explain me 10 common heart diseases with ecg changes and ecg images of those diseases
Reading File
Finding Sources
Searching the Web
common heart diseases ECG changes electrocardiogram findings with images
Finding Sources
Finding Sources
Searching the Web
ECG images myocardial infarction atrial fibrillation heart block LVH site:litfl.com OR site:ecgwaves.com
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Searching the Web
ECG images pericarditis STEMI ventricular tachycardia heart block Brugada WPW ecgwaves litfl
Loading Image
Loading Image
Loading Image
Searching the Web
STEMI inferior ECG image litfl.com OR ecgwaves.com Q wave ST elevation
Loading Image
Loading Image
I now have all the material needed to write a thorough, well-illustrated answer. Here is the complete guide:
10 Common Heart Diseases: ECG Changes & Images
1. ST-Elevation Myocardial Infarction (STEMI)
What it is: Complete occlusion of a coronary artery causing transmural myocardial necrosis.
ECG Changes:
- Hyperacute phase: Tall, peaked ("hyperacute") T waves - the earliest sign
- Acute phase: ST elevation ≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in precordial leads, with a convex (tombstone) or straight appearance
- Evolving: Development of pathological Q waves (>40 ms wide, >25% of R wave height) - indicate irreversible necrosis
- Reciprocal ST depression in opposite leads (e.g., inferior STEMI in II, III, aVF causes reciprocal depression in I, aVL)
- Late: T-wave inversion, persistent Q waves
Localisation:
| Territory | Leads with ST elevation |
|---|---|
| Inferior | II, III, aVF |
| Anterior | V1-V4 |
| Lateral | I, aVL, V5-V6 |
| Posterior | R>S in V1-V2, ST depression V1-V3 |
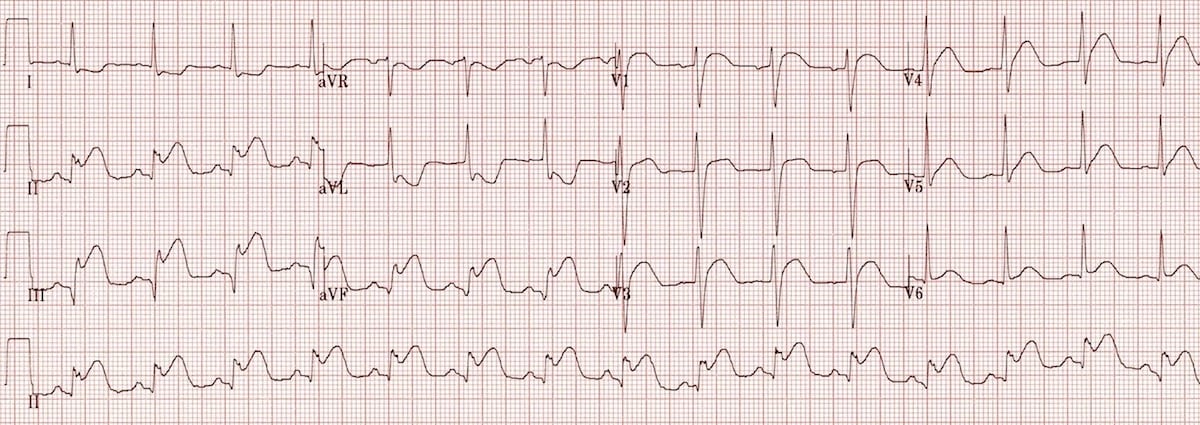
ECG - Inferior STEMI (note ST elevation in II, III, aVF with pathological Q waves and reciprocal change in aVL):
2. Atrial Fibrillation (AF)
What it is: Chaotic, disorganised atrial electrical activity with multiple simultaneous re-entrant wavelets, causing irregular ventricular response. Associated with hypertension, valvular disease, heart failure, thyrotoxicosis, and alcohol ("holiday heart").
