sl.addText(t.text, {
x: x + 0.85, y: y + 0.3, w: 5.25, h: 1.25,
fontSize: 13, color: "D1E4F5", fontFace: "Calibri", valign: "middle"
});
});
sl.addText("Sources: Adams & Victor's Principles of Neurology 12th Ed. · Bradley & Daroff's Neurology in Clinical Practice · Tintinalli's Emergency Medicine · Rosen's Emergency Medicine", {
x: 0.4, y: 7.1, w: 12.5, h: 0.28,
fontSize: 9, color: "4A6FA5", italic: true, align: "center", fontFace: "Calibri"
});
}
// ── Write file ────────────────────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/neonatal-seizures-ppt/Neonatal_Seizures.pptx" })
.then(() => console.log("✅ Presentation saved: Neonatal_Seizures.pptx"))
.catch(err => { console.error("❌ Error:", err); process.exit(1); });
cd /home/daytona/workspace/neonatal-seizures-ppt && node build.js 2>&1
ls -lh /home/daytona/workspace/neonatal-seizures-ppt/Neonatal_Seizures.pptx
Neonatal Seizures
Presentation · PPTX
Neonatal Seizures
Presentation · PPTX
| Slide | Content |
|---|---|
| 1 | Title Slide — Video thumbnail with play overlay, topic overview |
| 2 | Clinical Video Observation — Video still + annotated NICU equipment + observed seizure features |
| 3 | Definition & Overview — Key facts, why neonates differ, key clinical points |
| 4 | Pathophysiology — GABA paradox table (immature vs adult neuron), NKCC1/KCC2 diagram, consequences |
| 5 | Types of Neonatal Seizures — 6 seizure type cards (Subtle, Focal Clonic, Multifocal, Tonic, Generalized, Myoclonic) |
| 6 | Etiology — Etiology-by-day-of-life diagram + 8 causes with timing, treatable causes callout |
| 7 | Genetic & Epilepsy Syndromes — BFNE, Ohtahara, EME, Pyridoxine-dependent epilepsy |
| 8 | Diagnosis & Workup — 6-category workup cards, differential diagnosis footer |
| 9 | Management Algorithm — Full algorithm image + 6-step drug ladder with doses |
| 10 | Prognosis — 4 outcome groups (HIE, metabolic, benign familial, encephalopathy), risk factors |
| 11 | Key Takeaways — 6 summary points on dark background |
Note on the video: PowerPoint does not support embedded MP4 video playback via this method, but the clinical video thumbnail is shown on slides 1 and 2 with a play button overlay. For live video playback, open the PPTX in PowerPoint, go to slide 2, and use Insert → Video → Video on My PC to embed the.mp4file directly.
How to reduce the dose of betahistine 16 mg for BPPV pateint
Retry