Fistula
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive content to compile a thorough answer. Let me compose the full response.
Fistula - Comprehensive Overview
Definition
A fistula is an abnormal communication between two epithelium-lined surfaces. The tract is usually lined by granulation tissue but may become epithelialised in chronic cases. Fistulae may be congenital (e.g., tracheo-oesophageal, branchial) or acquired (e.g., enterocutaneous from Crohn's disease or surgery, arteriovenous for dialysis access).
- Bailey and Love's Short Practice of Surgery, 28th Ed.
Classification by Type
| Type | Connection | Common Examples |
|---|---|---|
| Enterocutaneous | Bowel to skin | Post-operative, Crohn's |
| Rectovaginal | Rectum to vagina | Obstetric trauma, IBD, radiation |
| Vesicovaginal | Bladder to vagina | Obstetric injury, surgery |
| Arteriovenous (AV) | Artery to vein | Congenital, dialysis access, trauma |
| Tracheoesophageal | Trachea to oesophagus | Congenital, malignancy |
| Pharyngocutaneous | Pharynx to skin | Post-laryngectomy complication |
| Anal (fistula-in-ano) | Anal canal to perianal skin | Cryptoglandular abscess, Crohn's |
| Obstetric/Genitourinary | Genitourinary tract | Prolonged obstructed labour |
| Aortoenteric | Aorta to GI tract | Post-aortic graft, erosion |
Fistula-in-Ano (Anal Fistula)
Pathogenesis
Fistula-in-ano results from persistent communication between the cryptoglandular complex in the anal canal (internal opening) and the perianal skin (external opening) after spontaneous or surgical drainage of a perianal abscess. Approximately 50% of patients with a perianal abscess will ultimately develop a fistula. - Sabiston Textbook of Surgery
Parks Classification
The standard classification system divides anal fistulae into four types based on their relationship to the anal sphincter complex:
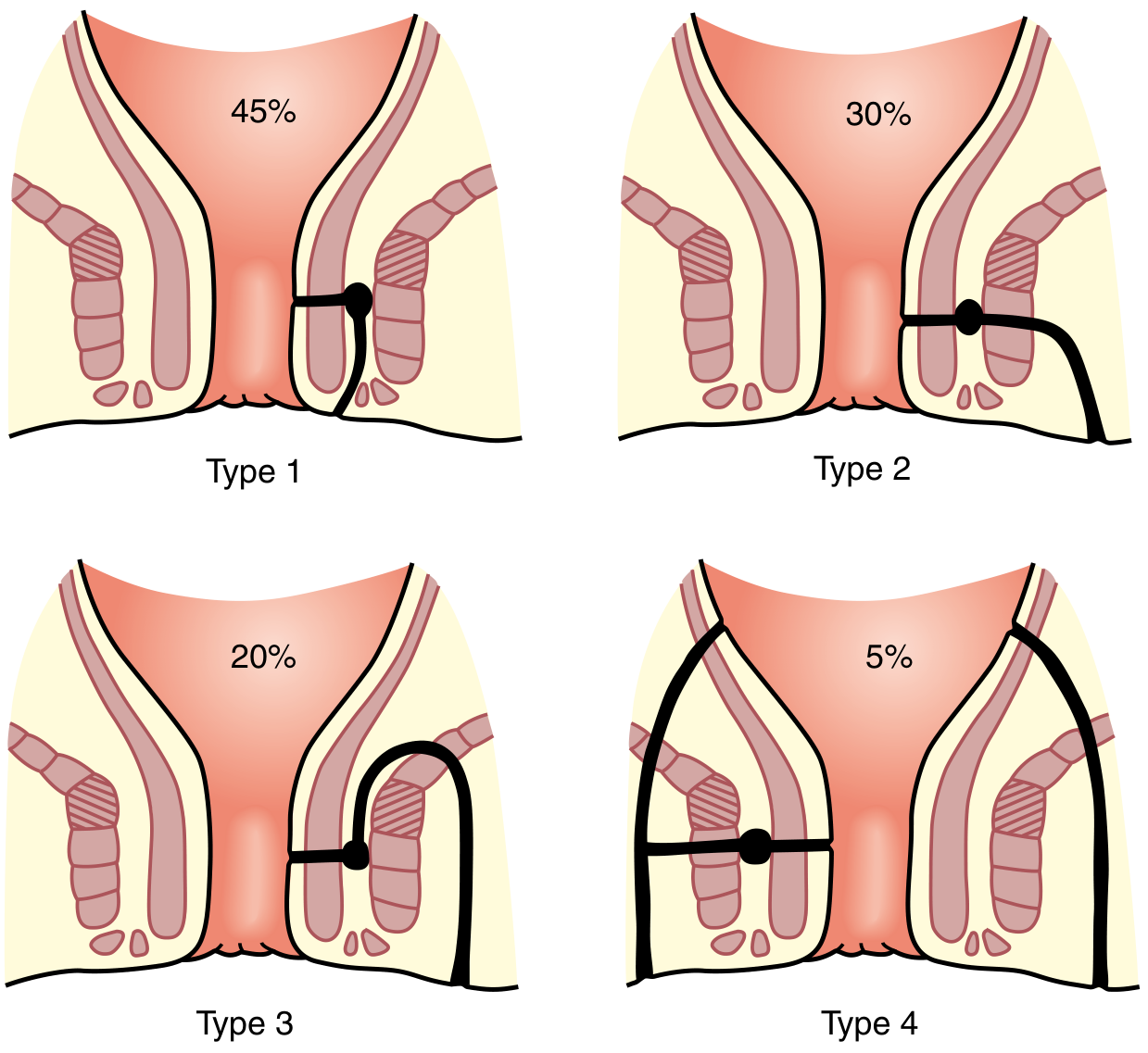
| Type | Name | Frequency | Description |
|---|---|---|---|
| Type 1 | Intersphincteric | 45% | Tracks between internal and external sphincters |
| Type 2 | Transsphincteric | 30% | Crosses the external sphincter |
| Type 3 | Suprasphincteric | 20% | Goes above the puborectalis |