ECG Changes (from Tintinalli's Emergency Medicine):
- Absent P waves - replaced by a chaotic, irregular fibrillatory baseline (best seen in V1)
- Irregularly irregular ventricular rhythm - the hallmark finding
- Atrial rate >600 bpm (not visible as distinct waves)
- Ventricular rate typically 120-170 bpm when AV node is unaffected
- Narrow QRS complexes (unless aberrant conduction or bundle branch block)
ECG - Three examples of Atrial Fibrillation (A: rapid ventricular response, B: controlled rate, C: slow response):
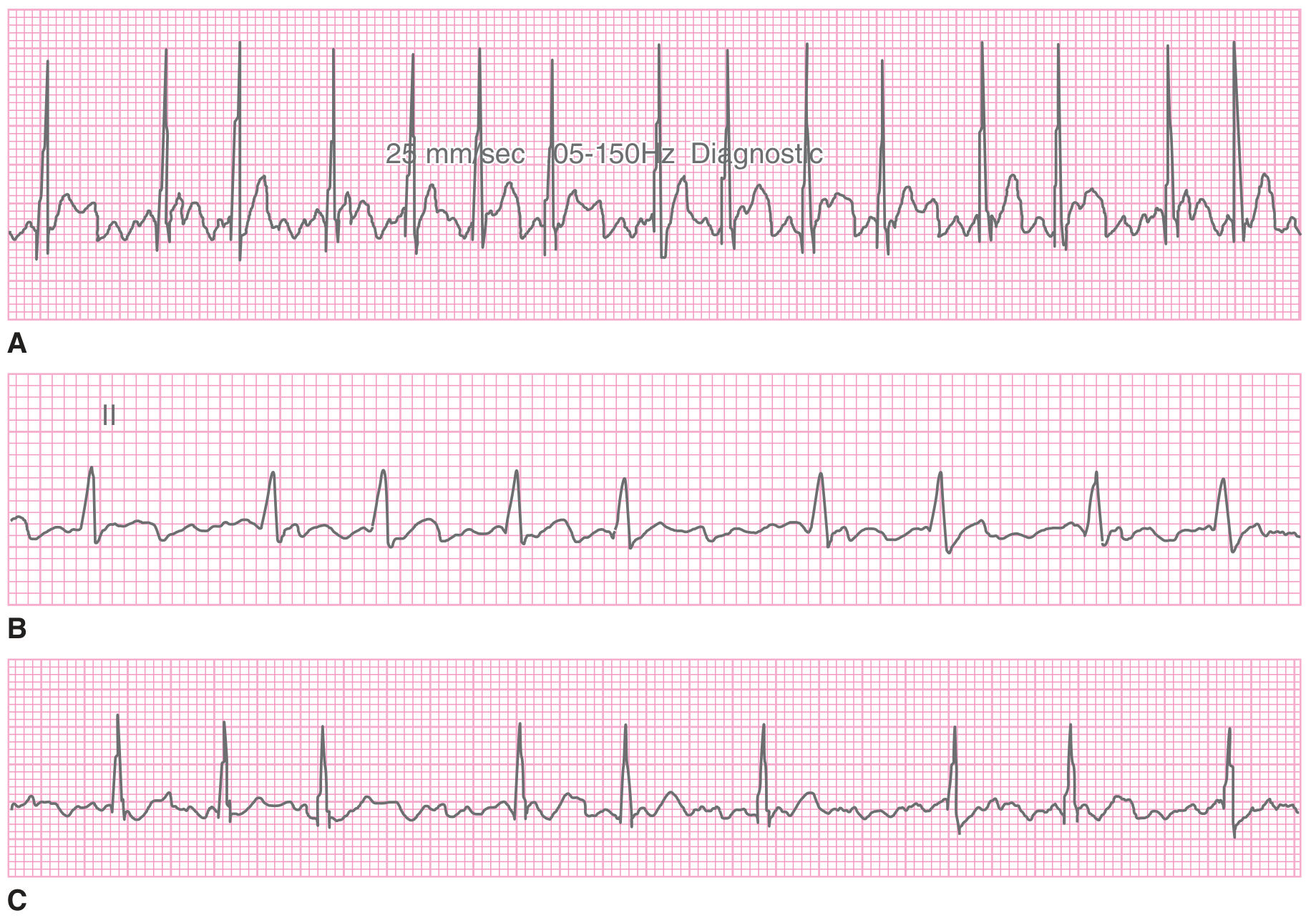
Source: Tintinalli's Emergency Medicine
3. Complete (Third-Degree) AV Heart Block
What it is: Complete failure of conduction between the atria and ventricles. The atria and ventricles beat independently, with the ventricles under control of a slow junctional or ventricular escape pacemaker.
