Miliary tb full details for md exam answer 15 marks from this pdf and your data
Reading File
Reading File
Running Command
Finding Sources
Running Command
Finding Sources
Running Command
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Running Command
Loading Image
Finding Sources
Finding Sources
I now have comprehensive material. Let me write the complete 15-mark MD exam answer.
MILIARY TUBERCULOSIS — 15-Mark MD Exam Answer
DEFINITION
Miliary tuberculosis (TB) is a form of disseminated tuberculosis resulting from massive haematogenous spread of Mycobacterium tuberculosis to multiple organs simultaneously. The term derives from the Latin milium (millet seed), describing the gross appearance of innumerable small (1–3 mm) discrete granulomatous lesions that stud the lung parenchyma and other organs, resembling scattered millet seeds.
EPIDEMIOLOGY AND RISK FACTORS
- Accounts for ~1–2% of all TB cases but contributes disproportionately to TB mortality
- High-risk groups:
- Children < 5 years (impaired cellular immunity)
- Elderly
- HIV-infected individuals (most important risk factor in modern era)
- Immunocompromised: organ transplant recipients, haematological malignancies, lymphoma
- Those on corticosteroids, anti-TNF agents, immunosuppressives
- Alcohol use disorder, cirrhosis, end-stage renal disease
- Pregnancy, malnutrition, diabetes mellitus, silicosis
PATHOGENESIS
- Primary infection: M. tuberculosis inhaled → phagocytosed by alveolar macrophages → Ghon focus formed
- Bacteraemia: organisms drain to regional lymph nodes → lympho-haematogenous dissemination → seeding of multiple organs (lungs, liver, spleen, bone marrow, CNS, kidneys, adrenals)
- Failure of containment: when host cell-mediated immunity (CMI) is impaired, contained foci reactivate or primary infection progresses without control
- Granuloma formation: in each seeded site, non-caseating or caseating granulomas form; in miliary disease these granulomas are tiny (< 2 mm) and uniform — the pathological hallmark
- Two mechanisms of miliary TB:
- Primary miliary TB: massive dissemination shortly after initial infection (common in infants/immunocompromised)
- Reactivation miliary TB: reactivation of dormant foci with subsequent haematogenous spread (common in elderly/HIV)
PATHOLOGY
- Gross: Lungs and affected organs studded with tiny (1–3 mm) yellowish-white firm nodules, resembling millet seeds
- Histology: Multiple discrete epithelioid cell granulomas with Langhans giant cells; may show central caseation; acid-fast bacilli demonstrable on Ziehl-Neelsen (ZN) stain
- Organs involved: Lungs (most prominent), liver, spleen, bone marrow, meninges, adrenals, kidneys, choroid of eye
CLINICAL FEATURES
General / Constitutional
| Symptom | Frequency |
|---|---|
| Fever (often high-grade, remittent) | Very common |
| Anorexia and weight loss | Very common |
| Night sweats | Common |
| Malaise, weakness | Common |
