Calcium and its disorders in pediatrics, detail explanation, in simple language - mbbs final year , pedia
Reading File
Finding Sources
Finding Sources
Searching the Web
calcium disorders pediatrics hypocalcemia hypercalcemia MBBS overview 2024
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have all the information needed. Let me put together a comprehensive, exam-focused response for an MBBS final year student.
Calcium and Its Disorders in Pediatrics
A Simple, Complete Guide for MBBS Final Year
1. Why Calcium Matters
Calcium is the most abundant mineral in the body. It does five key things:
- Builds and strengthens bones and teeth (stored as hydroxyapatite)
- Triggers muscle contraction (cardiac and skeletal)
- Enables nerve signal transmission
- Drives hormone secretion and intracellular signaling
- Supports immune function
2. Normal Calcium Values (Know These!)
| Parameter | Normal Range |
|---|---|
| Total serum calcium | 8.5 - 10.5 mg/dL |
| Ionized (free) calcium | 4.5 - 5.5 mg/dL (1.1 - 1.4 mmol/L) |
| Neonates (first week) | Slightly lower; 7 - 12 mg/dL |
Exam tip: In blood, calcium exists in 3 forms:
- ~45% bound to albumin (inactive)
- ~10% bound to anions like phosphate (inactive)
- ~45% ionized = the biologically active form
Corrected calcium formula (used when albumin is low):
Corrected Ca = Measured Ca + 0.8 × (4 - serum albumin in g/dL)
3. How the Body Regulates Calcium
This is the foundation. Understand the PTH-Vitamin D axis thoroughly.
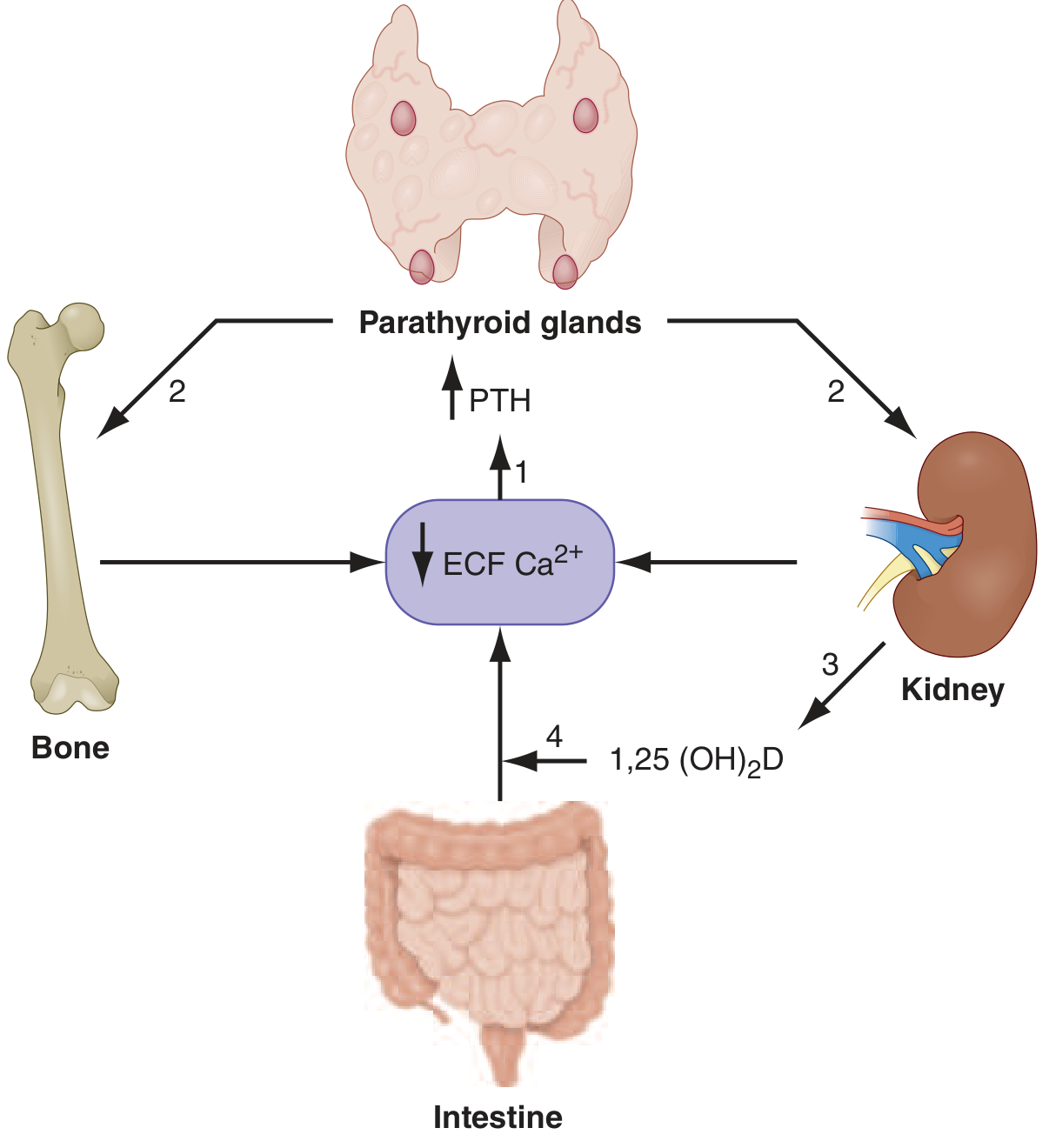
When calcium falls:
- Parathyroid glands sense low Ca via the Calcium-Sensing Receptor (CaSR) → secrete PTH
- PTH acts on:
- Bone → increases osteoclast activity → releases Ca and phosphate
- Kidney → increases Ca reabsorption in distal tubule; increases phosphate excretion; activates vitamin D
- Kidney → converts 25(OH)D to 1,25(OH)₂D (calcitriol) via 1α-hydroxylase
- Calcitriol acts on the intestine → increases dietary calcium absorption
- All three effects together raise serum calcium back to normal
- High calcium → shuts off PTH secretion (negative feedback)
Simple memory: PTH = "Phosphate Tossed out, calcium Held in"
4. HYPOCALCEMIA
Definition
- Total serum Ca < 8.5 mg/dL (or ionized Ca < 4.5 mg/dL)
- In neonates: Ca < 7.0 mg/dL (term) or < 7.5 mg/dL (preterm)
Classification - Very Important for Exams
A. By PTH Level
| PTH Low (Hypoparathyroidism) | PTH High (Secondary Hyperparathyroidism) |
|---|---|
| DiGeorge syndrome | Vitamin D deficiency (rickets) |
| Autoimmune hypoparathyroidism (APS-1) | Chronic kidney disease |
| Post-surgical (parathyroid damage) | Malabsorption syndromes |
| Genetic: GCM2, GATA3, PTH gene mutations | Pseudohypoparathyroidism |
| Magnesium deficiency (suppresses PTH) | Hyperphosphatemia |
B. By Age Group (pediatric-specific)
Neonatal Hypocalcemia - the most common Ca disorder in neonates:
| Early Neonatal (Day 1-3) | Late Neonatal (Day 4-10) |
|---|---|
| Prematurity (most common) | High phosphate cow's milk formula |
| Infant of diabetic mother (IDM) | Hypoparathyroidism (DiGeorge) |
| Perinatal asphyxia | Maternal vitamin D deficiency |
| Maternal hyperparathyroidism | Hypomagnesemia |
