Head injury for nurses
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Searching Images
head injury types epidural subdural hematoma brain CT scan
Now I have comprehensive content to write a thorough nursing-focused guide on head injury. Let me compile the full answer:
Head Injury — Nursing Guide
1. Definitions & Terminology
| Term | Meaning |
|---|---|
| Head trauma | Any external trauma to the craniofacial area (blunt, penetrating, blast, rotational, acceleration-deceleration) |
| Head injury | Clinically evident injury on exam — ecchymosis, laceration, deformity |
| Traumatic brain injury (TBI) | Actual injury to the brain parenchyma itself |
| Primary injury | Damage occurring at the moment of impact |
| Secondary injury | Subsequent systemic insults (hypoxia, hypotension, raised ICP) that worsen outcome |
The nurse's primary aim in TBI care is preventing secondary brain injury, because primary injury is not reversible. — Rosen's Emergency Medicine, p. 367
2. Classification by Severity (GCS-based)
| Severity | GCS Score | Key Features |
|---|---|---|
| Mild (concussion/MTBI) | 13–15 | LOC < 30 min, post-traumatic amnesia < 24 h, feeling dazed/confused |
| Moderate | 9–12 | Longer LOC, more prominent neurological deficits |
| Severe | 3–8 | Coma; high risk of death/disability |
Glasgow Coma Scale (GCS) — Full Scoring Table
| Eye Opening | Score | Verbal Response | Score | Motor Response | Score |
|---|---|---|---|---|---|
| Spontaneous | 4 | Oriented | 5 | Obeys commands | 6 |
| To speech | 3 | Confused | 4 | Localizes pain | 5 |
| To pain | 2 | Inappropriate words | 3 | Withdraws from pain | 4 |
| None | 1 | Incomprehensible | 2 | Flexion (decorticate) | 3 |
| None | 1 | Extension (decerebrate) | 2 | ||
| No response | 1 |
GCS range: 3–15. The motor score carries the most prognostic weight. Assess before sedation/paralysis are given; reassess every 30 minutes or with any mental status change.
— Sabiston Textbook of Surgery, p. 803
3. Types of Head Injury
3a. Concussion (MTBI)
- Functional, not structural, brain injury from shaking/impact
- Standard CT/MRI are normal — imaging not required for pure concussion
- Symptoms: headache, dizziness, cognitive slowing, sleep disturbance, emotional changes
- Management: 24–48 h of rest, then graded return to activity (bed rest is no longer recommended)
- All children with concussion need monitoring by a primary care physician or concussion specialist