Respiratory
- Dry cough (may be minimal)
- Progressive dyspnoea
- ARDS in fulminant form
Specific Signs
- Hepatosplenomegaly (granulomatous infiltration)
- Lymphadenopathy (generalised)
- Choroidal tubercles on fundoscopy — PATHOGNOMONIC for miliary TB (seen in ~13–87% of cases; bilateral, yellowish-white lesions near disc)
- Cutaneous lesions (more common in HIV): papules/vesiculopapules (tuberculosis cutis miliaris disseminata or tuberculosis cutis acuta generalisata)
- Signs of meningeal irritation if TB meningitis supervenes
Complications
- TB meningitis (most serious; occurs in ~30% of miliary TB)
- ARDS (fulminant miliary TB)
- Disseminated intravascular coagulation (DIC)
- SIADH → hyponatraemia
- Adrenal insufficiency (bilateral adrenal involvement)
- Pancytopenia (bone marrow infiltration)
DIAGNOSIS
1. Chest X-Ray (CXR)
- Classic finding: diffuse bilateral micronodular (1–3 mm) shadows uniformly distributed throughout both lung fields — the "snowstorm" pattern
- May be absent in up to 50% of cases in early disease — do not exclude miliary TB on the basis of a normal CXR
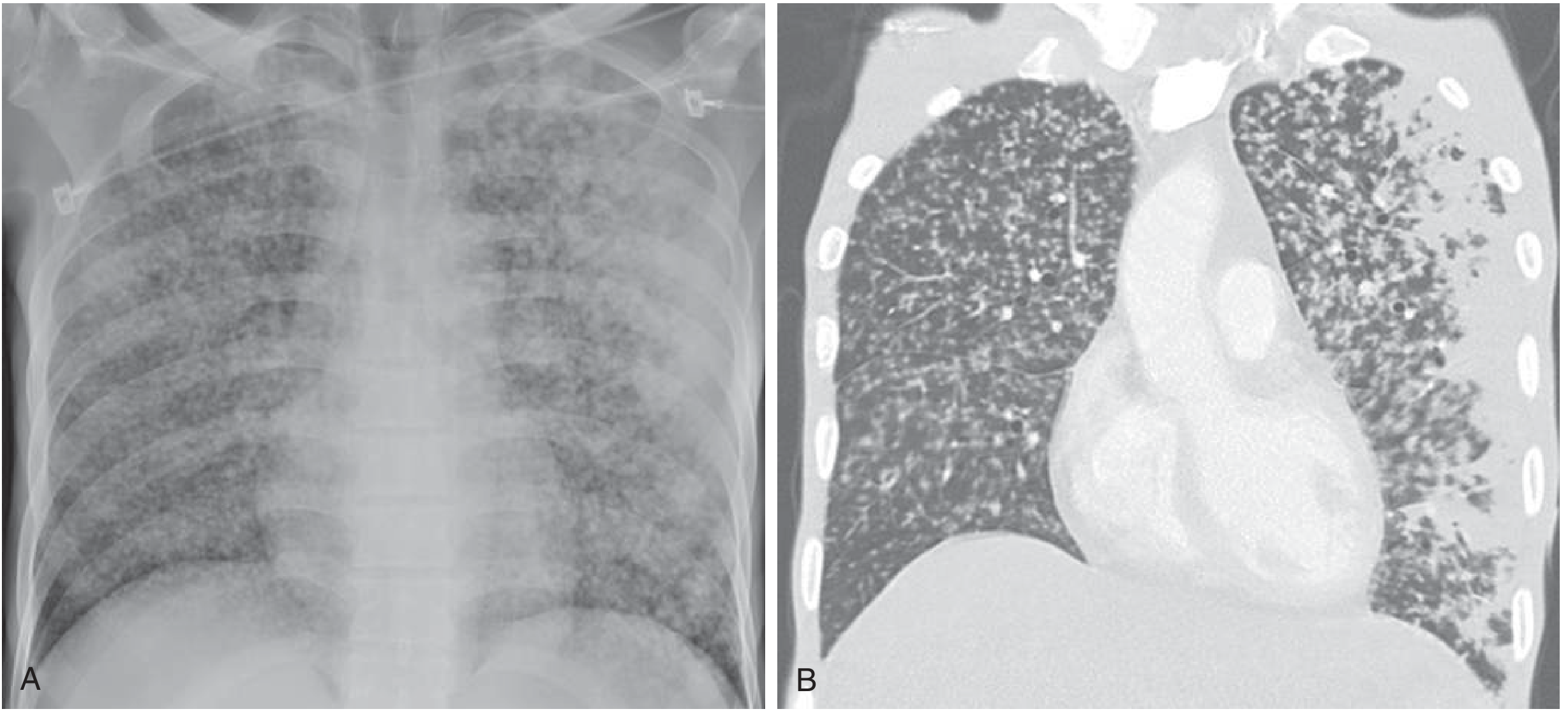
2. HRCT Chest
- More sensitive than plain CXR
- Shows random distribution of 1–3 mm nodules throughout both lungs (as opposed to perilymphatic or centrilobular in other conditions)
3. Sputum Smear & Culture
- AFB smear positive in only 20–40% of miliary TB cases
- M. tuberculosis culture remains the gold standard (6–8 weeks; BACTEC MGIT: 2–3 weeks)
- Bronchoscopy with BAL and transbronchial biopsy increases yield when sputum is inadequate
4. Tuberculin Skin Test (TST / Mantoux)
- Often negative (anergy) in miliary TB due to severe immunosuppression — do not use to exclude disease
5. IGRA (Interferon-γ Release Assay)
- More specific than TST but sensitivity similar; may yield indeterminate results in miliary TB
- A negative TST or IGRA does NOT exclude miliary TB
6. Blood Tests
- CBC: anaemia (normocytic/normochromic), leukopenia or leukocytosis, thrombocytopenia (if bone marrow involved)
- ESR elevated
- LFTs: elevated ALP, transaminases (hepatic granulomas)
- Serum Na⁺: hyponatraemia due to SIADH (common, especially if meningitis present)
- LDH elevated
7. Fundoscopy
- Choroidal tubercles — pathognomonic; bilateral, pale/yellow, discrete lesions adjacent to optic disc
8. Biopsy (Highest Diagnostic Yield in Difficult Cases)
| Biopsy Site | Yield |
|---|---|
| Liver (AFB smear + culture + PCR) | Highest yield |
| Bone marrow | High (especially if pancytopenic) |
| Lymph node | Useful if lymphadenopathy present |
| Transbronchial | Useful with bronchoscopy |
- All biopsies show epithelioid granulomas with or without caseation; ZN stain for AFB
9. Lumbar Puncture
- Mandatory if meningism suspected
- CSF: lymphocytic pleocytosis, raised protein, low glucose (CSF:serum glucose < 0.5), AFB smear/culture
10. Nucleic Acid Amplification Tests (NAAT/PCR)
