DIAPHRAGM ANATOMY AND ANAESTHETIC IMPLICATIONS
Reading File
Finding Sources
Finding Sources
Searching the Web
diaphragm anatomy anaesthetic implications phrenic nerve block 2024
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
I now have comprehensive material to write a detailed, well-illustrated answer. Let me compile the full response:
Diaphragm Anatomy and Anaesthetic Implications
1. Overview
The diaphragm is a dome-shaped musculotendinous sheet that serves as the floor of the thoracic cavity and the roof of the abdominal cavity. It is the primary muscle of inspiration, responsible for roughly 70-80% of the tidal volume during quiet breathing. Its anatomy has profound implications for regional anaesthesia, mechanical ventilation, abdominal surgery, and laparoscopy.
2. Structural Anatomy
2.1 General Structure
The diaphragm consists of a central tendinous part (the central tendon) into which peripherally arranged muscle fibers converge. The pericardium attaches firmly to the middle part of the central tendon.
"The diaphragm is a thin musculotendinous structure that fills the inferior thoracic aperture and separates the thoracic cavity from the abdominal cavity."
- Gray's Anatomy for Students
2.2 Peripheral Attachments
The diaphragm attaches peripherally to:
- Anteriorly: Xiphoid process of the sternum
- Laterally: Costal margins of ribs VII-XII; ends of ribs XI and XII