| Sepsis, RDS |
IDM hypocalcemia mechanism: Maternal hyperglycemia → fetal hyperinsulinism → calcitonin release → calcium falls. Also maternal hyperparathyroidism suppresses fetal PTH glands.
Older children:
- Vitamin D deficiency rickets - most common cause in India
- Celiac disease / malabsorption
- Hypoparathyroidism (genetic, autoimmune)
- Pseudohypoparathyroidism (PTH resistance, Albright's hereditary osteodystrophy)
- Chronic kidney disease
- Alkalosis - hyperventilation increases calcium binding to albumin → ionized Ca falls → tetany
Clinical Features - "Think CATS"
C - Convulsions / Cramps
A - Arrhythmias (prolonged QTc)
T - Tetany
S - Spasms (laryngospasm, bronchospasm)
More specifically:
- Neuromuscular irritability - tingling, numbness of hands/feet/lips
- Tetany - sustained painful muscle spasm
- Trousseau's sign - inflate BP cuff above systolic for 3 min → carpopedal spasm (carpal tunnel squeezing - thumb adduction, finger flexion) → positive
- Chvostek's sign - tap facial nerve anterior to ear → ipsilateral facial muscle twitch → positive (less specific)
- Laryngospasm - "crowing" breathing, can be life-threatening in infants
- Seizures - a major cause of neonatal seizures
- Prolonged QTc on ECG → risk of arrhythmia
- Papilledema in chronic cases (raised ICP)
- Cataracts in long-standing hypoparathyroidism
- Dental hypoplasia, dry skin, brittle nails in chronic cases
Investigations
| Test | Finding |
|---|---|
| Serum calcium | Low (<8.5 mg/dL) |
| Serum phosphate | High if hypoparathyroidism or CKD; Low if vitamin D deficiency |
| Serum PTH | Low (hypoparathyroidism) or High (secondary) |
| Serum 25(OH)D | Low in vitamin D deficiency |
| Serum Mg | Check - hypomagnesemia causes PTH suppression |
| Urinary calcium | Low (appropriate conservation) |
| ECG | Prolonged QTc interval |
| X-ray wrist | Cupping, fraying of metaphysis in rickets |
Phosphate levels help narrow the diagnosis:
- Low Ca + High PO4 + Low PTH = Hypoparathyroidism
- Low Ca + High PO4 + High PTH = Pseudohypoparathyroidism or CKD
- Low Ca + Low PO4 + High PTH = Vitamin D deficiency (rickets)
Treatment
Acute / Symptomatic (tetany, seizures, laryngospasm):
- IV Calcium gluconate 10%: 1-2 mL/kg (max 10 mL) slow IV over 10-20 min
- ECG monitoring during infusion (can cause arrhythmia if given too fast)
- Followed by calcium gluconate infusion: 2-4 mg/kg/hr
Chronic / Maintenance:
- Oral calcium carbonate or calcium gluconate supplements
- Vitamin D (cholecalciferol / calcitriol) depending on cause
- In hypoparathyroidism: calcitriol (active form) because cannot activate vitamin D
- Treat underlying cause (e.g., correct Mg, treat rickets, DiGeorge management)
5. HYPERCALCEMIA
Definition
- Total serum Ca > 10.5 mg/dL
- Severe: > 14 mg/dL (hypercalcemic crisis)
- Less common than hypocalcemia in pediatrics
Causes in Children (PTH-based classification)
PTH High (Hyperparathyroidism-related):
- Primary hyperparathyroidism - parathyroid adenoma (rare in children), MEN syndromes
- Familial Hypocalciuric Hypercalcemia (FHH) - CaSR mutation → PTH inappropriately normal/high with mild hypercalcemia; benign, urine calcium LOW
