Trichilemmal cyst
Reading File
Finding Sources
Finding Sources
Searching PubMed
trichilemmal cyst
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Trichilemmal Cyst (Pilar Cyst / Wen)
Synonyms
- Pilar cyst
- Wen
- Isthmus–catagen cyst
Origin & Pathogenesis
Trichilemmal cysts arise from the outer root sheath (ORS) of the hair follicle, specifically from the epithelium located between the orifice of the sebaceous gland and the arrector pili muscle. This squamous epithelium undergoes rapid keratinization, forming a wall that lacks a granular layer — the defining histologic feature.
Epidemiology
- Present in 5–10% of the general population
- Predominantly affect middle-aged women
- ~60% of patients with hereditary forms are women over age 60
- Autosomal dominant inheritance linked to chromosome 3p (germline variant in PLCD1, encoding phospholipase C delta 1α)
- Most patients have multiple lesions; 10% have >10 lesions
Clinical Features
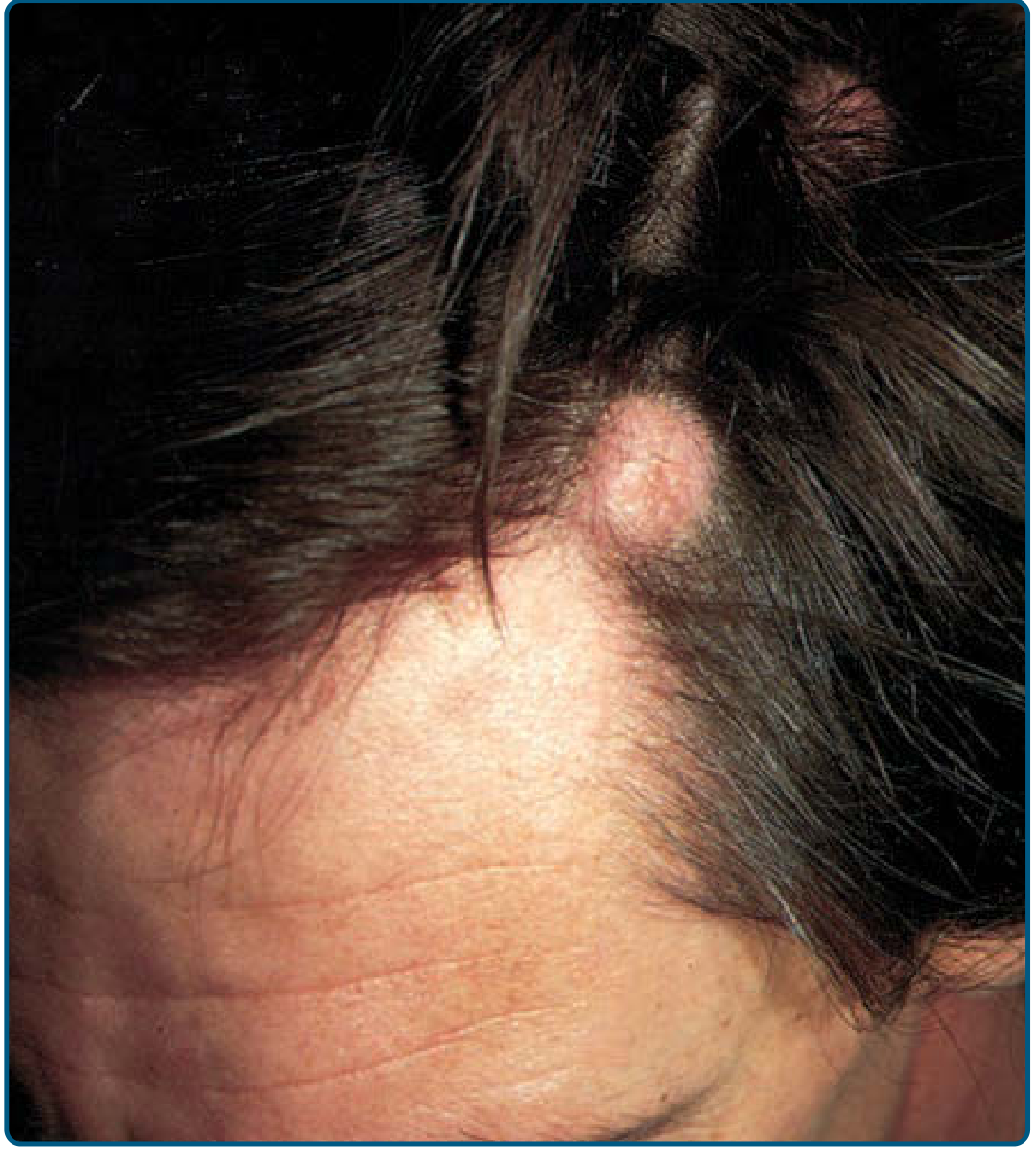
Trichilemmal (pilar) cyst: mobile, firm nodule at the scalp hairline
| Feature | Detail |
|---|---|
| Location | 90% on the scalp (also face, neck, trunk, extremities) |
| Morphology | Mobile, firm, well-circumscribed, smooth-surfaced nodule |
| Punctum | Absent (distinguishes from epidermoid cyst) |
| Consistency | Firmer and more mobile than epidermoid cysts |
| Usually | Asymptomatic; may rupture → inflammation/infection |
| Rapid growth | Abnormal — suggests infection or malignant transformation |
Histopathology
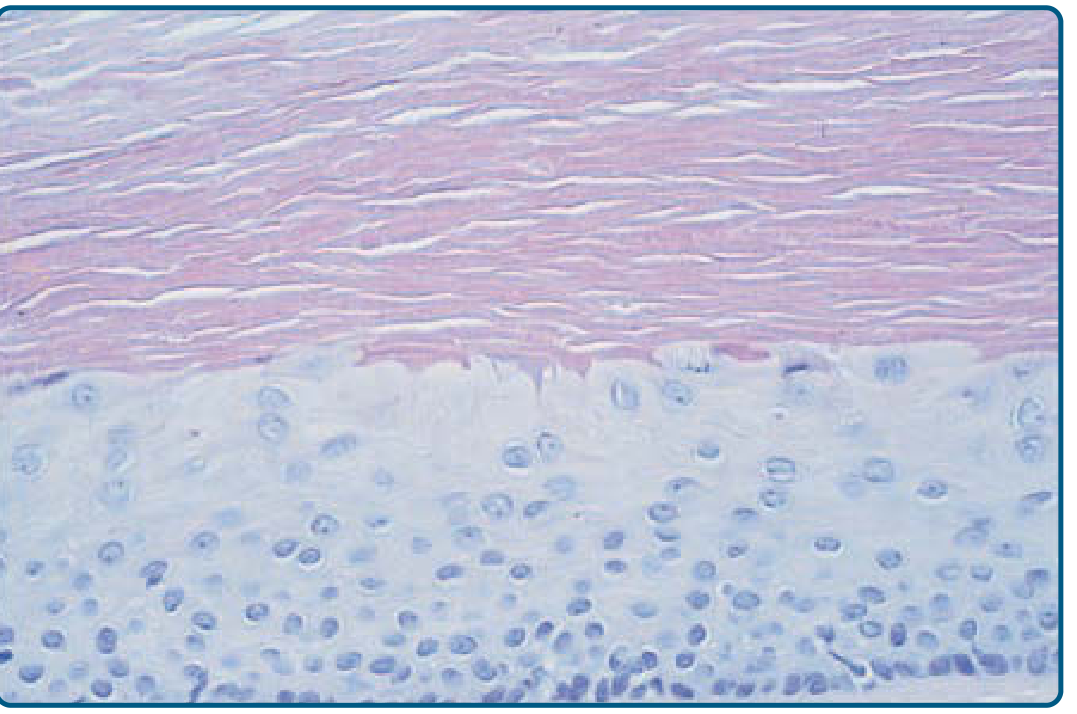
Histology: swollen outer-root-sheath keratinocytes with abrupt keratinization and no granular layer. Compact eosinophilic keratin fills the cyst lumen.
Key microscopic findings:
- No granular layer (trichilemmal keratinization)
- Lining cells swell and become pale near the cavity, then abruptly keratinize
- Contents: homogeneous eosinophilic keratin (compact, not lamellar)
- Calcification common; ossification rare
- Hybrid cysts (combined epidermoid + pilar features) occur
Differential Diagnosis
| Entity | Distinguishing point |
|---|---|
| Epidermoid cyst | Punctum present; granular layer present; usually non-scalp |
| Dermoid cyst | Midline, deeper, may have adnexal structures |
| Lipoma | Soft, lobulated, compressible |
| Alopecic/aseptic nodules of scalp | Ruptured pilar cysts can mimic these |