ECG Changes (from Goldman-Cecil Medicine and Harrison's Principles):
- P waves and QRS complexes are completely dissociated - P waves "march through" at their own rate with no relationship to QRS
- Atrial rate is faster than ventricular rate (key distinguishing feature)
- Ventricular rate typically 20-40 bpm (ventricular escape) or 40-60 bpm (junctional escape)
- QRS may be narrow (junctional escape) or wide/bizarre (ventricular escape)
- Causes: acute inferior MI, infiltrative disease (sarcoidosis, amyloid), Lyme disease, drugs (digoxin, beta-blockers)
ECG - Idioventricular escape rhythm (slow, wide complex beats at ~30 bpm - seen in complete heart block with ventricular escape):
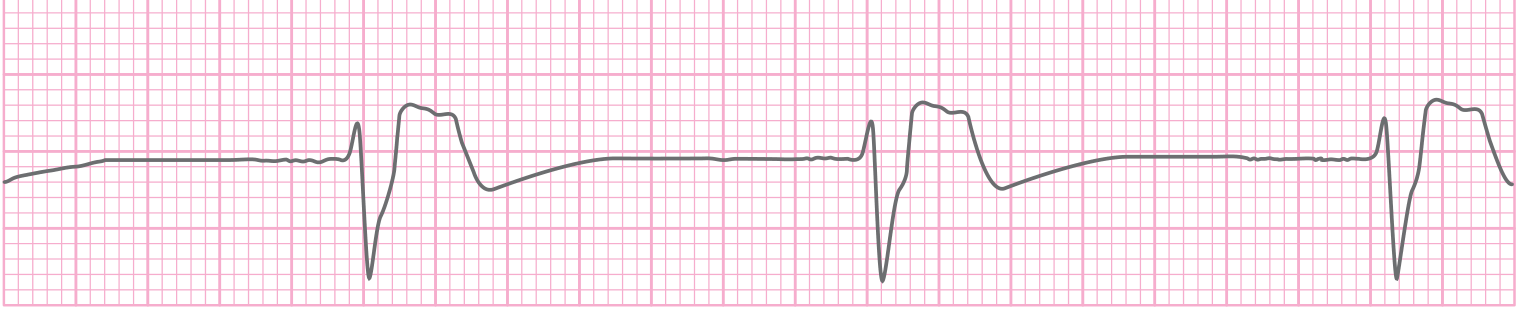
Source: Tintinalli's Emergency Medicine
4. Left Ventricular Hypertrophy (LVH)
What it is: Thickening of the left ventricular wall, commonly due to hypertension, aortic stenosis, or hypertrophic cardiomyopathy.
ECG Changes:
- Increased QRS voltage (Sokolow-Lyon criterion: S in V1 + R in V5 or V6 ≥35 mm; or R in aVL ≥11 mm)
- Left axis deviation
- Strain pattern: ST depression and T-wave inversion in I, aVL, V5-V6 (lateral leads)
- Left atrial enlargement (P mitrale): Biphasic P wave in V1, prolonged P wave duration >120 ms in II
- Widened QRS (but usually <120 ms unless combined with LBBB)
As noted in Braunwald's Heart Disease: LV hypertrophy and left atrial enlargement on ECG may indicate left heart disease rather than pulmonary arterial hypertension as the cause of elevated pressures.
5. Pericarditis
What it is: Inflammation of the pericardial sac, most often viral in origin. Produces characteristic pleuritic chest pain and serial ECG changes that evolve through four stages.
ECG Changes (4 classical stages):
| Stage | Timing | ECG Findings |
|---|---|---|
| I | Hours-days | Diffuse concave ("saddle-shaped") ST elevation in multiple leads (I, II, aVL, aVF, V2-V6); PR depression (virtually all leads except aVR which shows PR elevation) |
| II | Days | ST returns to baseline; PR depression persists |
| III | Weeks | Diffuse T-wave inversion |
| IV | Weeks-months | ECG returns to normal |
Key distinguishing features from STEMI:
- ST elevation is diffuse (not territory-based) and concave up (not convex)
- PR depression is a hallmark not seen in MI
- No reciprocal changes (except aVR)
- No pathological Q waves
ECG - Pericarditis (note concave ST elevation in multiple leads with PR depression; compare with benign early repolarisation):

Source: LITFL ECG Library
6. Ventricular Tachycardia (VT)
What it is: A potentially life-threatening arrhythmia originating below the bundle of His, most commonly in the setting of ischaemic heart disease, dilated cardiomyopathy, or electrolyte imbalance.