- Posteriorly: Arcuate ligaments and lumbar vertebrae via the crura
2.3 The Crura
Two muscular extensions (crura) anchor the diaphragm to the vertebral column and blend with the anterior longitudinal ligament:
- Right crus: Largest and broadest; attaches to vertebral bodies LI-LIII and intervening discs
- Left crus: Attaches to vertebral bodies LI-LII and the associated intervertebral disc
The crura connect across the midline via the median arcuate ligament, which passes anterior to the aorta.
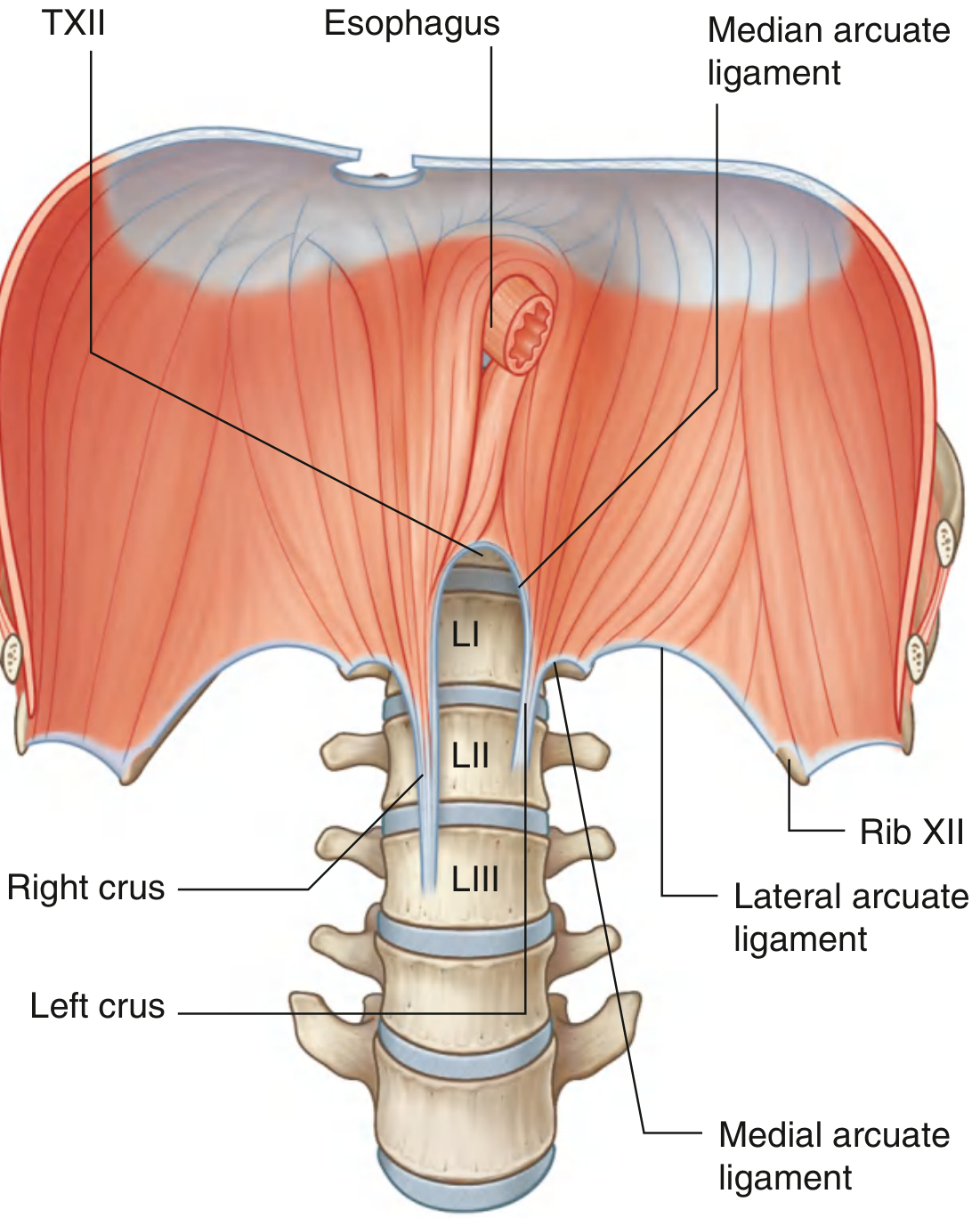
2.4 The Three Arcuate Ligaments
| Ligament | Spans | Attachment |
|---|---|---|
| Median arcuate | Crosses aorta | Between the two crura |
| Medial arcuate | Covers psoas major | Vertebral body LI/LII to transverse process LI |
| Lateral arcuate | Covers quadratus lumborum | Transverse process LI to rib XII |
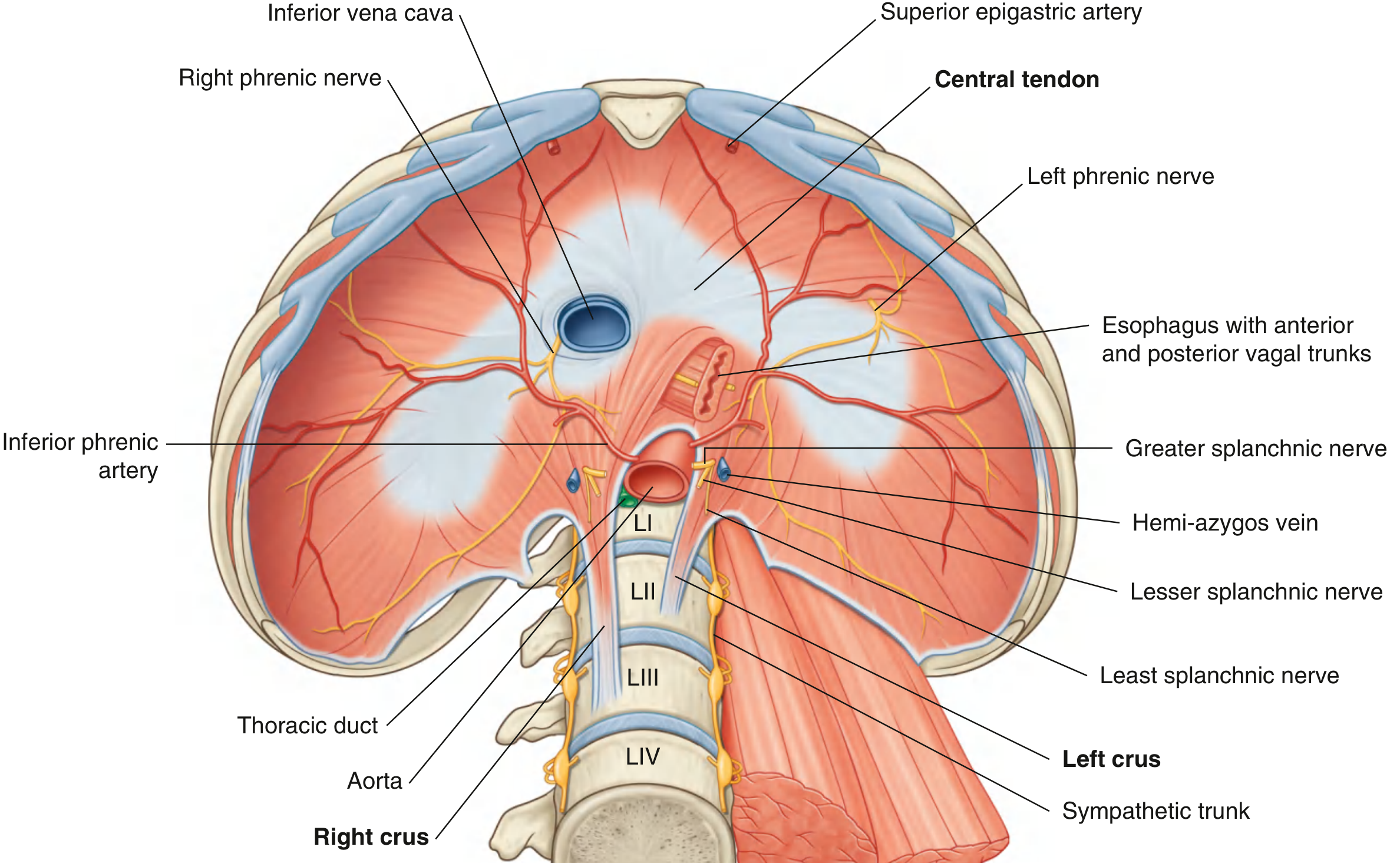
3. The Three Major Diaphragmatic Openings
Three major structures (and their companions) traverse the diaphragm through distinct openings. The mnemonic "I 8 10 eggs AT 12" aids recall of the vertebral levels:
| Opening | Vertebral Level | Structures Passing Through |
|---|---|---|
| Caval (IVC) opening | T8 (in central tendon) | Inferior vena cava; right phrenic nerve |
