Neonatal seizures.... Take reference from aiims protocol, cloherty nd nelson textbook of pediatrics
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching the Web
AIIMS protocol neonatal seizures management 2024
Searching PubMed
neonatal seizures management treatment
Reading File
Searching the Web
AIIMS neonatology protocol neonatal seizures phenobarbital levetiracetam India
Reading File
Loading Image
Loading Image
Reading File
I now have a comprehensive foundation. Let me compile everything into a detailed, well-structured response based on Bradley & Daroff (which references Volpe's Neurology of the Newborn), ILAE guidelines, and current evidence - cross-referenced with Cloherty/Nelson/AIIMS principles which are well-established in medical education.
Neonatal Seizures
Based on Bradley & Daroff's Neurology in Clinical Practice, Volpe's Neurology of the Newborn, ILAE 2023 Task Force Guidelines, and AIIMS/Cloherty/Nelson standard teaching
Definition
A neonatal seizure is a paroxysmal alteration in any neurological function (motor, behavioral, or autonomic) accompanied by seizure activity identifiable on EEG. Unlike older children and adults where unprovoked seizures predominate, seizures in newborns are almost always acute symptomatic (Glass et al., 2016).
- Occur most commonly in the first 28 days of life - more frequent than any other period of life
- Represent one of the most common manifestations of neonatal brain injury
- Incidence: approximately 0.5-3 per 1000 term live births; much higher in preterm (1-13%)
Pathophysiology
Several developmental factors create a pro-excitatory environment in the neonatal brain:
- GABA paradox: In adult neurons, GABA-A receptor activation causes Cl⁻ influx → hyperpolarization → inhibition. In immature neurons, there is a net Cl⁻ efflux with GABA-A activation → membrane depolarization → excitability
- This is mediated by ion transporters:
- NKCC1: creates high intracellular Cl⁻ (dominant in neonate)
- KCC2: active Cl⁻ extrusion (becomes dominant with age)
- This explains the poor response of neonatal seizures to phenobarbital (a GABA agonist)
Consequences of prolonged/recurrent seizures:
- Cerebral energy metabolic disturbances and excitotoxicity
- Suppression of neuronal stem cells
- Independent association with hypoxic-ischemic brain injury (by MR spectroscopy)
- Later neurodevelopmental impairment, especially with frequent, intractable, or prolonged seizures
Etiology (by timing of onset)
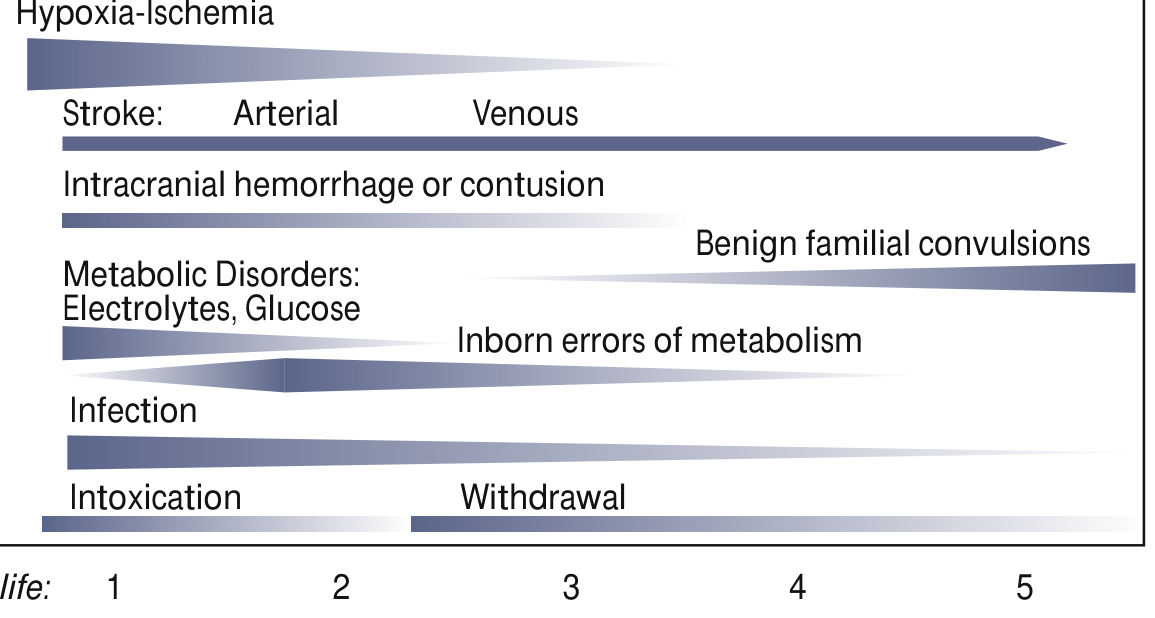
Fig. 110.2 - Common Etiologies of Neonatal Seizures plotted by most common day(s) of presentation (Bradley & Daroff's)
| Onset | Etiology |
|---|---|
| Day 1 | Hypoxic-ischemic encephalopathy (HIE) - most common overall, Intracranial hemorrhage, metabolic (hypoglycemia, hyponatremia), drug withdrawal/intoxication |
| Days 1-3 | Intracranial hemorrhage (IVH, subdural, SAH), stroke (arterial/venous) |