ECG Changes (from Goldman-Cecil Medicine):
- Wide QRS complex tachycardia - QRS duration >120 ms (often >140 ms) at rate >100 bpm
- AV dissociation - P waves march independently of QRS complexes (pathognomonic of VT when visible)
- Fusion beats - P wave partially captures the ventricle, producing a QRS morphology intermediate between sinus and VT beats (pathognomonic)
- Capture beats - occasional narrow QRS when a P wave fully conducts through to the ventricle
- Concordance - all precordial leads pointing in the same direction (positive or negative)
- Northwest axis (extreme left axis deviation)
The combination of fusion beats or AV dissociation during a wide-QRS complex tachycardia confirms VT and distinguishes it from SVT with aberrancy (Goldman-Cecil Medicine).
7. Wolff-Parkinson-White (WPW) Syndrome
What it is: An accessory pathway (Bundle of Kent) bypasses the AV node, causing ventricular pre-excitation and risk of re-entrant tachycardia. Can be life-threatening if AF develops with rapid conduction down the accessory pathway.
ECG Changes:
- Short PR interval (<120 ms) - because conduction bypasses AV nodal delay
- Delta wave - slurred upstroke at the beginning of the QRS complex (initial pre-excitation)
- Wide QRS (>120 ms) - due to fusion of pre-excited and normally conducted impulses
- Secondary ST-T changes opposite to the delta wave direction
- In AF with WPW: extremely rapid, irregular wide complex tachycardia (>250 bpm) - a medical emergency
The LITFL Killer ECG infographic below illustrates the delta wave and short PR interval characteristic of WPW:
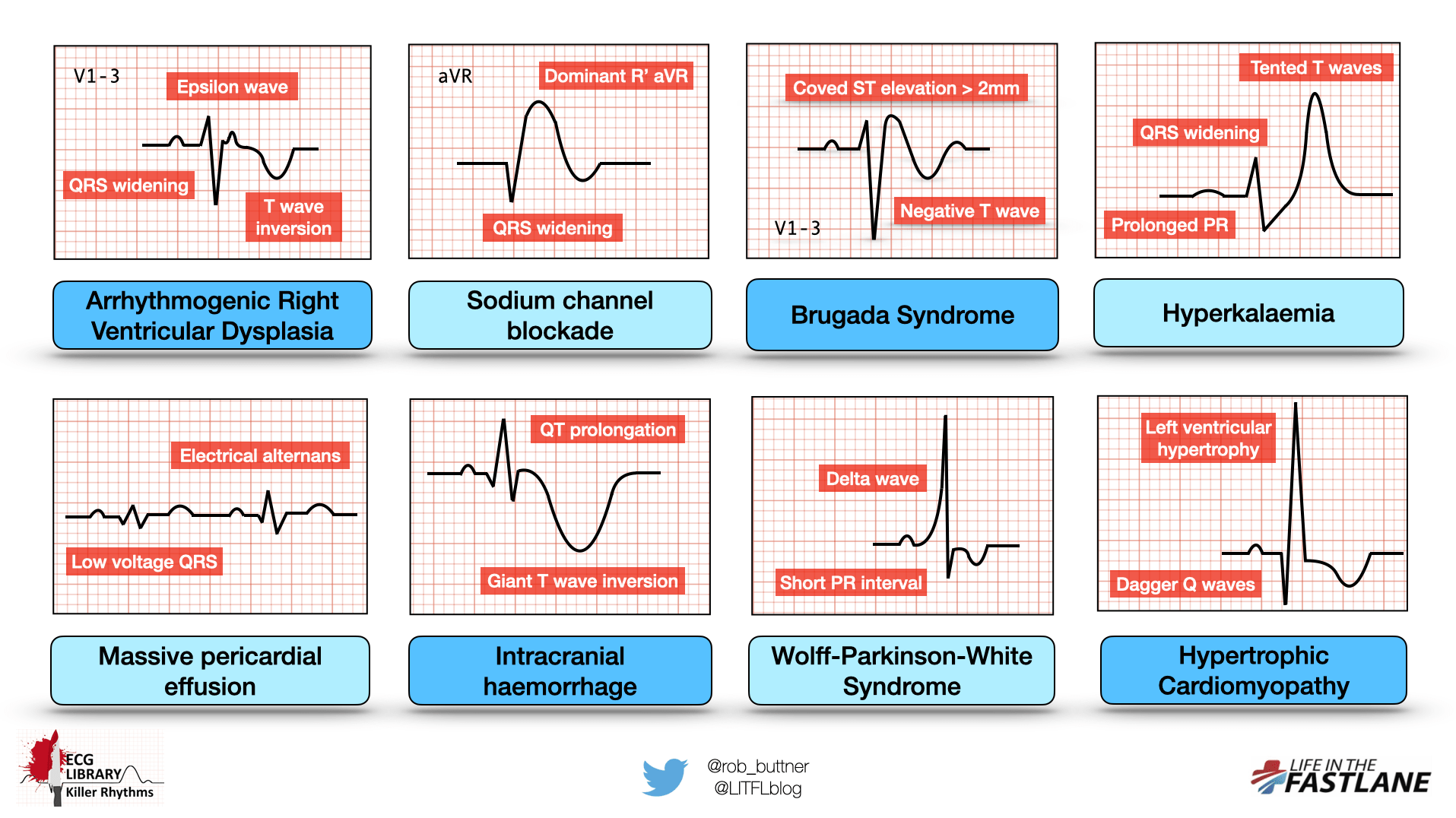
Source: LITFL ECG Library - Killer ECG Patterns
8. Brugada Syndrome
What it is: An inherited sodium channelopathy causing sudden cardiac death from ventricular fibrillation in structurally normal hearts. More common in Asian males.