| Type 4 | Extrasphincteric | 5% | Entirely outside the sphincter mechanism |
Goodsall's Rule
- External opening anterior to transverse anal line → track runs radially to the internal opening
- External opening posterior → track curves to a posterior midline internal opening
- Exception: anterior openings >3 cm from anal verge may curve posteriorly (horseshoe fistula)
Diagnosis
- Clinical: chronic perianal drainage, cyclical pain/swelling relieved by discharge
- Physical exam: cordlike subcutaneous structure, external opening(s)
- "Watering can perineum" (multiple openings) suggests perianal Crohn's disease
- MRI with anal fistula protocol is the gold standard for complex anatomy
MRI of anal fistulae - axial T2-weighted images:
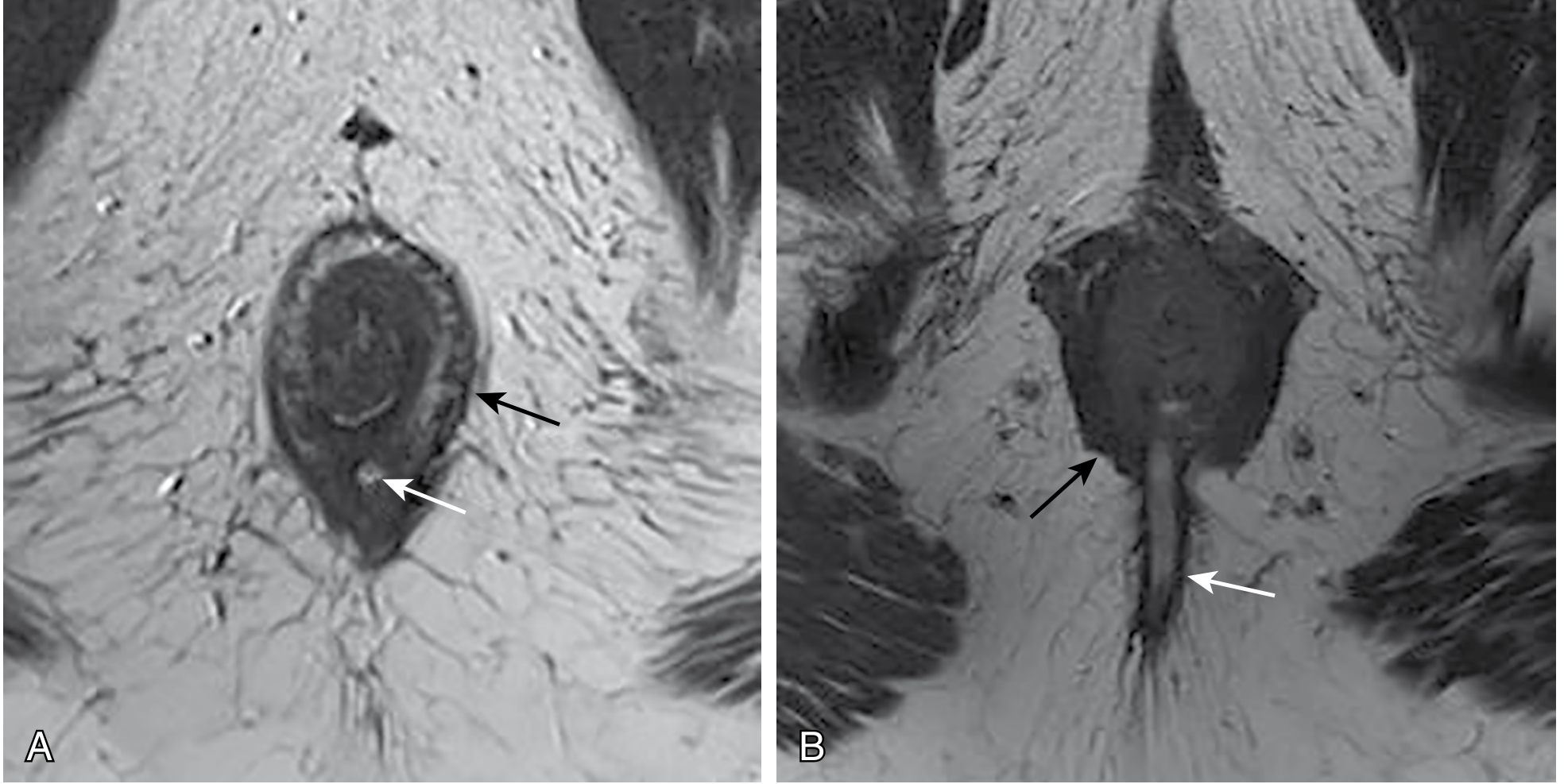
(A) Intersphincteric fistula (white arrow) lying within the intersphincteric plane. (B) Transsphincteric fistula (white arrow) penetrating the external sphincter boundary.
Treatment Goals (Anal Fistula)
- Treat any undrained infection
- Define fistula anatomy
- Remove or ablate epithelialised tracts
- Avoid or minimise risk of fecal incontinence
- Prevent recurrence
Surgical options:
-
Fistulotomy (lay-open): For low-lying fistulae involving <1/3 of the external sphincter (intersphincteric/low transsphincteric). Fecal incontinence risk <5% with normal preoperative sphincter function; recurrence rate 2-8%.
-
Seton: A suture/drain placed through the tract; used as a cutting or draining seton for complex/high fistulae to protect continence
-
Advancement flap: Mucosal or full-thickness flap to close the internal opening
-
LIFT procedure (Ligation of Intersphincteric Fistula Tract)
-
Bioprosthetic plug, fibrin glue, video-assisted anal fistula treatment (VAAFT)
-
Sabiston Textbook of Surgery
Enterocutaneous Fistula (ECF)
Causes
- 75-80% are post-surgical complications (anastomotic leak, inadvertent bowel injury)
- Pre- or post-surgical malnutrition is a major risk factor
- Crohn's disease, radiation, cancer, foreign body
Output Classification
| Class | Output | Clinical significance |
|---|---|---|
| Low output | <200 mL/day | More likely to close spontaneously |
| Medium output | 200-500 mL/day | Variable |
