Clinical cardio mbbs final year examination university exam 20 marks. Empyema thiracis, detailed and management also Briefly describe intercostals drainage, rib resection, decortication and window operation
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative surgical textbooks. Let me compile the complete answer.
EMPYEMA THORACIS
Clinical Cardiology / Surgery - MBBS Final Year | 20 Marks
DEFINITION
Empyema thoracis is a collection of purulent fluid (pus) within the pleural space, resulting from invasion of pyogenic bacteria, fungi, parasites, or mycobacteria. It is characterized by pleural fluid with WBC >25,000/mL (neutrophilic predominance), glucose <30 mg/dL, and pH <7.2.
- Fischer's Mastery of Surgery, 8th ed.
- Sabiston Textbook of Surgery
ETIOLOGY / PATHOGENESIS
Sources of infection (Schwartz's Principles of Surgery):
| Route | Examples | Frequency |
|---|---|---|
| Contiguous spread | Pneumonia, lung abscess, subphrenic abscess, esophageal perforation, mediastinitis | 50-60% |
| Direct inoculation | Thoracic surgery, thoracentesis, penetrating chest injury | 30-40% |
| Hematogenous | Distant septic focus | <1% |
Common organisms:
- Gram-positive: S. pneumoniae, S. aureus, beta-hemolytic streptococci
- Gram-negative aerobes: E. coli, Klebsiella, Pseudomonas
- Anaerobes: Fusobacterium nucleatum, Prevotella spp., Bacteroides fragilis (especially in aspiration, alcoholism, periodontal disease)
- Polymicrobial cultures present in up to 50% of cases
- Cultures may be sterile if antibiotics were started before culture
- Fishman's Pulmonary Diseases and Disorders
THREE STAGES OF EMPYEMA
The clinical course classically progresses over ~3 weeks:
| Stage | Week | Fluid Character | pH / Glucose / LDH | Treatment |
|---|---|---|---|---|
| Stage I - Exudative | Week 1 | Thin, free-flowing, watery | pH >7.3, glucose >60, LDH <500 | Antibiotics ± thoracentesis |
