Explain glomerular filtration like how i should write the answer for my university exams
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content I need. Let me compile a thorough, exam-ready answer.
Glomerular Filtration - Exam Answer
Definition
Glomerular filtration is the first step in urine formation. It is the process by which a portion of the blood plasma passing through the glomerular capillaries is forced into Bowman's space (the urinary space), forming the glomerular ultrafiltrate. The ultrafiltrate resembles plasma but is virtually free of plasma proteins and blood cells.
(Costanzo Physiology, p. 267)
Normal Values (Memorize These)
| Parameter | Value |
|---|---|
| Glomerular Filtration Rate (GFR) | 125 mL/min or 180 L/day |
| Renal Blood Flow (RBF) | ~1200 mL/min |
| Renal Plasma Flow (RPF) | ~625 mL/min |
| Filtration Fraction (GFR/RPF) | ~20% |
The kidneys expose the entire extracellular fluid to tubular scrutiny >10 times per day, allowing rapid clearance of waste products and toxic substances. (Medical Physiology)
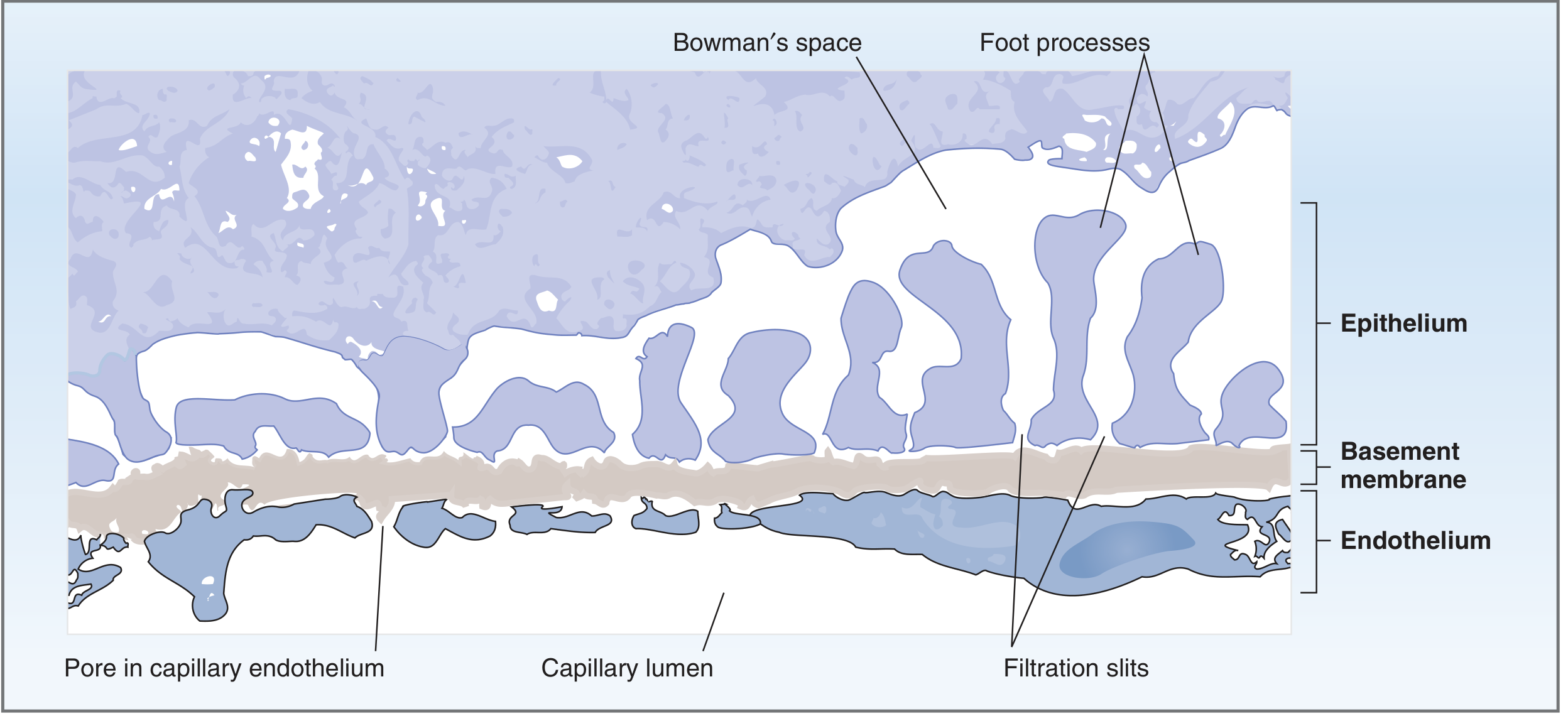
The Glomerular Filtration Barrier
The barrier has three structural layers (from capillary lumen to Bowman's space):
1. Fenestrated Endothelium
- Pores: 70-100 nm in diameter
- Freely allows fluid, small solutes, and even plasma proteins to pass
- Prevents filtration of blood cells (pores too small for these)
- Coated with negatively charged glycoproteins that repel anionic proteins like albumin
2. Glomerular Basement Membrane (GBM) - THE MAJOR BARRIER
- Has three sub-layers: lamina rara interna (inner) + lamina densa (middle) + lamina rara externa (outer)
- Composed of type IV collagen and proteoglycans (heparan sulfate)
- Does not permit filtration of plasma proteins - this is the most significant barrier
- Proteoglycans carry strong negative charges that electrostatically repel anionic proteins
3. Visceral Epithelium (Podocytes)
- Specialized cells with long foot processes (pedicels) that wrap around the capillaries
- Between foot processes are filtration slits (25-60 nm wide)
- Filtration slits are bridged by thin slit diaphragms containing proteins nephrin and podocin
- Mutations in nephrin gene → absent slit diaphragms → massive proteinuria
(Costanzo Physiology, pp. 267-268; Guyton & Hall Medical Physiology)
Determinants of Filterability
Filtration of a substance depends on two factors:
A. Molecular Size
| Substance | Molecular Weight | Filterability |
|---|---|---|
| Water, Na+, Glucose, Inulin | 18 - 5,500 | 1.0 (freely filtered) |
| Myoglobin | 17,000 | 0.75 |
| Albumin | 69,000 | 0.005 (barely filtered) |
B. Electrical Charge
- The barrier is lined with fixed negative charges (glycoproteins on endothelium, GBM, podocytes)
- Cationic molecules are attracted → filtered MORE readily
- Anionic molecules are repelled → filtered LESS readily
- This is why albumin (negatively charged at physiologic pH) is barely filtered despite its size being at the threshold
- In certain glomerular diseases (e.g., minimal change nephropathy), loss of negative charge → proteinuria
Forces Driving Glomerular Filtration - The Starling Equation
GFR is governed by the Starling forces (just like in systemic capillaries), but with one modification: oncotic pressure of Bowman's space = 0 (virtually no protein enters the filtrate).
The GFR Equation:
GFR = Kf × [(P_GC - P_BS) - π_GC]
