Cushings syndrome
Reading File
Finding Sources
Searching PubMed
"Cushing syndrome" diagnosis treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive information to write a thorough answer. Let me compile everything.
Cushing's Syndrome
Definition
Cushing's syndrome is the clinical state resulting from chronic exposure to excess glucocorticoids, regardless of the source. When hypercortisolism is specifically caused by an ACTH-secreting pituitary adenoma, it is termed Cushing's disease - a subset of Cushing's syndrome.
- Campbell Walsh Wein Urology, p. 3134
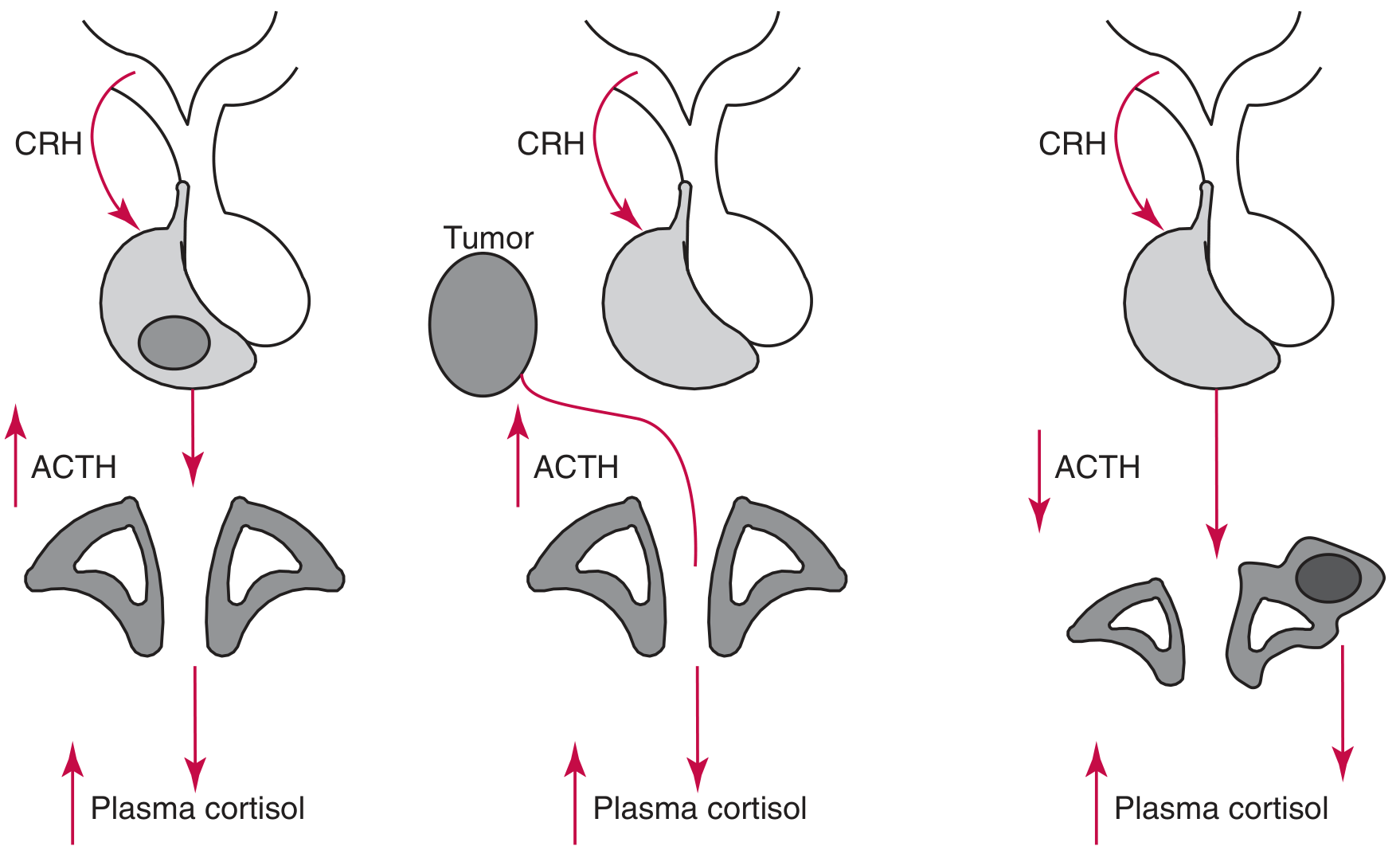
Pathophysiology & The HPA Axis
The zona fasciculata of the adrenal cortex secretes ~20 mg of cortisol daily under regulation of the hypothalamic-pituitary-adrenal (HPA) axis:
- Hypothalamus releases CRH (corticotropin-releasing hormone)
- Anterior pituitary secretes ACTH (from POMC cleavage)
- Adrenal cortex produces cortisol
- Cortisol completes a negative feedback loop by suppressing CRH and ACTH
Cortisol secretion follows a circadian rhythm - peak in the morning, nadir around 11 PM. Even small disruptions in this rhythm are considered pathological.