3b. Epidural Hematoma (EDH)
- Arterial bleed (usually middle meningeal artery) between skull and dura
- Caused by skull fracture crossing the meningeal groove
- Classic presentation: lucid interval → sudden deterioration
- Only 15–20% have this classic pattern; many have minimal initial symptoms
- Rapid progression: headache → impaired consciousness → herniation signs within hours
- CT appearance: biconvex (lens-shaped) hyperdense collection
- Look for signs of basal skull fracture: Battle's sign (mastoid bruising), raccoon eyes (periorbital bruising), blood behind tympanic membrane
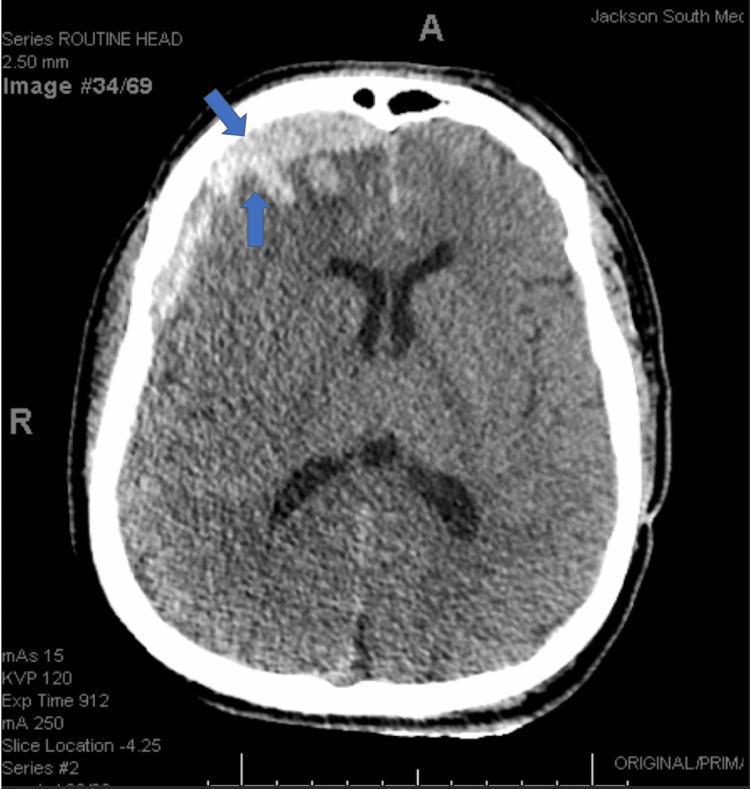
3c. Subdural Hematoma (SDH)
- Venous bleed from torn bridging veins between brain and dural sinuses
- More common in elderly (brain atrophy stretches bridging veins) and patients on anticoagulants
- Develops more slowly; may wax and wane
- CT appearance: crescent-shaped hyperdense collection following the brain surface
- Warfarin/clopidogrel users with even minor head injury → immediate non-contrast CT regardless of symptoms; check INR
3d. Diffuse Axonal Injury (DAI)
- Shearing of axons from rotational forces (e.g., motor vehicle crashes)
- More common in children due to less myelination and higher brain water content
- CT may appear normal or show small petechial hemorrhages
- Associated with prolonged coma and poor outcome
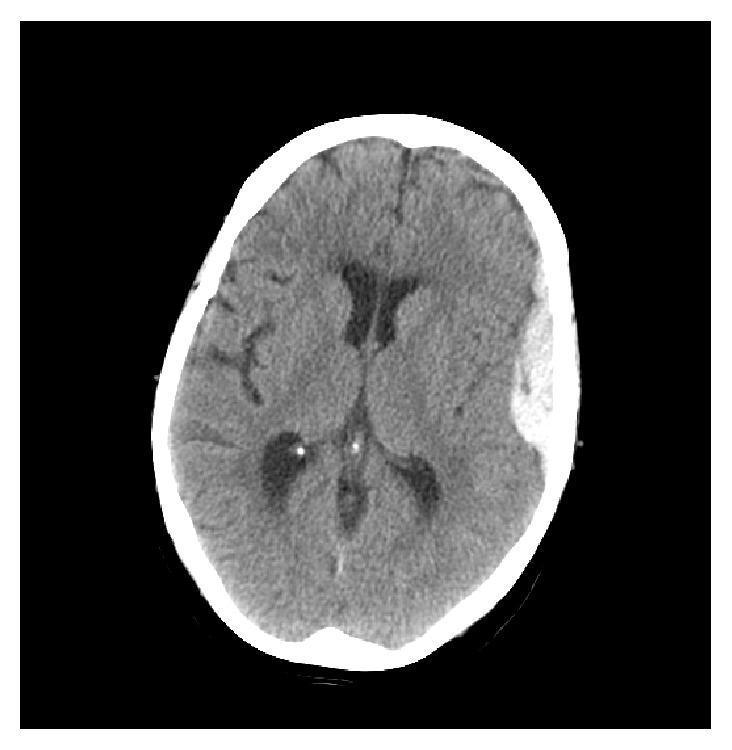
3e. Cerebral Contusion & Intracerebral Hemorrhage
- Bruising/hemorrhage within the brain parenchyma
- Commonly at frontal/temporal poles (coup–contrecoup)
CT scans showing the classic appearances:
4. Neurological Assessment — Nursing Priorities
ABCs First
Airway, breathing, circulation must be secured before any neurological assessment. The pediatric and adult brain are highly sensitive to hypoxia and hypoperfusion.
Pupil Examination (assess simultaneously with GCS)
| Finding | Significance |
|---|---|
| Unilateral fixed & dilated | Ipsilateral uncal herniation (CN III compression) |
| Bilateral fixed & dilated | Global anoxia / brainstem failure — poor prognosis |
| Anisocoria > 1 mm (new) | Rising ICP — requires urgent reimaging |
| Unreactive pupils with normal GCS | Still significant; report to team |
Cushing's Triad — Sign of Impending Herniation
- Hypertension (widened pulse pressure)
- Bradycardia
- Irregular breathing
This is a late, pre-terminal sign. Act immediately.