- GeneXpert MTB/RIF on sputum or BAL — detects M. tuberculosis DNA within 2 hours; also detects rifampicin resistance
- Mycobacterial PCR on biopsied tissue shortens time to diagnosis
DIFFERENTIAL DIAGNOSIS OF MILIARY PATTERN ON CXR
| Condition | Features |
|---|---|
| Histoplasmosis | Fungal; endemic areas; serology helpful |
| Sarcoidosis | Perilymphatic nodules; raised ACE; non-caseating granulomas |
| Miliary metastases | Malignancy history; variable nodule size |
| Pneumoconiosis (siderosis) | Occupational history |
| Disseminated fungal infection | Cryptococcus, Coccidioides |
| Langerhans cell histiocytosis | Upper lobe predominance |
TREATMENT
Regimen (Same as Other Forms of Active TB)
Intensive Phase (2 months) — HRZE:
| Drug | Daily Dose |
|---|---|
| Isoniazid (H) | 5 mg/kg (max 300 mg) |
| Rifampicin (R) | 10 mg/kg (max 600 mg) |
| Pyrazinamide (Z) | 25 mg/kg (max 2 g) |
| Ethambutol (E) | 15 mg/kg (max 1.6 g) |
Continuation Phase (7–10 months) — HR:
- Standard TB: 4 months HR
- Miliary TB: 7–10 months total (extended due to severity)
- CNS/meningeal involvement: minimum 12 months total
Corticosteroids
- Indicated in: miliary TB with meningitis, ARDS, severe hypoxia, adrenal insufficiency, pericarditis
- Prednisolone 1–2 mg/kg/day × 4–6 weeks, then taper
- Reduces complications and mortality in TB meningitis
Pyridoxine (Vitamin B6)
- 10–25 mg/day with isoniazid to prevent peripheral neuropathy
Supportive Care
- Nutritional support
- Correction of hyponatraemia (fluid restriction for SIADH)
- Respiratory support (oxygen, mechanical ventilation in ARDS)
- Treatment of adrenal insufficiency with hydrocortisone
Key Principle
Initiate treatment immediately on clinical suspicion — do NOT wait for microbiological confirmation. Delay in treatment is the leading cause of the high mortality (~21%) in miliary TB.
PROGNOSIS
- Mortality: ~21% even in the antibiotic era (higher with delayed treatment, CNS involvement, ARDS, or DIC)
- With prompt treatment: good response expected in most immunocompetent patients
- HIV co-infection worsens prognosis
- Fulminant miliary TB with ARDS/DIC carries very high mortality
SUMMARY TABLE — MILIARY TB AT A GLANCE
| Feature | Key Point |
|---|---|
| Definition | Haematogenous dissemination of MTB to multiple organs |
| Lesion | 1–3 mm granulomas resembling millet seeds |
| Pathognomonic sign | Choroidal tubercles on fundoscopy |
| CXR | Bilateral diffuse 1–3 mm nodules ("snowstorm"); absent in 50% early |
| TST/Mantoux | Often false negative (anergy) |
| Best diagnostic yield | Liver biopsy + AFB smear/culture/PCR |
| Treatment | 2HRZE + 7–10 HR; steroids if meningitis/ARDS |
| Mortality | ~21% |
Sources: Goldman-Cecil Medicine (ELSEVIER 2024), Rosen's Emergency Medicine, Tintinalli's Emergency Medicine, Harrison's Principles of Internal Medicine 22e (McGraw-Hill 2025), Robbins Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.