A 30 Year old male met with road traffic accident and had massive haemorrhage. The patient was pale, pulse was rapid and thread skin was cold and clammy. (2+3+10) (2023P1)
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a thorough answer. The question is marked (2+3+10) suggesting:
- 2 marks: Diagnosis / identify the condition (hemorrhagic/hypovolemic shock)
- 3 marks: Classification (ATLS Classes I-IV)
- 10 marks: Pathophysiology + Management
Let me now compose the full answer.
Hemorrhagic (Hypovolemic) Shock Following Road Traffic Accident
PART 1 (2 marks) - Diagnosis
The clinical picture - pallor, rapid thready pulse, cold and clammy skin following massive hemorrhage after RTA - is classic hemorrhagic (hypovolemic) shock.
Definition: Hemorrhagic shock results from rapid reduction in intravascular blood volume following hemorrhage, leading to an imbalance between systemic oxygen delivery and oxygen consumption, causing inadequate tissue perfusion.
- Pallor = peripheral vasoconstriction diverting blood from skin
- Rapid thready pulse = compensatory tachycardia + reduced stroke volume
- Cold and clammy skin = sympathetic-mediated vasoconstriction + sweat gland activation
This is a "cold shock" characterized by increased systemic vascular resistance (SVR) and decreased cardiac output (CO) - in contrast to septic/distributive shock which is warm. (Sabiston Textbook of Surgery)
PART 2 (3 marks) - Classification (ATLS Classes)
Based on ATLS (Advanced Trauma Life Support), hemorrhagic shock is classified into four classes based on blood loss:
| Parameter | Class I | Class II | Class III | Class IV |
|---|---|---|---|---|
| Blood loss (mL) | Up to 750 | 750-1500 | 1500-2000 | >2000 |
| Blood loss (% BV) | Up to 15% | 15-30% | 30-40% | >40% |
| Pulse rate | <100 | >100 | >120 | >140 |
| Blood pressure | Normal | Normal | Decreased | Decreased |
| Pulse pressure | Normal/Increased | Decreased | Decreased | Decreased |
| Respiratory rate | 14-20 | >20-30 | 30-40 | >35 |
| Urine output (mL/hr) | >30 | 20-30 | 5-15 | Negligible |
| CNS/Mental status | Slightly anxious | Mildly anxious | Anxious & confused | Confused & lethargic |
(Schwartz's Principles of Surgery, 11th ed.)
The patient described (massive hemorrhage, rapid thready pulse, cold/clammy skin) fits Class III-IV shock.
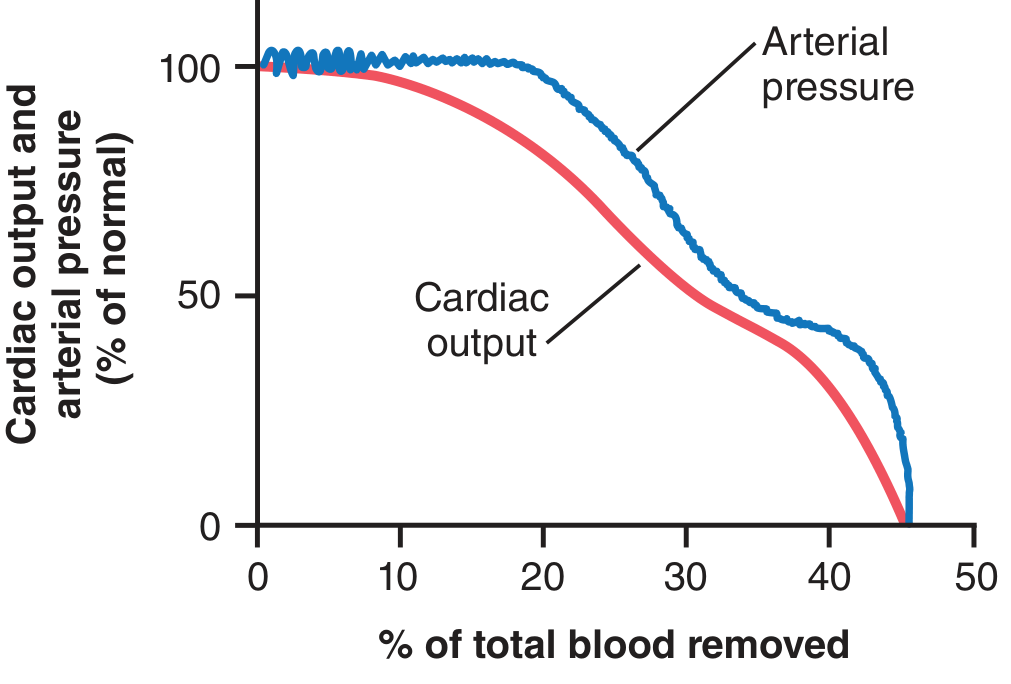
Key note: Only 10% of total blood volume can be removed with almost no effect on arterial pressure or cardiac output. Greater blood loss diminishes cardiac output first, then arterial pressure - both fall to zero when ~40-45% of total blood volume is removed. (Guyton and Hall Medical Physiology)
PART 3 (10 marks) - Pathophysiology and Management
PATHOPHYSIOLOGY
A. Initial Hemodynamic Response