- Tertiary hyperparathyroidism - chronic CKD with autonomous PTH secretion
PTH Low (PTH-independent):
- Malignancy (second most common cause with hyperparathyroidism together = 80-90% of cases)
- Solid tumors: PTHrP (PTH-related peptide) mimics PTH
- Leukemia/lymphoma: osteolytic lesions or excess 1,25(OH)₂D production
- Vitamin D intoxication - excessive supplementation (common in India now with over-supplementation)
- Granulomatous diseases - TB, sarcoidosis - macrophages make excess 1,25(OH)₂D
- Williams syndrome - hypersensitivity to vitamin D (deletion 7q11)
- Subcutaneous fat necrosis of newborn - ectopic calcitriol production
- Immobilization - increased bone resorption
- Ketogenic diet for epilepsy in children
Clinical Features - "Bones, Stones, Groans, Moans, Thrones"
| Mnemonic | System | Symptoms |
|---|---|---|
| Bones | Skeletal | Bone pain, pathological fractures, subperiosteal resorption |
| Stones | Renal | Nephrolithiasis, nephrocalcinosis, polyuria, polydipsia |
| Groans | GI | Nausea, vomiting, constipation, anorexia, peptic ulcers |
| Moans | Neuro/Psych | Lethargy, depression, confusion, weakness, stupor |
| Thrones | (bonus) | Renal failure (sitting on the throne = passing water = renal effects) |
ECG: Shortened QTc (opposite of hypocalcemia)
Severe/crisis: Altered consciousness, coma, arrhythmias
Investigations
| Test | Finding |
|---|---|
| Serum calcium | > 10.5 mg/dL |
| Serum PTH | High = primary HPT; Low = PTH-independent |
| Serum PTHrP | High in malignancy (humoral hypercalcemia) |
| Serum 25(OH)D | High in vitamin D toxicity |
| Urinary calcium | High (hypercalciuria) - EXCEPT in FHH (low) |
| Serum phosphate | Low in primary HPT; variable others |
| Serum ALP | High in HPT / bone disease |
| X-ray skull/hand | "Salt and pepper" skull, subperiosteal resorption in HPT |
| US abdomen | Nephrolithiasis, nephrocalcinosis |
| DEXA scan | Reduced bone density |
FHH (Familial Hypocalciuric Hypercalcemia) vs Primary HPT:
- Both have high (or normal) PTH + high calcium
- FHH: urine calcium/creatinine ratio < 0.01 (kidneys retain calcium due to CaSR mutation)
- Primary HPT: urine calcium HIGH
Treatment
Mild asymptomatic (Ca 10.5-12):
- Treat underlying cause
- Adequate hydration, avoid thiazides and vitamin D supplements
- FHH: no treatment needed (benign)
Moderate to severe / symptomatic:
-
IV Normal Saline hydration - first and most important step
- Expands volume, promotes renal calcium excretion
- Rate: 10-20 mL/kg bolus, then maintenance + replacement
-
Loop diuretics (furosemide) - after adequate hydration
- Blocks Ca reabsorption in loop of Henle → calciuresis
- Never give before hydration (worsens hypercalcemia)
-
Bisphosphonates (pamidronate, zoledronate)
- Inhibit osteoclast-mediated bone resorption
- Drug of choice for malignancy-associated hypercalcemia
-
Calcitonin - rapid onset (hours), short duration
- Inhibits bone resorption + increases renal Ca excretion
- Useful as a bridge while awaiting bisphosphonate effect
-
Corticosteroids - for granulomatous disease, lymphoma, vitamin D toxicity
- Inhibit macrophage CYP27B1, reduce 1,25(OH)₂D production