| Oesophageal hiatus | T10 (in muscular part, left of midline) | Oesophagus; vagus nerves (anterior and posterior trunks); oesophageal branches of left gastric artery and vein |
| Aortic hiatus | T12 (behind diaphragm, between crura) | Aorta; thoracic duct; sometimes azygos/hemiazygos veins |
Additional structures passing outside the main openings:
- Sympathetic trunks pass posterior to the medial arcuate ligament
- Greater, lesser, and least splanchnic nerves penetrate the crura
- Hemiazygos vein may pass through the left crus
"The azygos and hemiazygos veins may also pass through the aortic hiatus or through the crura of the diaphragm. Other structures outside the posterior attachments of the diaphragm lateral to the aortic hiatus include the sympathetic trunks. The greater, lesser, and least splanchnic nerves penetrate the crura."
- Gray's Anatomy for Students
4. Blood Supply
| Surface | Arteries |
|---|---|
| Superior (thoracic) surface | Musculophrenic and pericardiacophrenic arteries (branches of internal thoracic artery); superior phrenic arteries (from thoracic aorta); intercostal artery branches |
| Inferior (abdominal) surface | Inferior phrenic arteries (branches of abdominal aorta and/or coeliac trunk) - the largest supply |
Venous drainage mirrors the arterial supply: pericardiacophrenic and musculophrenic veins drain into the IVC superiorly; inferior phrenic veins drain into IVC and the left suprarenal vein inferiorly.