ECG Changes (Type 1 - diagnostic):
- Coved-type ST elevation ≥2 mm in right precordial leads V1-V3
- Negative T wave (inverted) in V1-V3 following the coved ST elevation
- The pattern resembles a "shark fin" or right bundle branch block morphology
- Type 2 and 3 have saddle-shaped ST elevation and are not diagnostic without clinical criteria
- The Type 1 pattern can be dynamic - triggered or unmasked by fever, sodium channel blockers, or vagal tone
ECG pattern - see the Brugada entry in the LITFL infographic above (top right): coved ST elevation >2 mm in V1-3 with negative T wave.
9. Hypertrophic Cardiomyopathy (HCM)
What it is: Genetic sarcomere mutation causing asymmetric septal hypertrophy, dynamic LV outflow tract obstruction, and high risk of sudden cardiac death, especially in young athletes.
ECG Changes:
- Voltage criteria for LVH (deep S in V1-V2, tall R in V5-V6)
- "Dagger" Q waves - deep, narrow Q waves in lateral (I, aVL, V5-V6) and/or inferior leads - due to septal hypertrophy (not ischaemia)
- Left axis deviation
- T-wave inversion - widespread, often dramatic in lateral leads
- Left atrial enlargement - broad, bifid P wave
- Giant T-wave inversion (particularly deep in V3-V5) - a hallmark in the apical variant (Yamaguchi syndrome)
- Atrial fibrillation in 20-25% of patients
ECG pattern - see the HCM entry in the LITFL infographic above (bottom right): LVH voltage + dagger Q waves.
10. Pulmonary Embolism (PE) / Right Heart Strain
What it is: Acute obstruction of pulmonary circulation causing acute pressure overload on the right ventricle, producing characteristic but variable ECG changes.
ECG Changes:
- Sinus tachycardia - the most common and sensitive finding (in >40% of cases)
- S1Q3T3 pattern - S wave in Lead I, Q wave in Lead III, T-wave inversion in Lead III (present in ~20%, not specific)
- Right bundle branch block (RBBB) or incomplete RBBB
- T-wave inversion in V1-V4 - right ventricular strain pattern