Hemorrhage reduces intravascular volume → decreased venous return → decreased cardiac preload → decreased cardiac output → decreased arterial blood pressure.
The cardiac output falls first; arterial pressure is maintained longer via sympathetic reflexes (see Guyton graph below):
B. Neuroendocrine (Sympathoadrenal) Compensation
Baroreceptors in the carotid sinus and aortic arch detect the fall in blood pressure and trigger a powerful sympathetic response:
- Arteriolar vasoconstriction - increases total peripheral resistance (maintains BP)
- Venous constriction - increases venous return to the heart
- Tachycardia - heart rate can rise to 160-180 bpm
- Adrenal medulla releases epinephrine and norepinephrine
- Renin-angiotensin-aldosterone system (RAAS) activation - renal vasoconstriction + sodium and water retention
- ADH (vasopressin) release from posterior pituitary - peripheral vasoconstriction + free water retention
- Cortisol and glucagon release - mobilizes glucose
Blood is preferentially redirected to the heart, brain, and kidneys at the expense of the skin (explaining cold, clammy skin), gut, and muscle.
C. Microcirculatory and Cellular Response
- Ischemic cells cannot maintain aerobic metabolism → switch to anaerobic glycolysis → lactic acid accumulation → metabolic acidosis
- Base deficit becomes progressively more negative even while BP and pH appear normal (base deficit is the earliest marker of clinically significant hemorrhage)
- Individual ischemic cells take up interstitial fluid → further depleting intravascular volume
- Cellular edema can restrict adjacent capillary flow - the "no-reflow" phenomenon - preventing reversal of ischemia even after macroperfusion is restored
D. Inflammatory & Organ-level Response
- Ischemic cells produce and release: lactate, free radicals, prostacyclin, thromboxane, prostaglandins, leukotrienes, endothelin, complement, interleukins, TNF, and damage-associated molecular patterns (DAMPs)
- These compounds cause direct cellular damage and amplify the systemic inflammatory response
- Multiple organ failure (MOF) can result from this inflammatory cascade
Organ-specific effects:
- CNS: Reflexes and cortical activity depressed; irreversible damage with prolonged ischemia
- Kidney: Initially compensates by vasoconstriction; prolonged hypotension → acute tubular necrosis (ATN)
- Lung: Capillary leak → ARDS (Adult Respiratory Distress Syndrome)
- Liver & gut: Mucosal barrier breakdown → bacterial translocation
E. Progressive vs. Compensated Shock
There is a critical threshold of blood loss. Below this threshold, the body's compensatory mechanisms (baroreceptors, RAAS, ADH, reverse stress-relaxation of vessels) can restore circulation = compensated (nonprogressive) shock.