- Fischer's Mastery of Surgery, 8e, p. 2591
5. Innervation
5.1 Motor and Sensory Supply
| Nerve | Origin | Supply |
|---|---|---|
| Phrenic nerves (bilateral) | Anterior rami C3, C4, C5 | ALL motor innervation to the entire diaphragm + sensory to the central part |
| Intercostal nerves (6th-11th) | Thoracic roots T6-T11 | Sensory innervation of the peripheral diaphragm |
"Motor innervation of the diaphragm, along with sensory innervation of the central diaphragm, is supplied by the phrenic nerves, which arise from the C3-C5 nerve roots. Sensory innervation of the peripheral diaphragm is supplied by the adjacent sixth through eleventh intercostal nerves."
- Morgan and Mikhail's Clinical Anesthesiology, 7e
The classic mnemonic: C3, 4, 5 keeps the diaphragm alive.
5.2 Course of the Phrenic Nerves
Both phrenic nerves descend through the thorax between the mediastinal pleura and the fibrous pericardium, anterior to the roots of the lungs:
- Right phrenic nerve: Passes along the right side of the right brachiocephalic vein, superior vena cava, and right atrium pericardium. It pierces the diaphragm close to or through the caval opening, just lateral to it.
- Left phrenic nerve: Slightly longer (to accommodate the larger heart on the left). Enters the mediastinum between the left subclavian and left common carotid arteries, passes anterior to the left vagus nerve at the aortic arch, and penetrates the muscular part of the left hemidiaphragm just lateral to the left cardiac surface.
5.3 Intraphrenicic Branching
Once the phrenic nerves traverse the diaphragm, each divides into:
- Sternal branch - runs anteromedially toward the sternum
- Anterolateral branch - passes laterally anterior to the central tendon
- Posterior branch - divides into posterolateral and crural branches
"Division of the diaphragm must take into account the location of the phrenic nerve and its branches."
- Fischer's Mastery of Surgery, 8e
6. Lymphatic Drainage
| Surface | Drainage |
|---|---|
| Superior surface | Anterior, middle, and posterior phrenic nodes |
| Inferior surface | Phrenic nodes (via vessels piercing the diaphragm) and aortic nodes (following inferior phrenic vessels) |
7. Movements and Physiology
During inspiration, the diaphragm contracts and flattens (descends by 1.5-2 cm during quiet breathing, up to 10 cm during deep breathing). This:
- Increases vertical diameter of the thorax
- Lowers intrathoracic pressure below atmospheric, drawing air into the lungs
- Raises intra-abdominal pressure
- Enhances venous return to the heart
The diaphragm accounts for approximately 70% of tidal volume during quiet breathing. Accessory muscles (intercostals, scalenes, sternocleidomastoid) contribute more during increased demand.
8. Anaesthetic Implications
8.1 Effect of Anaesthesia on Diaphragmatic Function
- General anaesthesia reduces functional residual capacity (FRC) primarily because it causes cephalad displacement of the diaphragm, especially in the dependent (posterior) zones
- The diaphragm shifts cranially during anaesthesia, worsening ventilation-perfusion mismatch and predisposing to atelectasis
- Neuromuscular blockade further paralyses diaphragmatic function, necessitating positive pressure ventilation
8.2 Phrenic Nerve Considerations in Regional Anaesthesia
Interscalene Block (ISB)
The most clinically relevant diaphragm consideration in regional anaesthesia:
"A properly performed interscalene block almost invariably blocks the ipsilateral phrenic nerve (completely with nerve stimulation techniques, but less so with certain low-volume ultrasound-guided techniques), so careful consideration must be given to patients with severe pulmonary disease or preexisting contralateral phrenic nerve palsy. Bilateral interscalene blocks are absolutely contraindicated. Hemidiaphragmatic paresis may result in dyspnea, hypercapnia, and hypoxemia."