- Right axis deviation
- P pulmonale - tall, peaked P waves in inferior leads (>2.5 mm) indicating right atrial overload
- As noted in Braunwald's Heart Disease: RV strain pattern (RV hypertrophy with ST depression in V1-V3) may be evident in advanced disease
ECG - Athlete's heart 12-lead ECG from Goldman-Cecil Medicine (illustrating normal variant voltage changes, early repolarisation, and variable P wave morphology at bradycardia - for context of normal vs pathological voltage):
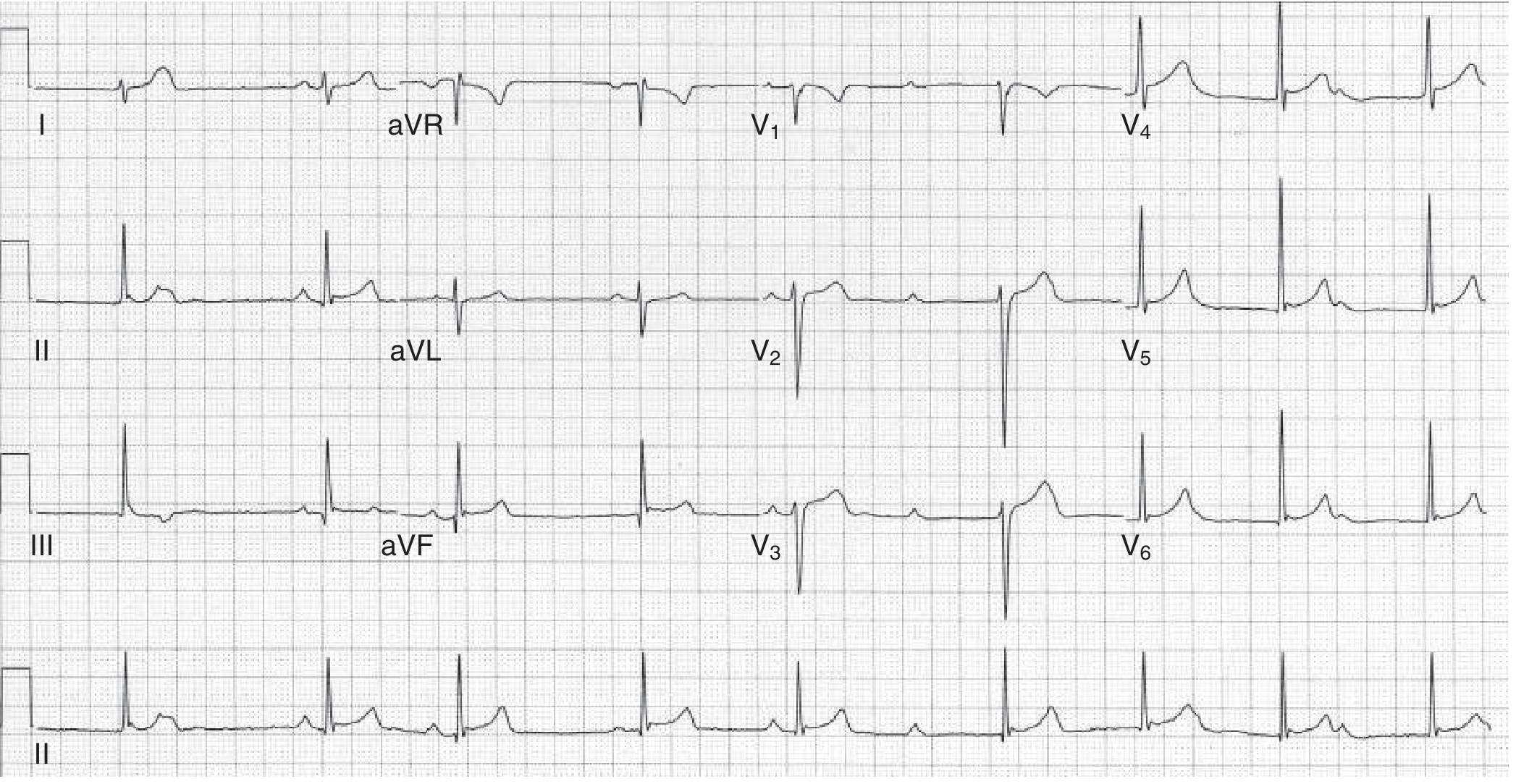
Source: Goldman-Cecil Medicine - Figure 42-7 Athlete's Heart
Quick Reference Summary Table
| Disease | Key ECG Finding | Leads Affected |
|---|---|---|
| STEMI | Convex ST elevation, Q waves, hyperacute T | Territory-specific |
| Atrial Fibrillation | Absent P waves, irregularly irregular RR | All leads |
| Complete Heart Block | P-QRS dissociation, slow escape rhythm | All leads |
| LVH | High voltage, strain pattern, left axis | V1/V5-V6, I, aVL |
| Pericarditis | Diffuse concave ST elevation, PR depression | Diffuse (not V1, aVR) |
| Ventricular Tachycardia | Wide QRS tachycardia, AV dissociation | All leads |
| WPW | Short PR, delta wave, wide QRS | All leads |
| Brugada | Coved ST elevation, negative T wave | V1-V3 |
| HCM | Dagger Q waves, massive LVH voltage | Lateral/inferior |
| Pulmonary Embolism | Sinus tachycardia, S1Q3T3, RBBB, RV strain | I, III, V1-V4 |
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide - ECG sections on arrhythmias
- Goldman-Cecil Medicine (International Edition) - ECG interpretation chapters
- Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine - Pulmonary hypertension and arrhythmia chapters
- Harrison's Principles of Internal Medicine 22E - Atrial fibrillation chapter
- LITFL ECG Library - Inferior STEMI, Pericarditis, Killer ECG patterns
This is a shared conversation. Sign in to Orris to start your own chat.