Etiology & Classification
| Type | Cause | % of Endogenous Cases |
|---|---|---|
| Exogenous | Iatrogenic glucocorticoid use (oral, topical, inhaled) | Most common overall |
| Cushing's Disease (ACTH-dependent) | Pituitary corticotroph adenoma | ~68-70% of endogenous |
| Ectopic ACTH syndrome (ACTH-dependent) | Non-pituitary tumors (small cell lung CA, carcinoid, etc.) | ~10-12% |
| Adrenal adenoma (ACTH-independent) | Autonomous cortisol secretion | ~10% |
| Adrenal carcinoma (ACTH-independent) | Autonomous cortisol secretion | ~8% |
| AIMAH / PPNAD | Bilateral adrenal hyperplasia | Rare |
ACTH-dependent causes account for 80-85% of endogenous Cushing's syndrome.
- Campbell Walsh Wein Urology, p. 3135-3136
- Henry's Clinical Diagnosis and Management, p. 1806
Key features of ectopic ACTH syndrome (vs. pituitary Cushing's disease):
- More rapid onset
- Greater proximal limb weakness, skin pigmentation, hypokalemia, hypertension, and glycosuria
- Plasma ACTH usually >20 pg/mL (at times >50 pg/mL)
- Not suppressed by dexamethasone
Clinical Features
Classic features described by Harvey Cushing (1932):
Metabolic/Body Composition:
- Central (truncal) obesity - "buffalo hump," supraclavicular fat pads
- Moon face (facial plethora)
- Weight gain with thin extremities
Skin:
- Purple/violaceous striae over abdomen and extremities
- Skin fragility, easy bruising
- Acne, hirsutism
- Hyperpigmentation (especially in ectopic ACTH - due to high ACTH stimulating melanocyte receptors)
Musculoskeletal:
- Proximal muscle weakness (myopathy) - can be the presenting complaint to neurologists
- Osteoporosis, pathological fractures, kyphosis
Cardiovascular/Metabolic:
- Hypertension
- Hyperglycemia / diabetes mellitus
- Hypokalemia (especially ectopic ACTH)
- Dyslipidemia
Endocrine/Reproductive:
- Amenorrhea, impotence
- Growth retardation in children
Neuropsychiatric:
- Depression, anxiety, cognitive dysfunction
- Rarely psychosis
Diagnosis
Diagnosis proceeds in two phases: (1) confirm hypercortisolism, then (2) determine the cause.