-
Cinacalcet (calcimimetic) - for primary HPT or tertiary HPT
- Activates CaSR, suppresses PTH
- Used in some pediatric cases with HPT
-
Dialysis - for renal failure + severe refractory hypercalcemia
-
Surgery (parathyroidectomy) - for confirmed primary HPT
6. Quick Comparison Table (Exam Favorite)
| Feature | Hypocalcemia | Hypercalcemia |
|---|---|---|
| Definition | Ca < 8.5 mg/dL | Ca > 10.5 mg/dL |
| Neuromuscular | Tetany, Chvostek, Trousseau, seizures | Weakness, hypotonia, stupor |
| ECG | Prolonged QTc | Shortened QTc |
| GI | None significant | Nausea, vomiting, constipation |
| Renal | None (may conserve Ca) | Polyuria, stones, nephrocalcinosis |
| Bone | Rickets (in D deficiency) | Osteitis fibrosa cystica (HPT) |
| Most common cause (neonate) | Prematurity / IDM | Iatrogenic / subcutaneous fat necrosis |
| Most common cause (older child) | Vitamin D deficiency | Primary HPT / malignancy |
| Immediate Rx | IV Calcium gluconate | IV Normal saline |
7. Pediatric High-Yield Points for Exams
-
DiGeorge syndrome (22q11 deletion) - absent thymus + absent parathyroids → immunodeficiency + hypocalcemia. Features: Conotruncal heart defects, dysmorphic face, hypocalcemia, T-cell deficiency.
-
Pseudohypoparathyroidism (PHP) - PTH is high but organs don't respond (PTH resistance). Look for Albright's hereditary osteodystrophy: short stature, short 4th metacarpal, obesity, round face, subcutaneous calcifications. Calcium low, phosphate high, PTH very high.
-
Hypomagnesemia causes hypocalcemia by suppressing PTH release - always check Mg in resistant hypocalcemia. Treat Mg first.
-
Williams syndrome - "elfin facies," supravalvular aortic stenosis, hypercalcemia, intellectual disability. Caused by chromosome 7q11 deletion.
-
Subcutaneous fat necrosis of newborn - large neonate, traumatic delivery → hard plaques on back/buttocks in first weeks → hypercalcemia due to ectopic 1,25(OH)₂D production. Can cause severe hypercalcemia - restrict dietary calcium and vitamin D.
-
Vitamin D deficiency rickets - most common metabolic bone disease in children in India.
- Cause: poor sunlight, dark skin, exclusively breastfed without supplementation, maternal deficiency
- Lab: low Ca, low PO4, high PTH, high ALP, low 25(OH)D
- X-ray: cupping and fraying of metaphysis (especially distal radius), Looser zones
- Treatment: Vitamin D 2000-4000 IU/day (Stoss therapy: single 600,000 IU dose)
-
Neonatal Trousseau / Chvostek - less reliable in neonates; seizures and apnea are the typical presentation.
-
ECG monitoring is mandatory during IV calcium infusion due to risk of bradycardia and cardiac arrest if pushed too fast.
8. Summary Flowchart
Low Calcium (Hypocalcemia)
↓
Check PTH
/ \
Low PTH High PTH
↓ ↓
Hypoparathyroidism Check Phosphate & Vit D
(DiGeorge, / \
autoimmune, High PO4 Low PO4
post-op, Low Vit D Low Vit D
genetic) ↓ ↓
CKD/PHP Vitamin D
Deficiency/Rickets
Sources: Harrison's Principles of Internal Medicine 22E, 2025 (McGraw Hill) - Chapter 57 on Calcium Disorders; Rosen's Emergency Medicine; Brenner & Rector's The Kidney.
This is a shared conversation. Sign in to Orris to start your own chat.