| Stage II - Fibrinopurulent | Week 2 | Turbid, loculated, fibrinous adhesions | pH <7.2, glucose <40 | Chest tube / VATS |
| Stage III - Organized/Chronic | Week 3+ | Thick peel on visceral pleura; trapped lung | Highly viscous, acid | Decortication / open drainage |
- Fischer's Mastery of Surgery, 8th ed.
- Schwartz's Principles of Surgery, 11th ed.
CLINICAL FEATURES
Symptoms:
- Fever, chills, rigors (constitutional)
- Chest pain (pleuritic - sharp, worse on breathing)
- Dyspnoea, cough (often productive if underlying pneumonia)
- Weight loss, malaise, anorexia (in chronic cases)
Signs:
- Tachycardia, tachypnoea
- Dullness to percussion over affected area
- Reduced/absent breath sounds
- Reduced chest expansion on affected side
- Intercostal fullness may be present
- In chronic empyema: scoliosis toward affected side, chest wall retraction, clubbing
INVESTIGATIONS
Blood:
- Raised TLC (neutrophilia), raised ESR, raised CRP
- Blood cultures (bacteremia may be present)
- Low albumin in chronic cases
Pleural Fluid Analysis (Thoracentesis):
- Appearance: turbid, frankly purulent
- WBC >25,000/mL with neutrophil predominance
- Glucose <30 mg/dL (empyema) - low due to bacterial metabolism
- pH <7.2 (exudate)
- LDH >1000 U/L
- Gram stain and culture (aerobic, anaerobic, AFB, fungal)
- Protein, LDH (Light's criteria for exudate)
Imaging:
- CXR: Homogeneous opacity, blunting of costophrenic angle; D-shaped opacity suggests loculation; mediastinal shift away from affected side
- CT chest (investigation of choice): Confirms diagnosis, shows loculations, pleural thickening, "split pleura sign" (enhancement of both pleural layers), underlying lung pathology
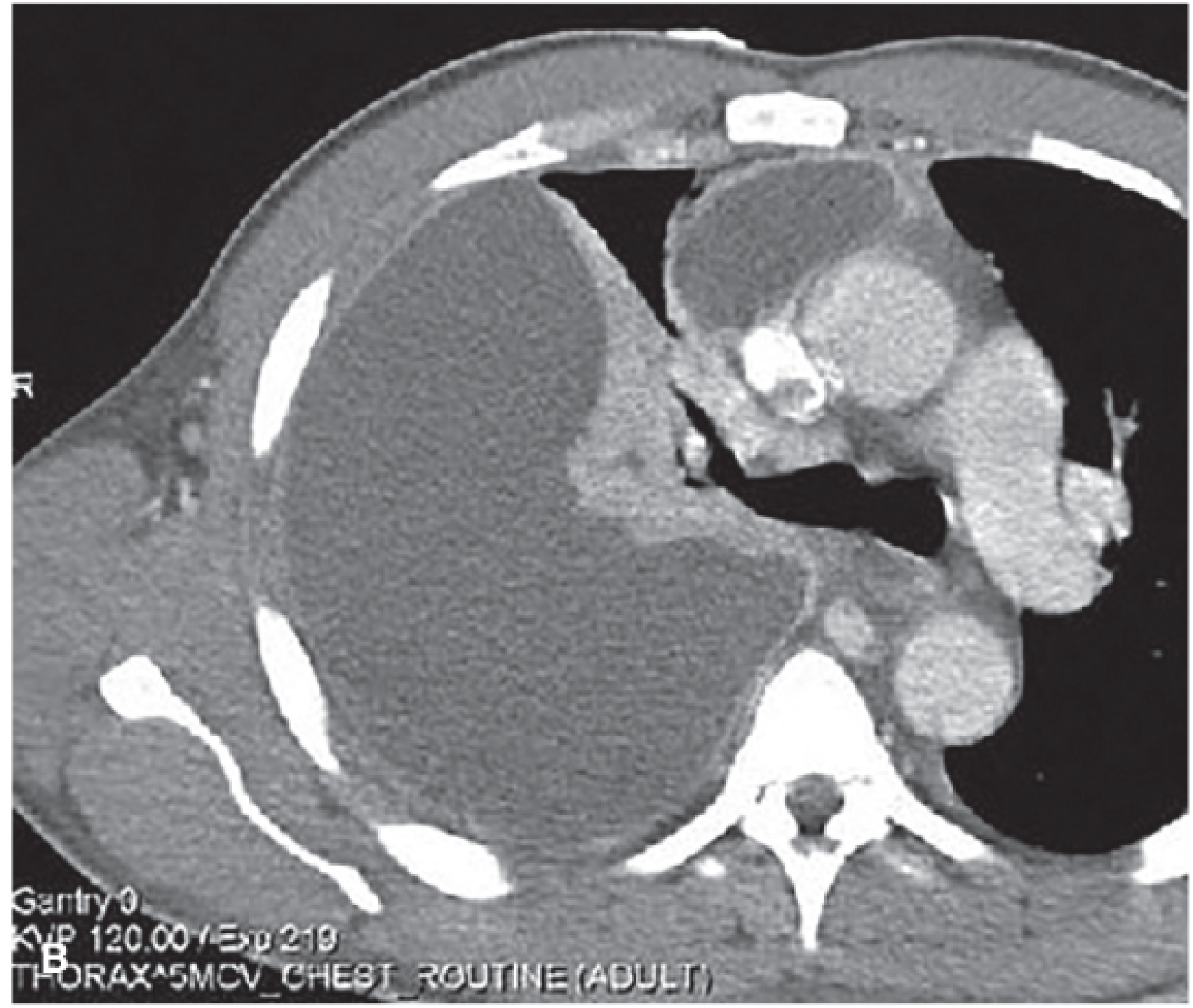
CT chest showing Stage II complicated parapneumonic effusion with large right empyema (Fischer's Mastery of Surgery, 8th ed.)