Beyond this threshold, shock becomes progressive through vicious positive-feedback cycles as shown in the diagram below from Guyton and Hall:
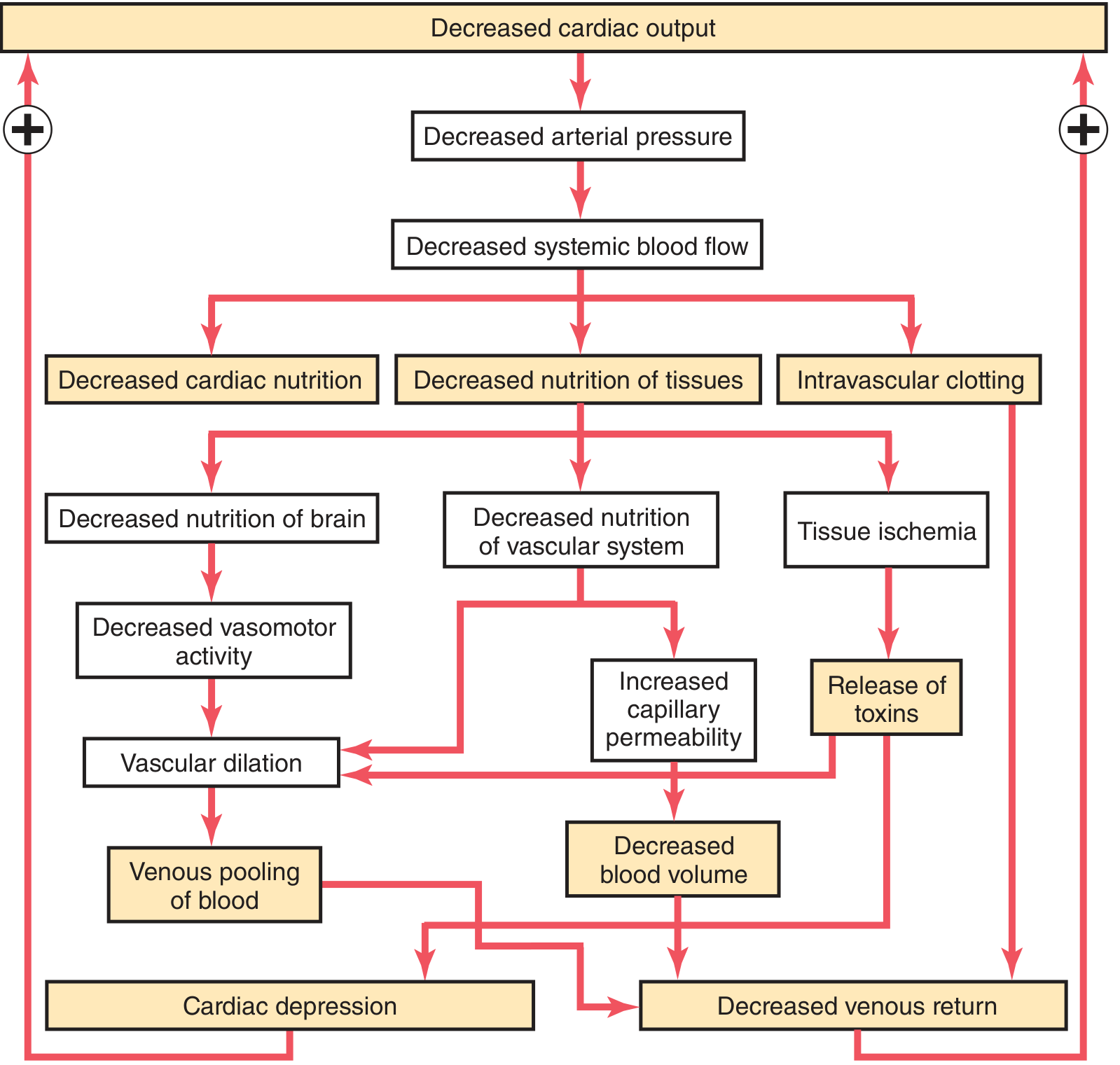
Key positive-feedback cycles include:
- Decreased cardiac output → decreased coronary flow → cardiac depression → further decreased output
- Decreased systemic flow → decreased vasomotor center nutrition → vasomotor failure → vascular dilation → venous pooling
- Tissue ischemia → increased capillary permeability → further blood volume loss
- Intravascular clotting → tissue ischemia → toxin release → further cardiac depression
Once irreversible shock is reached, massive ischemic damage, cell membrane failure (Na-K ATPase failure), and widespread intravascular coagulation make survival impossible even with blood transfusion.