Phase 1 - Screening Tests (any one of three)
| Test | Principle | Notes |
|---|---|---|
| 24-hour urinary free cortisol (UFC) | Measures unbound cortisol filtered by glomerulus; integrated over 24 hrs | Upper normal ~110-138 nmol/24h (40-50 µg/day); values >4x ULN are diagnostic. May be falsely normal in ~10-15% of cases; unreliable in GFR <30 mL/min |
| Overnight low-dose dexamethasone suppression test (LD-DST) | 1 mg dexamethasone at midnight; cortisol measured at 8 AM. Failure to suppress = Cushing's | Dexamethasone corresponds to 3-4x physiologic glucocorticoid; not detected by cortisol assay |
| Late-night salivary cortisol (LNSC) | Takes advantage of loss of diurnal rhythm - cortisol fails to suppress at night even in mild Cushing's | Practical for outpatient use; 2 separate collections recommended |
- Henry's Clinical Diagnosis and Management, p. 1811-1814
- Campbell Walsh Wein Urology, p. 3137-3138
Phase 2 - Localizing the Cause
Once hypercortisolism is confirmed:
- Plasma ACTH level
- ACTH suppressed (undetectable/low) → ACTH-independent (adrenal cause) → proceed to adrenal imaging (CT)
- ACTH elevated/normal → ACTH-dependent → proceed to pituitary MRI
- High-dose dexamethasone suppression test (8 mg)
- Suppresses urinary cortisol by ≥90% → Cushing's disease (pituitary)
- No suppression → ectopic ACTH or adrenal source
-
CRH stimulation test - helps distinguish pituitary from ectopic ACTH
-
Inferior petrosal sinus sampling (IPSS) - gold standard for distinguishing pituitary Cushing's disease from ectopic ACTH when imaging is equivocal
-
Imaging: MRI pituitary (most adenomas are microadenomas <1 cm); CT/MRI abdomen for adrenal; whole-body imaging for ectopic source
Treatment
Treatment is dictated by the underlying cause.
Cushing's Disease (Pituitary Adenoma)
- First-line: Transsphenoidal pituitary microsurgery - curative in ~70-90% of microadenomas
- If surgery fails: repeat surgery, stereotactic radiosurgery, or bilateral adrenalectomy
- Nelson syndrome (progressive pituitary tumor growth after bilateral adrenalectomy) occurs in 8-29% of cases - prophylactic radiotherapy is controversial
Ectopic ACTH Syndrome
- Resect the primary tumor - possible in only ~10% of patients
- For unresectable tumors: bilateral adrenalectomy with lifelong steroid replacement
- Up to 35% of cases have no identifiable primary tumor
ACTH-Independent (Adrenal) Cushing's
- Unilateral adrenalectomy for solitary adenoma/carcinoma
- Bilateral adrenalectomy for AIMAH and PPNAD with lifelong replacement
Medical Therapy (bridge to surgery or when surgery not possible)
Steroidogenesis inhibitors:
- Metyrapone - most commonly used
- Ketoconazole
- Aminoglutethimide
- Etomidate (IV, for severe/urgent cases)
- Mitotane (adrenolytic - primarily for adrenal carcinoma)
- Mifepristone (glucocorticoid receptor antagonist)
Exogenous Cushing's
- Taper and discontinue glucocorticoid therapy when clinically possible
- Adrenal insufficiency during taper must be anticipated
Key Distinguishing Points
| Feature | Cushing's Disease | Ectopic ACTH | Adrenal Tumor |
|---|---|---|---|
| ACTH level | Elevated | Very elevated | Suppressed (low) |
| Dexamethasone suppression | Partial (high-dose) | No suppression | No suppression |
| Pigmentation | Mild | Pronounced | Absent |
| Hypokalemia | Mild | Severe | Absent/mild |
| Onset | Gradual | Rapid | Variable |
Pseudo-Cushing's Syndrome
A condition of HPA axis overactivity without true Cushing's syndrome. Seen in:
- Major depression
- Alcoholism
- Poorly controlled diabetes
- Morbid obesity
- Anxiety disorders
Mild UFC elevation can occur; distinguished by CRH + dexamethasone testing (Liddle test).
- Henry's Clinical Diagnosis and Management, p. 1814
Sources: Campbell Walsh Wein Urology (3-Volume Set), Adams and Victor's Principles of Neurology, 12th ed., Henry's Clinical Diagnosis and Management by Laboratory Methods, Tietz Textbook of Laboratory Medicine, 7th ed.
This is a shared conversation. Sign in to Orris to start your own chat.