- Morgan and Mikhail's Clinical Anesthesiology, 7e
Key points:
- ISB provides excellent shoulder analgesia but nearly always blocks the ipsilateral phrenic nerve
- Hemidiaphragm paralysis from ISB reduces pulmonary function by approximately 25% in healthy patients - usually well tolerated
- Contraindicated in patients with contralateral phrenic nerve palsy, severe COPD, or moderate-severe obstructive lung disease
- Associated complications: Horner syndrome (cervicothoracic ganglion block), hoarseness (recurrent laryngeal nerve), pneumothorax (apical pleura proximity)
"In a patient with severe pulmonary compromise or hemidiaphragmatic paralysis, for example, a contralateral interscalene or cervical plexus block with resultant phrenic nerve block could be catastrophic."
- Morgan and Mikhail's Clinical Anesthesiology, 7e
Supraclavicular Block
Also carries a high risk of phrenic nerve blockade (up to 50-70%) due to proximity to the phrenic nerve at C5 level.
Diaphragm-Sparing Alternatives
Recent evidence favours alternatives for patients with respiratory compromise:
- Superior trunk block (STB): Targets the superior trunk of the brachial plexus more distally; evidence shows non-inferior analgesia vs ISB with lower rates of phrenic involvement
- Anterior suprascapular nerve block: Targets the suprascapular nerve at the omohyoid level
- Infraclavicular or axillary blocks: Target cords/terminal nerves below clavicle; spare the phrenic nerve
"Recent evidence suggests diaphragm paresis may be avoidable with more distal 'lung-sparing' block techniques that target the terminal nerves supplying the shoulder joint."
- Miller's Anesthesia, 10e
Cervical Plexus Block (Deep)
- Deep cervical plexus block can spread to C3-C5 roots, blocking the phrenic nerve
- Caution required bilaterally or in patients with compromised pulmonary reserve
8.3 Phrenic Nerve Injury in Thoracic and Cardiac Surgery
- The phrenic nerve lies on the pericardium, anterior to the lung root - it is at risk during cardiac surgery (especially during iced slush cooling), thoracic dissection, and mediastinal procedures
- Division of the phrenic nerve results in permanent ipsilateral hemidiaphragm paralysis
- Intraoperative cold cardioplegia and ice packing are a recognised cause of phrenic nerve palsies after cardiac surgery
8.4 Spinal/Epidural Anaesthesia Level and Diaphragm
- Complete cervical cord injuries above C5 eliminate both phrenic and intercostal nerve function, making spontaneous ventilation impossible
- High thoracic epidurals (above T4) can impair intercostal contributions to breathing, but the diaphragm remains functional as long as C3-C5 segments are spared
- In patients with pre-existing diaphragmatic compromise, high neuraxial blocks must be used cautiously
8.5 Diaphragmatic Breathing in Prone Position
- Prone positioning (used in ARDS management) allows the dorsal diaphragm (functionally dependent in supine) to move more freely, recruiting dependent zones
- Anaesthetists use prone positioning strategically for both ARDS patients on ICU and for posterior spinal/neurosurgical procedures
8.6 Laparoscopic Surgery - Diaphragmatic Implications
- Pneumoperitoneum (CO2 insufflation) elevates the diaphragm cranially, increasing peak airway pressures and reducing FRC
- Steep Trendelenburg (robotic prostatectomy, gynaecological laparoscopy) causes maximal cephalad diaphragm displacement
- CO2 absorbed from the peritoneal cavity crosses the diaphragm and raises PaCO2 - requires increased minute ventilation
- Post-laparoscopic shoulder tip pain is caused by CO2 irritating the undersurface of the diaphragm, with pain referred to C4/C5 dermatomes (shoulder tip) via the phrenic nerve
8.7 Referred Pain via the Phrenic Nerve
Because the phrenic nerve arises from C3-C5, irritation or inflammation of the central diaphragm refers pain to the tip of the shoulder (C4 dermatome):
"Irritation or inflammation of the diaphragm causes pain at the tip of the shoulder. Referred pain occurs when the central nervous system fails to differentiate between visceral and somatic sensory information."