Signs of Raised ICP in Children
- Bulging fontanelle (infants)
- Vomiting, irritability, altered consciousness
- Papilledema (late)
- Cushing's triad
Herniation Syndromes
- Transtentorial (uncal): ipsilateral dilated pupil, contralateral hemiplegia, decreasing consciousness
- Central: bilateral pupil changes, decorticate → decerebrate posturing
5. Secondary Brain Injury — What Nurses Must Prevent
Secondary brain injury is caused by systemic insults that compound primary damage. The key ones:
| Insult | Target | Nursing Action |
|---|---|---|
| Hypotension (SBP < 90 mmHg) | SBP ≥ 90 mmHg | Fluid resuscitation, vasopressors as ordered; monitor MAP |
| Hypoxia (SpO₂ < 90%) | PaO₂ > 60 mmHg; SpO₂ ≥ 95% | Supplemental O₂, airway management |
| Hyperthermia | Normothermia | Antipyretics, cooling blankets |
| Hyperglycemia/Hypoglycemia | Euglycemia | Monitor glucose; treat per protocol |
| Seizures | Seizure prevention/control | Administer antiepileptics as ordered; monitor EEG |
Hypotension (SBP < 90 mmHg) is an independent predictor of poor outcome in TBI. — Rosen's Emergency Medicine
6. ICP Monitoring & Management
When ICP Monitoring is Indicated
- GCS ≤ 8 with structural injury on CT
- High-risk patients (large contusions, coagulopathy)
- Moderate TBI undergoing urgent non-neurosurgical surgery
Targets
- ICP < 20–22 mmHg
- CPP (= MAP − ICP) = 60–70 mmHg
Tiered ICP Management (Sabiston / ACS-TQIP)
Tier 1:
- Head of bed 30°, head in neutral position (ensure cervical immobilisation devices don't compress jugular veins)
- Short-acting sedation (propofol, fentanyl) to allow periodic neurological checks
- CSF drainage via EVD/ventriculostomy when available
Tier 2:
- Hyperosmolar therapy: mannitol or hypertonic saline
- Monitor serum Na every 6 h (hold if Na > 160 mEq/L or osmolality > 320 mOsm/L)
- Consider controlled hyperventilation to PaCO₂ 30–35 mmHg (temporary; monitor for cerebral ischaemia)
- Neuromuscular blockade trial dose
Tier 3:
- Decompressive craniectomy
- Continuous NMB infusion
- Barbiturate coma (with continuous EEG to titration burst suppression)
— Sabiston Textbook of Surgery, pp. 805–806
7. Nursing Management of the Head-Injured Patient
Emergency Phase (ED/Trauma Bay)
- Immobilise cervical spine until cleared (assume C-spine injury with significant head trauma)
- Airway: intubate if GCS ≤ 8, airway unprotected, or rising ICP signs
- Breathing: ventilate to ETCO₂ 35–45 mmHg; avoid hyperventilation unless herniation is imminent
- Circulation: aggressive fluid resuscitation to maintain SBP ≥ 90 mmHg
- Disability: GCS + pupils; identify lateralising signs
- Exposure: full assessment for other injuries; remove clothing carefully
Ongoing Neurological Monitoring (ICU/Ward)
- GCS every 1 hour (or more frequently if deteriorating)
- Pupils size, symmetry, reactivity hourly
- Vital signs including BP, HR, RR, temperature
- ICP values and CPP calculations if monitored
- Limb movement/power comparison (drift, pronator)
- Seizure activity — document duration, type, post-ictal state
- Fluid balance — strict hourly urine output; target euvolemia
Positioning
- HOB 30° (unless haemodynamically unstable)
- Head midline — avoid neck flexion/rotation (obstructs venous drainage)
Anticoagulation Reversal
- Warfarin → prothrombin complex concentrate (PCC); check INR
- Clopidogrel → desmopressin (DDAVP)
- Low threshold for CT in any anticoagulated patient with head injury, even if asymptomatic
8. Special Populations
Elderly
- Higher risk of subdural and intraparenchymal haemorrhage (brain atrophy stretches bridging veins)
- Less likely to develop EDH (dura more adherent to skull)
- Brain atrophy creates extra intracranial space → bleeding may accumulate before symptoms appear → delayed diagnosis
- Any mental status change: do not attribute to baseline dementia; CT first
- Anticoagulant use is common — immediate CT even with minor mechanism
Children
- Larger head-to-body ratio → higher torque forces on cervical spine
- Less myelinated brain → higher risk of DAI and post-traumatic seizures
- Pliable skull → parenchymal injury without skull fracture
- CPP target > 40 mmHg; ICP target < 20 mmHg
- Consider non-accidental injury (NAI) in any infant/toddler with unexplained TBI, especially with retinal haemorrhages or patterned bruising
9. Red Flag Signs — Escalate Immediately
| Sign | Concern |
|---|---|
| Falling GCS (≥ 2 points) | Deterioration / expanding haematoma |
| New pupil asymmetry or fixed/dilated pupil | Transtentorial herniation |
| Cushing's triad | Imminent herniation |
| New seizure | Intracranial pathology, hypoglycaemia |
| CSF from nose (rhinorrhoea) or ears (otorrhoea) | Basal skull fracture |
| Raccoon eyes / Battle's sign | Basal skull fracture |
| Worsening headache | Rising ICP |
| Persistent vomiting | Raised ICP |
10. Discharge Advice (Mild/Concussion)
- Return to ED if: worsening headache, repeated vomiting, increasing confusion, seizure, one-sided weakness, or slurred speech
- No alcohol for 48 hours
- Rest 24–48 h, then graduated return to activity (not prolonged bed rest)
- No driving until cleared by clinician
- Family/carer should observe overnight — wake patient every 2–4 h on night of injury
Sources:
- Rosen's Emergency Medicine, Head Injury chapter
- Sabiston Textbook of Surgery (10e), TBI chapter — GCS table, ICP tiers
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma — Epidural Hematoma section
- Tintinalli's Emergency Medicine — Elderly & Pediatric Head Injury
This is a shared conversation. Sign in to Orris to start your own chat.