MANAGEMENT
Management follows the ATLS primary survey (ABCDE) principle.
1. Immediate - Control of Hemorrhage
- Direct pressure on external bleeding wounds
- Tourniquet for extremity hemorrhage
- Pelvic binder for pelvic fractures (can lose >2000 mL into pelvis)
- Emergency surgical hemorrhage control (damage control surgery) if internal hemorrhage
2. Airway and Breathing
- Maintain airway; administer high-flow oxygen (100%)
- Intubate if GCS < 8 or airway at risk
3. Intravenous Access and Resuscitation
- Establish two large-bore peripheral IV lines (16G or larger)
- Draw blood for: FBC, crossmatch, coagulation studies, ABG, base deficit, lactate
4. Fluid Resuscitation Strategy
Hemorrhagic shock = blood products are the resuscitative fluid of choice. Crystalloid alone leads to anemia and dilutional coagulopathy. (Sabiston Textbook of Surgery)
- Massive Transfusion Protocol (MTP): Packed Red Blood Cells (pRBCs) : Fresh Frozen Plasma (FFP) : Platelets in 1:1:1 ratio
- Recent evidence suggests whole blood may be superior to component therapy
- Tranexamic acid (TXA): Should be given within 3 hours of injury (CRASH-2 trial evidence) - reduces fibrinolysis and mortality
- Viscoelastic testing (TEG/ROTEM) can guide targeted component replacement, especially when transfusion exceeds 10 units pRBCs
- Avoid hypothermia (use warmed fluids) - hypothermia worsens coagulopathy
The lethal triad of trauma must be prevented:
Hypothermia + Acidosis + Coagulopathy = irreversible death
5. Response to Resuscitation (classify patient)
| Category | Description | Action |
|---|---|---|
| Responder | Vital signs normalize | Investigate for occult injury |
| Transient responder | Initial improvement then deteriorates | Urgent surgical evaluation |
| Non-responder | No response despite resuscitation | Immediate surgical intervention |
6. Vasopressors
- Early vasopressor use in hemorrhagic shock has minimal evidence but may be used as a temporizing bridge while blood products are given
- Evidence supports vasopressin in a "vasopressin-deficient state" seen in prolonged shock
7. Permissive Hypotension (Damage Control Resuscitation)
- For penetrating vascular injuries: target SBP ~90 mmHg (to prevent dislodging an endogenous clot)
- Exception: TBI patients require SBP >100 mmHg to maintain cerebral perfusion pressure
- This concept is NOT appropriate for blunt trauma with TBI
8. Endpoints of Resuscitation
- Normalize: HR, BP, urine output (>0.5 mL/kg/hr)
- Clearance of lactate
- Improvement in base deficit (toward 0)
- Normalization of coagulation
9. Monitoring
- Urine output (Foley catheter)
- ABG with lactate and base deficit
- CVP / IVC ultrasound to distinguish hemorrhagic from cardiogenic shock
- eFAST (extended Focused Assessment with Sonography for Trauma) to identify source
10. Definitive Hemorrhage Control
- Damage control surgery: abbreviated initial operation to stop bleeding and contamination; definitive repair after resuscitation in ICU
- Interventional radiology: angioembolization for pelvic/hepatic/splenic hemorrhage
Summary
| Aspect | Key Points |
|---|---|
| Diagnosis | Hemorrhagic shock - rapid pulse, pallor, cold/clammy = Class III-IV |
| Mechanism | Hypovolemia → ↓CO → sympathetic activation → vasoconstriction → ischemia → acidosis |
| Classification | ATLS Classes I-IV based on % blood volume lost |
| Management | Stop bleeding, O2, MTP (1:1:1), TXA within 3 hrs, damage control surgery |
| Goals | Correct lethal triad (hypothermia, acidosis, coagulopathy) |
Sources: Guyton and Hall Textbook of Medical Physiology | Schwartz's Principles of Surgery, 11th ed. | Sabiston Textbook of Surgery | Miller's Anesthesia, 10th ed. | Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.