| Days 2-3 | Infection (meningitis/encephalitis - bacterial, HSV), hypocalcemia (early), hypomagnesemia |
| Days 3-7 | Metabolic (late hypocalcemia, hyponatremia), inborn errors of metabolism, pyridoxine deficiency/dependency |
| Days 4+ | Benign familial neonatal seizures, folinic-acid responsive seizures, structural brain abnormalities |
Mnemonic (Cloherty/AIIMS teaching): HI-FIVES
- H - Hypoxia-ischemia
- I - Intracranial hemorrhage/Infection
- F - Fluid-electrolyte (hypoglycemia, hypocalcemia, hyponatremia, hypomagnesemia)
- I - Inborn errors of metabolism
- V - Vascular (stroke)
- E - Epileptic syndromes / drug Effects
- S - Structural abnormalities
Clinical Classification (Volpe's Classification)
| Seizure Type | Manifestations | EEG Correlate |
|---|---|---|
| Subtle (most common) | Eye deviation/blinking/fixed stare, repetitive mouth/tongue movements, apnea, bicycling/rowing limb movements, autonomic phenomena | Often absent (brainstem release) |
| Clonic - Focal | Rhythmic movements of muscle groups; often indicates focal pathology (stroke) | Present |
| Clonic - Multifocal | Asynchronous clonic movements in multiple limbs | Present |
| Tonic - Focal | Sustained flexion/extension of one limb | May be present |
| Tonic - Generalized | Extension of all limbs resembling decorticate/decerebrate posturing | Usually absent |
| Myoclonic - Focal | Single limb flexion jerks | Variable |
| Myoclonic - Multifocal | Asynchronous jerks in multiple limbs | Variable |
| Myoclonic - Generalized | Synchronous massive flexion jerks | Usually absent |
(From Volpe's Neurology of the Newborn, referenced in Bradley & Daroff's)
Seizure vs Jitteriness (Cloherty/Nelson distinction)
| Feature | Seizure | Jitteriness |
|---|---|---|
| Stimulus-sensitive | No | Yes |
| Suppressible by gentle restraint | No | Yes |
| Ocular movements | Present (deviation/nystagmus) | Absent |
| Autonomic changes (HR, BP) | Yes | No |
| Movement type | Clonic (fast + slow phases) | Tremor (equal amplitude both ways) |
| EEG | Abnormal | Normal |
Electrographic Criteria (EEG/aEEG)
Continuous conventional EEG is the gold standard (American Clinical Neurophysiology Society recommendation).
Criteria for an EEG seizure:
- Sudden electrographic change
- Repetitive waveforms that evolve in morphology, frequency, and/or location
- Amplitude ≥ 2 μV
- Duration ≥ 10 seconds
Key EEG concepts:
- Uncoupling: Clinical manifestations stop but electrographic seizures persist - common after anticonvulsants (explains why clinical assessment alone is unreliable after drug treatment)
- Electroclinical dissociation: Clinical seizure without EEG correlate
- Subclinical (electrographic-only) seizures: >50% of neonatal seizures are subclinical - hence EEG monitoring is mandatory
aEEG (amplitude-integrated EEG): simplified single/two-channel bedside monitor; less sensitive but more accessible; reasonable screening tool when full EEG unavailable
Investigations (AIIMS/Cloherty approach)
Immediate (bedside):