Where:
- Kf = Filtration coefficient (hydraulic conductance × surface area)
- P_GC = Hydrostatic pressure in glomerular capillary (45 mmHg) → FAVORS filtration
- P_BS = Hydrostatic pressure in Bowman's space (10 mmHg) → OPPOSES filtration
- π_GC = Oncotic pressure in glomerular capillary (28 mmHg) → OPPOSES filtration
Net Ultrafiltration Pressure:
| Force | Value (mmHg) | Direction |
|---|---|---|
| P_GC (glomerular capillary hydrostatic) | +45 | Favors filtration |
| P_BS (Bowman's space hydrostatic) | -10 | Opposes filtration |
| π_GC (glomerular capillary oncotic) | -28 | Opposes filtration |
| Net Ultrafiltration Pressure | +7 mmHg | Net: Favors filtration |
Note: π_GC is NOT constant - as fluid is filtered out, protein concentrates in the capillary, increasing π_GC. Eventually π_GC rises until net ultrafiltration pressure = 0, a state called filtration equilibrium.
(Costanzo Physiology, pp. 268-269)
The Filtration Coefficient (Kf)
Kf = intrinsic water permeability per unit area × total surface area
The Kf of glomerular capillaries is >100-fold higher than skeletal muscle capillaries because:
- Greater total surface area (extensive capillary loops in the glomerulus)
- Higher intrinsic water permeability
This extremely high Kf is why GFR is 180 L/day - far exceeding filtration in any other capillary bed.
Significance of a High GFR
A high GFR (180 L/day) is essential because:
- Rapid toxin excretion - sudden rise in a toxic substance is quickly cleared by filtration
- Low steady-state waste levels - without high GFR, blood urea nitrogen (BUN) would accumulate to dangerous levels
Classic Example (Pitts): A person consuming 70 g/day protein produces 12 g/day urea nitrogen:
- Normal GFR (180 L/day) → BUN = 6.7 mg/dL
- End-stage renal disease, GFR 10% of normal (18 L/day) → BUN = 67 mg/dL
Mesangial Cells (Bonus Point)
Mesangial cells surround and lie between the glomerular capillaries. They:
- Produce extracellular matrix providing structural support
- Contain actin-myosin microfilaments with contractile properties
- Can alter capillary blood flow (and therefore GFR) by contracting or relaxing
- Are NOT part of the filtration barrier itself
Clinical Correlations (Exam Favorites)
| Condition | Mechanism | Effect on Filtration |
|---|---|---|
| Minimal change nephropathy | Loss of negative charges on barrier | Proteinuria (albumin filtered) |
| Mutations in nephrin/podocin | Absent slit diaphragms | Massive proteinuria (congenital nephrotic syndrome) |
| Increased efferent arteriolar tone (e.g., angiotensin II) | Raises P_GC | Increases GFR |
| Urinary tract obstruction | Raises P_BS | Decreases GFR |
| Hypoalbuminemia | Lowers π_GC | Increases GFR (but edema elsewhere) |
| End-stage renal disease | Loss of nephrons → loss of Kf and surface area | Greatly reduced GFR |
Exam Writing Tips
- Always define GFR first with the normal value (125 mL/min / 180 L/day)
- Draw the three-layer barrier diagram - examiners love it
- Write the Starling equation, define each term, and calculate the net ultrafiltration pressure (+7 mmHg)
- Mention both size AND charge as determinants of filterability
- Include filtration equilibrium - it shows depth of understanding
- Close with 1-2 clinical correlations
Sources: Costanzo Physiology 7e, pp. 267-270 | Guyton & Hall Medical Physiology | Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.