- Ultrasound: Confirms fluid, guides drainage; internal echoes/septations indicate fibrinopurulent stage
MANAGEMENT
A. General / Medical Measures
- Antibiotics (systemic, not intrapleural): Broad spectrum empirically covering gram-positive, gram-negative, and anaerobes
- e.g., Piperacillin-tazobactam / Meropenem + Metronidazole (for anaerobes)
- Modify based on culture and sensitivity
- Duration typically 3-6 weeks
- Nutritional support, physiotherapy, analgesics
B. DRAINAGE PROCEDURES
1. Thoracentesis (Aspiration)
- Used in Stage I (exudative phase) when fluid is thin and free-flowing
- Simple needle aspiration - adequate for early parapneumonic effusions
- Complete drainage + lung re-expansion confirms adequacy
2. INTERCOSTAL TUBE DRAINAGE (Closed Chest Drainage / ICD)
Indications:
- Stage I-II empyema (fibrinopurulent phase)
- Frankly purulent or rapidly accumulating fluid
- Bronchopleural fistula with empyema
- Loculated fluid unresponsive to thoracentesis
Technique:
- Patient positioned semi-recumbent or lateral
- Site: usually 5th-6th intercostal space, mid-axillary line (or ultrasound-guided)
- Local anaesthesia; incision over upper border of rib below (to avoid neurovascular bundle)
- Blunt dissection through intercostal muscles; finger sweep to confirm pleural cavity
- Large-bore chest tube (28-32 Fr) inserted; directed posteriorly and basally
- Connected to underwater seal drainage (Bülau drain) ± suction (-20 cmH₂O)
- Tube removed when: drainage <100-200 mL/day, lung expanded on imaging, infection resolving
Adjuncts (intrapleural fibrinolytics):
- tPA (10 mg) + DNase (5 mg): instilled via chest tube, clamped 1-2 hours, drain released; position changes every 15 minutes; repeated daily for 3-5 days
- Reduces viscosity, breaks down fibrin loculations
- Combination more effective than either alone
- Reduces need for surgical intervention; reduces hospital stay by ~7 days
- Schwartz's, Fischer's
Failure criteria (chest tube inadequate - needs surgery):
- Lung fails to re-expand
- Persistent fever >48-72 hours
- Drainage >200 mL/day beyond 7 days
- CT shows inadequate drainage/loculations
- Fishman's Pulmonary Diseases
3. RIB RESECTION (Open Drainage / Drainage via Rib Resection)
Indications:
- Chronic/organized empyema where chest tube drainage fails
- When closed drainage is ineffective and patient is unfit for thoracotomy
- As a temporizing measure before definitive surgery
Principle: Resection of a segment of rib overlying the empyema cavity provides a wide, dependent, gravity-dependent opening for drainage. The parietal pleura becomes adherent to the chest wall (symphysis), preventing collapse - making this "open drainage" safe.
Technique:
- Patient under GA or local anaesthesia
- A 5-7 cm segment of the rib overlying the most dependent part of the empyema cavity is resected (usually 8th or 9th rib posterolaterally)
- Periosteum is stripped; rib excised with rib shears
- Underlying parietal pleura entered; pus drained
- Cavity washed with saline/antiseptic
- A large-bore tube/drain placed in the cavity and kept open (not connected to underwater seal)
- Cavity is packed and managed with daily dressings until it gradually obliterates
- Skin closure delayed (secondary intention)
Advantage: Simple, avoids GA, allows gravity-dependent drainage
Disadvantage: Slower healing; requires prolonged nursing/dressing care; leaves chest wall deformity
- Fishman's, Schwartz's
4. DECORTICATION
Definition: Surgical removal of the thick fibrous cortex (pleural "peel") from the surface of the entrapped lung so that it can re-expand and obliterate the empyema space.
Indications:
- Stage III (organized/chronic) empyema with thickened visceral pleura
- "Trapped lung" - lung encased by fibrous peel and unable to expand
- Failed chest tube drainage with persistent pleural infection
- Restrictive physiology from fibrous pleural peel
Timing: Usually performed after 4-6 weeks of medical treatment once the peel is organized but before the lung becomes irreversibly fibrosed.
Surgical Approach:
- Posterolateral thoracotomy (standard) OR
- VATS (Video-Assisted Thoracoscopic Surgery) in selected early-stage cases
Operative Steps:
- Posterolateral thoracotomy through 5th or 6th intercostal space
- Empyema cavity entered; pus and debris evacuated
- The thick fibrous peel (cortex) overlying the visceral pleura is carefully dissected free using a Cobb elevator, gauze swabs, and sharp dissection
- Both parietal cortex (from chest wall) and visceral cortex (from lung surface) are removed
- Care is taken NOT to damage the underlying visceral pleura (which would cause air leak)
- Lung is inflated intraoperatively to confirm full expansion
- Chest drains placed; chest closed in layers
Result: Lung re-expands to fill the pleural cavity, eliminating the dead space.