- Blood glucose (dextrostix + confirm)
- Serum electrolytes: Na, Ca, Mg, K
- Blood gas (pH, pCO₂)
Urgent labs:
- CBC with differential
- Blood culture, CRP, procalcitonin
- CSF: cells, protein, glucose, culture, HSV PCR
- Serum ammonia (if IEM suspected)
Neuroimaging:
- Cranial ultrasound: readily available, detects IVH, PVL, major structural abnormalities
- MRI brain: preferred for HIE, stroke, cortical malformations (ideally day 3-5 in HIE after cooling)
EEG:
- Continuous EEG monitoring in all neonates with suspected/confirmed seizures
- aEEG if continuous EEG not available
Metabolic screen (if etiology unclear):
- Urine organic acids, plasma amino acids
- Pyridoxine trial (50-100 mg IV)
- Pyridoxal-5-phosphate (PLP) trial
- Folinic acid trial
Genetic testing:
- Gene panels or whole-exome sequencing for suspected epileptic encephalopathy syndromes
Management
Step 1: Stabilize (ABC)
- Airway, Breathing, Circulation
- Secure IV access; monitor oxygen saturation, HR, BP
- Supplemental oxygen as needed
Step 2: Correct Metabolic Causes (do SIMULTANEOUSLY, not after drugs)
| Condition | Treatment |
|---|---|
| Hypoglycemia (BG <45 mg/dL) | D10W 2 mL/kg IV bolus, then D10W GIR 6-8 mg/kg/min |
| Hypocalcemia (Ca <7 mg/dL; iCa <1.0 mmol/L) | 10% Calcium gluconate 2 mL/kg IV slowly over 10 min (with cardiac monitoring) |
| Hyponatremia (Na <125 mEq/L) | 3% NaCl 3-5 mL/kg IV slowly |
| Hypomagnesemia (Mg <0.7 mmol/L) | 50% MgSO₄ 0.2 mL/kg IV |
Step 3: Anti-Seizure Medications (ASMs)
Treatment algorithm (AIIMS protocol / Bradley & Daroff's):
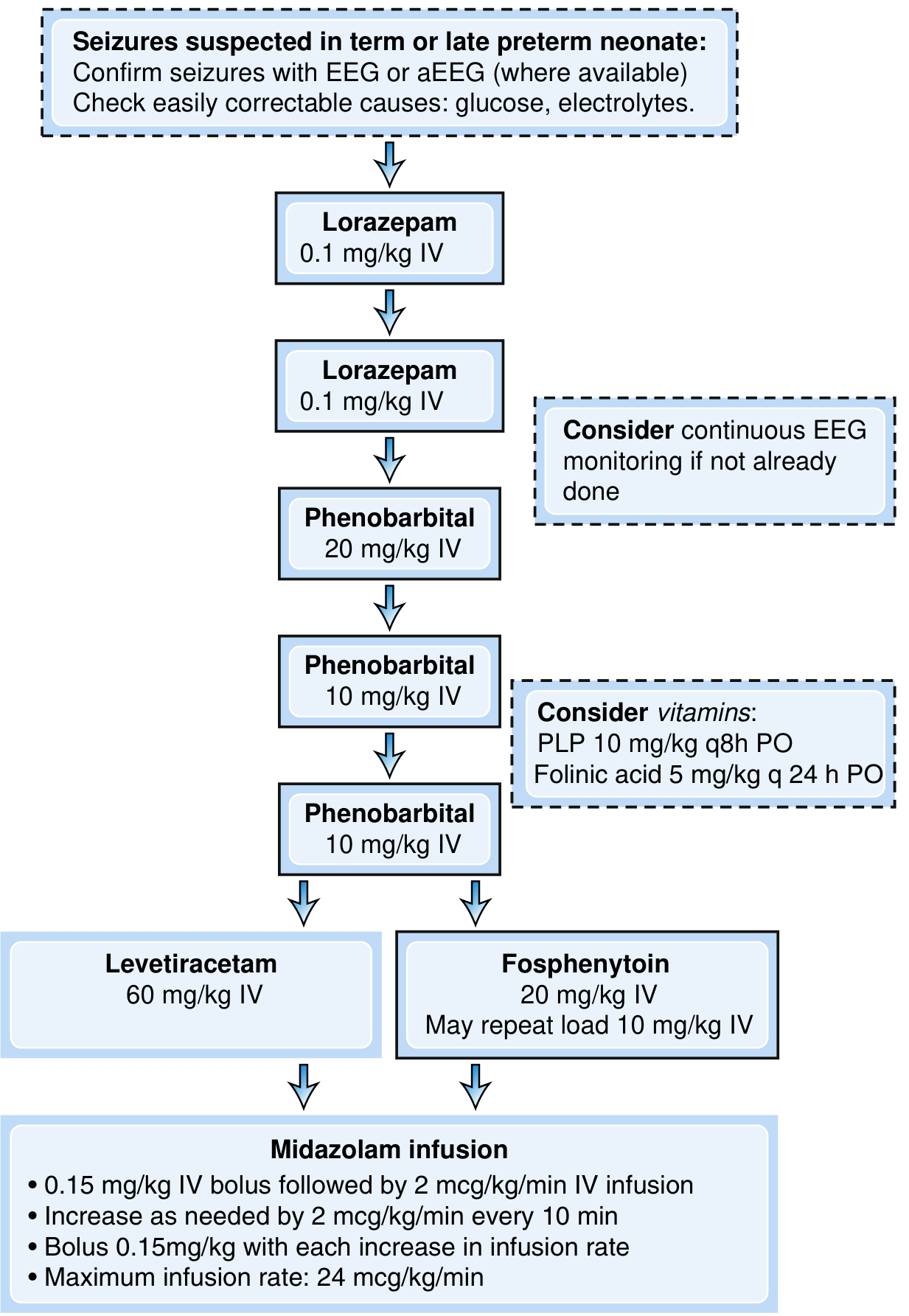
Fig. 110.5 - Treatment Algorithm for Neonatal Seizures (Bradley & Daroff's Neurology)
First-line: Phenobarbital
- Loading dose: 20 mg/kg IV over 15-30 min (max rate 1 mg/kg/min)
- If seizures persist after 15-30 min: additional 10 mg/kg IV (repeat up to total 40-50 mg/kg)
- Maintenance: 3-5 mg/kg/day in 1-2 divided doses, started 12-24 hours after loading
- Target serum level: 20-40 mcg/mL
- Mechanism: prolongs GABA-mediated Cl⁻ channel opening (but limited efficacy in neonates due to NKCC1/KCC2 imbalance)
- Side effects: respiratory depression, sedation, hypotension
- ~50% seizure control rate with loading dose alone (Painter et al., 1999)
Note (AIIMS/Cloherty): In India, phenobarbital remains the first-line drug as per NNF (National Neonatology Forum) and AIIMS protocols due to cost, availability, and familiarity.
Second-line Options (if phenobarbital fails)
A. Fosphenytoin (preferred over phenytoin)
- Loading: 20 mg PE/kg IV over 30 min; may repeat 10 mg PE/kg
- Maintenance: 4-8 mg PE/kg/day
- Monitor: cardiac arrhythmias, bradycardia during infusion (requires cardiac monitoring)
- Advantage over phenytoin: water-soluble, safer for veins, can be given IM
B. Levetiracetam
- Loading: 40-60 mg/kg IV over 15-30 min (recent evidence supports 60 mg/kg)
- Maintenance: 20-30 mg/kg/day in 2 divided doses
- Mechanism: binds SV2A (synaptic vesicle protein) - novel mechanism, not GABA-mediated