- S Das, Manual on Clinical Surgery
Clinical examples:
- Subphrenic abscess → shoulder tip pain
- Ruptured ectopic pregnancy / haemoperitoneum → shoulder tip pain in Trendelenburg
- Post-laparoscopic CO2 → bilateral shoulder pain
- Diaphragmatic pleural irritation (pneumonia, PE) → ipsilateral shoulder pain
- Hepatic/splenic pathology irritating the diaphragm
8.8 Hiccoughs (Singultus)
Hiccoughs are caused by involuntary, rhythmic spasm of the diaphragm (predominantly left hemidiaphragm) with sudden closure of the glottis. Anaesthetic significance:
- Can be triggered by rapid induction, gastric distension, opioids, or mediastinal irritation
- Intractable hiccoughs post-surgery may indicate phrenic nerve irritation or subphrenic pathology
- Can be treated by phrenic nerve block or use of chlorpromazine, metoclopramide, or baclofen
8.9 Diaphragmatic Hernias
The anaesthetist must be aware of:
- Congenital diaphragmatic hernia (Bochdalek hernia): Left-sided posterolateral defect (90%) causing neonatal respiratory failure; anaesthetic management focuses on avoiding high airway pressures and managing pulmonary hypertension
- Hiatus hernia: Enlargement of the oesophageal hiatus; increases aspiration risk during induction - full stomach precautions, rapid sequence induction (RSI) indicated
- Traumatic diaphragmatic rupture: Usually left-sided after blunt trauma; bowel herniation may compromise ventilation acutely
8.10 Diaphragmatic Pacing
For high cervical spinal cord injuries (above C4) where phrenic nerve integrity is preserved but central drive is lost:
"Patients with injured phrenic nerves (high spinal cord injury) may benefit from diaphragm pacing after intercostal-to-phrenic nerve transfer."
- Mulholland and Greenfield's Surgery, 7e
This is relevant when managing long-term ventilator-dependent patients.
9. Summary Table - Key Anaesthetic Scenarios
| Scenario | Diaphragmatic Relevance |
|---|---|
| Interscalene block | Ipsilateral phrenic nerve block (~100%); reduces ipsilateral lung function ~25% |
| Deep cervical plexus block | Phrenic nerve block; bilateral risk catastrophic |
| High neuraxial block | Intercostal accessory muscles impaired; diaphragm preserved if C3-C5 spared |
| Laparoscopy/Trendelenburg | Cephalad displacement; raised PAP; CO2 absorption; shoulder tip pain |
| Cardiac surgery | Phrenic nerve at risk from dissection and cold cardioplegia |
| Prone positioning | Recruits dorsal lung zones; improves diaphragm mechanics |
| Hiatus hernia | Aspiration risk; use RSI |
| CDH (neonatal) | Avoidance of high Pip; manage pulmonary hypertension |
| Post-op shoulder tip pain | Referred diaphragmatic irritation via phrenic nerve (C4) |
Sources
- Gray's Anatomy for Students - Diaphragm anatomy, crura, arcuate ligaments, innervation
- Morgan and Mikhail's Clinical Anesthesiology, 7e - Phrenic nerve innervation, interscalene block, phrenic nerve palsies
- Miller's Anesthesia, 10e - Interscalene block, diaphragm-sparing techniques, superior trunk block
- Fischer's Mastery of Surgery, 8e - Phrenic nerve course, intraphrenic branching, vascular supply
- Bailey and Love's Short Practice of Surgery, 28e - Referred pain, diaphragmatic hernias
- Mulholland and Greenfield's Surgery, 7e - Diaphragmatic pacing
This is a shared conversation. Sign in to Orris to start your own chat.