Complications: Air leak, bleeding, bronchopleural fistula, incomplete expansion, wound infection
"The fibrous cortex or peel from the entrapped underlying lung is removed so that the lung can expand to obliterate the pleural space... It requires careful dissection to remove the parietal and visceral cortex, taking care not to damage the visceral pleura, so allowing the lung to re-expand fully."
- Bailey & Love's Short Practice of Surgery, 28th ed.
- Fischer's Mastery of Surgery, 8th ed.
5. WINDOW OPERATION (Thoracostomy Window / Eloesser Flap)
Definition: A permanent or semi-permanent opening (window) is created in the chest wall by excising segments of 2-3 ribs to allow open drainage and packing of the empyema cavity. It converts the closed empyema space into an open cavity accessible for daily care.
Indications:
- Chronic empyema in debilitated/frail patients unfit for thoracotomy
- Empyema with bronchopleural fistula post-pneumonectomy (where definitive surgery is too risky)
- Failed or recurrent empyema after rib resection drainage
- As a palliative/temporizing procedure to allow healing
Principle: By marsupializing the empyema cavity to the skin surface, the cavity can be irrigated, packed, and gradually allowed to granulate and contract. If a bronchopleural fistula exists, healing of the fistula can occur once the cavity is clean.
Technique (Classic Eloesser Flap / Modified):
- Segments of 2-3 ribs (usually 2-3 cm each) overlying the empyema are resected
- The skin is fashioned into a U-shaped or tongue flap that is sutured to the parietal pleura, creating a permanent cutaneous opening (the "window")
- The cavity is packed with gauze/Betadine soaked dressings
- Daily dressing changes allow the cavity to gradually granulate inward
- Once the cavity is clean and the bronchopleural fistula (if present) heals, the window can be formally closed - often with a muscle flap (e.g., latissimus dorsi, serratus anterior, or omentum)
Advantages:
- Applicable in high-risk patients
- Does not require general anaesthesia
- Converts life-threatening infection to a manageable chronic wound
Disadvantages: Prolonged healing, cosmetic deformity, requires frequent dressing changes, risk of superinfection
- Fishman's Pulmonary Diseases and Disorders (Eloesser flap described)
- Schwartz's Principles of Surgery, 11th ed.
SUMMARY TABLE - SURGICAL PROCEDURES FOR EMPYEMA
| Procedure | Stage | Principle | Key Feature |
|---|---|---|---|
| Thoracentesis | Stage I | Needle aspiration | Free-flowing fluid only |
| ICD (Chest Tube) | Stage I-II | Closed drainage to underwater seal | ± tPA/DNase instillation |
| VATS | Stage II | Minimally invasive washout / decortication | Early surgery reduces hospital stay |
| Rib Resection + Open Drainage | Chronic | Open, gravity-dependent drainage after rib excision | Patient unfit for thoracotomy |
| Decortication | Stage III (organized) | Peel removal → lung re-expansion | Thoracotomy or VATS; eliminates trapped lung |
| Window Operation (Eloesser) | Chronic, post-pneumonectomy, BPF | Open cavity marsupialisation to skin | Palliative; for high-risk patients |
COMPLICATIONS OF EMPYEMA
- Bronchopleural fistula - pus enters bronchial tree
- Pneumothorax (if BPF develops)
- Empyema necessitatis - pus burrows through chest wall, presents as subcutaneous swelling
- Osteomyelitis of ribs
- Septicaemia
- Fibrothorax - complete fibrotic obliteration of pleural space
- Scoliosis (in children, from chronic empyema)
- Restrictive lung disease from trapped lung
MORTALITY
- Ranges from 1% in healthy patients to >40% in immunocompromised patients
- Death often reflects severity of underlying comorbidity
- Schwartz's Principles of Surgery, 11th ed.
Sources: Sabiston Textbook of Surgery; Fischer's Mastery of Surgery, 8th ed.; Schwartz's Principles of Surgery, 11th ed.; Bailey & Love's Short Practice of Surgery, 28th ed.; Fishman's Pulmonary Diseases and Disorders; Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.