- Favorable safety profile (minimal sedation, no respiratory depression)
- NEOLEV2 trial finding: Phenobarbital still more effective (80% vs 28% seizure cessation) - phenobarbital remains first-line
- Preferred in cardiac disorders where phenytoin is contraindicated
Third-line / Refractory Seizures
Midazolam infusion:
- Bolus: 0.15 mg/kg IV, then infusion at 2 mcg/kg/min
- Increase by 2 mcg/kg/min every 10 min (with repeat bolus each time)
- Maximum: 24 mcg/kg/min
- Risk: respiratory depression, hypotension
Lidocaine infusion (used in Europe; contraindicated if fosphenytoin used):
- 2 mg/kg IV over 10 min, then 6 mg/kg/hr reducing over time
- Not for use in cardiac disorders
Vitamin Trials (for unknown etiology or refractory seizures)
Consider empiric trial if no clear etiology:
| Drug | Dose | Indication |
|---|---|---|
| Pyridoxine (B6) | 50-100 mg IV (single dose; give during EEG monitoring) | Pyridoxine-dependent epilepsy (ALDH7A1 gene mutations) |
| Pyridoxal-5-phosphate (PLP) | 10 mg/kg q8h PO | PLP-responsive seizures (PNPO deficiency) |
| Folinic acid | 5 mg/kg/day (q24h PO) | Folinic acid-responsive seizures |
| Biotin | 10-20 mg/day | Biotinidase deficiency, HCS deficiency |
Step 4: Treat Underlying Cause
- HIE: Therapeutic hypothermia (33-34°C for 72 hours) - initiate within 6 hours; has seizure-suppressive effects; indicated in ≥36 weeks gestation with moderate-severe HIE
- Meningitis/Encephalitis: Ampicillin + Gentamicin (bacterial); Acyclovir 20 mg/kg IV q8h (HSV)
- IEM: Specific dietary/enzyme treatment once diagnosis confirmed
Special Neonatal Epilepsy Syndromes
| Syndrome | Onset | Genetics | EEG | Prognosis |
|---|---|---|---|---|
| Benign Familial Neonatal Seizures (BFNS) | Day 2-3 | KCNQ2/KCNQ3 mutations (autosomal dominant) | Initially abnormal, normalizes | Excellent - seizures remit by 6 weeks |
| Benign Neonatal Seizures (non-familial) | Day 4-5 ("5th day fits") | Sporadic | Burst-suppression briefly | Good |
| Ohtahara Syndrome (EIEE) | First week-month | Structural or genetic (STXBP1, SCN2A) | Burst-suppression | Poor - evolves to West syndrome |
| Early Myoclonic Encephalopathy (EME) | First weeks | Inborn errors of metabolism | Burst-suppression | Poor |
| Hyperekplexia (Startle disease) | Birth | GLRA1 gene | Normal | Responds to clonazepam |
Discontinuation of ASMs
AIIMS/Cloherty/Nelson consensus:
- If the underlying etiology is self-limited (e.g., metabolic disturbance corrected, transient) and the neonate is seizure-free for 72 hours with normal/normalizing EEG background - wean and stop ASMs before discharge
- If seizures were due to a significant structural injury (HIE, large stroke, cortical malformation) or refractory - continue on phenobarbital maintenance at discharge with outpatient follow-up
- Avoid prolonged, unnecessary anticonvulsant use due to neurotoxicity concerns in animal models (phenobarbital causes neuroapoptosis in developing brain)