Spectrum of Proliferating / Malignant Forms
Proliferating Trichilemmal Cyst (Proliferating Pilar Tumor)
- First described by Jones (1966) as "proliferating epidermoid cyst"
- Large (up to 25 cm) exophytic neoplasm, confined almost exclusively to scalp and back of neck
- ~5× more common in women; mean age 65 years
- Gradually enlarges, may ulcerate
- Composed of squamous cells with trichilemmal differentiation forming scroll-like structures/small cysts
- Focal cellular atypia, mitoses, and necrosis may be present but do not necessarily predict aggressive behavior
- Vast majority cured by local excision; may recur; rarely locally aggressive
Malignant Proliferating Trichilemmal (Pilar) Tumor
- Frankly invasive SCC-like areas within a proliferating pilar tumor
- Characterized by: increased cellularity, cytologic atypia, frequent mitoses, stromal invasion
- Immunohistochemistry: express hair cytokeratins (CK7); malignant forms express CD34 (fetal hair root phenotype)
- Red flags for aggressive behavior: non-scalp location, recent rapid growth, size >5 cm, infiltrative growth pattern
- In KID syndrome (keratosis–ichthyosis–deafness), malignant proliferating pilar tumor can develop in young adulthood and may be fatal
Treatment
| Lesion | Management |
|---|---|
| Benign trichilemmal cyst | Surgical excision; easily enucleated through a small incision (cyst wall less adherent than epidermoid cyst); a dermal punch trephine technique is effective |
| Proliferating pilar tumor | Local excision (curative in vast majority) |
| Malignant proliferating pilar tumor | Wide local excision; Mohs surgery may be considered (see PMID 41081546) |
Practical tip: Pilar cysts tend to "deliver" themselves cleanly through an incision without rupture — easier enucleation than epidermoid cysts — which often allows intraoperative diagnosis.
Recent Evidence
A 2025 systematic review (PMID 39539041) characterized the clinical and genomic profiles of malignant proliferating trichilemmal tumors, and a 2026 systematic review (PMID 41081546) examined Mohs micrographic surgery for benign adnexal tumors including trichilemmal lesions — these do not substantially alter the established management approach above.
Sources: Fitzpatrick's Dermatology (8e), Andrews' Diseases of the Skin, Dermatology 2-Volume Set (5e)
This is a shared conversation. Sign in to Orris to start your own chat.