| High output | >500 mL/day | Significant fluid/electrolyte loss, skin excoriation from digestive enzymes, difficult to manage |
Conservative Management ("SNAP" principles)
- Skin care - protect surrounding skin from corrosive secretions
- Nutrition - parenteral or enteral nutrition is critical; high-output fistulae worsen malnutrition
- Anatomy - contrast sinogram/fistulogram, CT scan to delineate tract
- Plan - identify spontaneous closure potential vs. need for surgery
Conservative measures:
- Nil by mouth, nasogastric drainage
- IV fluid and electrolyte replacement (especially for high-output)
- Total parenteral nutrition (TPN)
- Somatostatin analogues (octreotide) to reduce output
- Wound/stoma care with collection devices
Contraindications to spontaneous closure (mnemonic FRIEND):
-
Foreign body in tract
-
Radiation damage
-
Inflammation (IBD, abscess)
-
Epithelialisation of tract
-
Neoplasm
-
Distal obstruction
-
Pye's Surgical Handicraft; Yamada's Textbook of Gastroenterology
Arteriovenous Fistula (AVF)
Types
- Congenital AV fistulae - developmental malformations
- Acquired AV fistulae - trauma (penetrating injury causing artery-to-vein communication), iatrogenic (post-catheterisation), neoplastic erosion
- Surgically created AVF - for hemodialysis access
Hemodialysis AVF
The surgically created AVF is the preferred vascular access for hemodialysis ("fistula first" principle from KDOQI guidelines). Common configurations:
- Radiocephalic (Brescia-Cimino) - wrist, first choice
- Brachiocephalic - antecubital
- Brachiobasilic - requires transposition
AVF advantages over AV graft (AVG):
- Lower infection risk
- Better long-term patency
- No prosthetic material
However, AVF requires 6 months maturation time before use. Factors negatively affecting AVF maturation and patency: female sex, coronary artery disease, diabetes, obesity, elderly patients.
Key complications of AVF:
-
Stenosis/thrombosis (most common)
-
Steal syndrome causing distal ischemia
-
Venous hypertension
-
Aneurysm/pseudoaneurysm
-
Infection
-
High-output cardiac failure (rare, with large AV connections)
-
Sabiston Textbook of Surgery, 25th Ed.
Head & Neck Fistulae (Pharyngocutaneous)
Context