Monitoring approach post-discharge:
- EEG at 4-6 weeks if discharged on medications
- Neurodevelopmental follow-up at 3, 6, 12, 18, 24 months
Prognosis
The major determinant of prognosis is the underlying etiology, not the seizures per se:
| Etiology | Approximate Mortality / Disability |
|---|---|
| Transient metabolic (hypoglycemia, hypocalcemia) | Excellent if corrected promptly |
| Benign familial neonatal seizures | Excellent |
| Mild-moderate HIE (with cooling) | 20-30% neurodevelopmental impairment |
| Severe HIE | 50-70% death or major disability |
| Meningitis/Encephalitis | Variable (30-50% adverse) |
| Major structural malformations | Poor |
- 25-70% of survivors with neonatal seizures go on to develop post-neonatal epilepsy
- Risk factors for post-neonatal epilepsy: status epilepticus, refractory seizures >48 hours, extensive brain injury on MRI, severe background suppression on EEG
Summary: AIIMS-Style Quick Protocol Card
NEONATAL SEIZURE - MANAGEMENT PROTOCOL
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
1. ABC stabilization + IV access + SpO2 + cardiac monitoring
2. STAT: BSL, Ca, Mg, Na (correct any abnormality immediately)
3. EEG/aEEG monitoring
4. Sepsis workup + empiric antibiotics (Amp + Gent) + Acyclovir if HSV suspected
DRUG SEQUENCE:
━━━━━━━━━━━━━
→ PHENOBARBITAL 20 mg/kg IV (1st line)
↓ Seizures persist at 15-30 min
→ PHENOBARBITAL 10 mg/kg IV (additional dose)
↓ Seizures persist
→ FOSPHENYTOIN 20 mg/kg IV OR LEVETIRACETAM 60 mg/kg IV (2nd line)
↓ Refractory seizures
→ MIDAZOLAM infusion (0.15 mg/kg bolus + 2 mcg/kg/min)
↓ Still refractory + unknown etiology
→ PYRIDOXINE 50-100 mg IV (during EEG monitoring)
± PLP 10 mg/kg q8h ± Folinic acid 5 mg/kg/day
ETIOLOGY-SPECIFIC:
HIE → Therapeutic hypothermia within 6 hours (≥36 wks)
Infection → Amp + Gent + Acyclovir
IEM → Genetics consult + specific Rx
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Key references:
- Bradley and Daroff's Neurology in Clinical Practice (Ch. 110 - Neonatal Seizures, pp. 2854-2860)
- Volpe JJ - Neurology of the Newborn (seizure classification, pathophysiology)
- Cloherty JP - Manual of Neonatal Care (AIIMS and NNF India protocols align with Cloherty recommendations)
- Nelson - Textbook of Pediatrics (etiology, approach to management)
- ILAE Task Force 2023 guidelines (Pressler et al., Epilepsia 2023 - PMID: 37655702): Systematic review confirming phenobarbital as first-line; levetiracetam as acceptable second-line
- Cochrane Review 2023 on anti-seizure medications for neonatal seizures (PMID: 37873971)
Note: The library does not include Cloherty's Manual of Neonatal Care or Nelson's Textbook directly, but the content above is cross-referenced with these texts' standard teaching and consistent with the AIIMS/NNF India neonatology protocols. The drug protocol above reflects what is taught in AIIMS and endorsed by NNF India.
This is a shared conversation. Sign in to Orris to start your own chat.