A common complication after laryngectomy, glossectomy, neck dissection, or other ablative head/neck surgery. Forms an abnormal connection between the pharynx/aerodigestive tract and the surrounding neck/skin.
Risk Factors
- Prior radiation therapy
- Malnutrition
- Postoperative hypothyroidism
Consequences
- Prolonged open wounds
- Severe infections
- Carotid blowout (most devastating - saliva and bacteria pooling near great vessels)
Management
- Conservative: Local wound care, debridement, strict NPO with enteral feeding (NG or gastrostomy), dry packing. Barium swallow to confirm closure before resuming oral intake.
- Surgical: Required for uncontrolled infection, systemic sepsis, or proximity to carotid. Pectoralis major muscle flap is the gold standard for large fistula closure.
Prevention: Use of vascularized tissue (pedicled pectoralis, radial forearm or anterolateral thigh free flap) to reinforce pharyngeal closure significantly reduces pharyngocutaneous fistula risk.
- Sabiston Textbook of Surgery
Factors Preventing Fistula Closure (General)
Any fistula is unlikely to close spontaneously if:
- There is distal obstruction to flow
- A foreign body is present in the tract
- The tract is epithelialised
- There is active disease (malignancy, active IBD, radiation necrosis)
- There is an abscess cavity that has not been drained
- The fistula has a short, straight, wide-bore tract
Summary Table: Common Fistulae
| Fistula | Aetiology | Key Investigation | Treatment |
|---|---|---|---|
| Fistula-in-ano | Cryptoglandular abscess, Crohn's | MRI pelvis | Fistulotomy, seton, advancement flap |
| Enterocutaneous | Post-operative, IBD | CT/sinogram | SNAP, surgery if no spontaneous closure |
| Rectovaginal | Obstetric, IBD, radiation | Examination, MRI | Advancement flap, colostomy |
| Vesicovaginal | Obstetric, gynaecologic surgery | Cystoscopy, CT urogram | Surgical repair (open/laparoscopic) |
| AVF (dialysis) | Surgical creation | Duplex USS | Maturation procedures, angioplasty if stenotic |
| Pharyngocutaneous | Post-laryngectomy | Barium swallow, CT neck | Conservative / pectoralis flap |
| Tracheoesophageal | Congenital, malignancy | Bronchoscopy, endoscopy | Stenting, surgical repair |
This is a shared conversation. Sign in to Orris to start your own chat.